Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
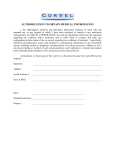
Health Services 102 HPER 6001 Dodge Street Omaha NE 68182 402-554-2374 InformedConsentforMedicalExaminationandTreatment Byreadingandsigningthisdocument,I,theundersignedpatient(orauthorizedrepresentative)consenttoandauthorizethe performanceofanytreatments,examinations,medications,anesthesia,medicalservices,andsurgicalordiagnosticprocedures (includingbutnotlimitedtotheuseoflabandradiographicstudies)asorderedorapprovedbymyattendingphysician(s),orany healthcareprofessionalassignedtomycarebymyattendingphysician(s),andIacknowledgeandconsenttothefollowing: 1. Duringthecourseofmycareandtreatment,Iunderstandthatvarioustypesofexaminations,tests,diagnosticortreatment procedures(“procedures”)maybenecessary.Theseproceduresmaybeperformedbyphysician(s),nurses,technicians, nursepractitioners,orotherhealthcareprofessionals.Whileroutinelyperformedwithoutincident,theremaybematerial risksassociatedwiththeseprocedures.IfIhaveanyquestionsconcerningtheseprocedures,Iwillaskmyphysician(s)to providemewithadditionalinformation.IalsounderstandmyphysicianmayaskmetosignadditionalInformedConsent documentsrelatingtospecificprocedures. 2. NOGUARANTEEOFRESULTS:UNOHealthServicesphysiciansandhealthcareprofessionalscannotguaranteeanyspecific result(s)ofanyexamination,treatment,procedureormedicalcare. 3. IunderstandthatIcanchangemymindregardingtheprocedureortreatment.IfIdo,Imusttellthepersonortheteam doingtheprocedureortreatmentbeforetheystart. 4. Iunderstandthatthehealthcareprofessionalsinvolvedinmycarewillrelyonmydocumentedmedicalhistory,aswellas otherinformationprovidedbyme,myimmediatefamily,orothershavinginformationaboutme,indeterminingwhether toperformorrecommendprocedures.Iagreetoprovideaccurateandthoroughinformationregardingmymedicalhistory andanyconditionsoreventswhichmayimpactmedicaldecision-making. 5. Iunderstandthattheclinic,asrequiredbylaw,mustreportcertaindiseasestolocalandstateagencies. 6. Iunderstandthatstudentsandothersmayobservetheprocedureortreatmentforeducationalpurposes.Observersmust beapprovedbythisfacility. Bysigningthisdocument,IcertifythatIhavereadandunderstanditscontentsandthatinformationprovidedbymeisaccurateand complete(includinginsuranceinformationandcurrenteligibilityforbenefits).Acopyofthisdocumentmaybeutilizedthesameas theoriginal.IfurtheracknowledgereceiptoftheNoticeofPrivacyPracticesofUNOHealthServicesatthisvisitoratapreviousvisit. PrintedName:________________________________________DateofBirth:_____________NUID#_____________________ PatientSignature:____________________________________________________________________Date:_____/_____/______ Parent/Guardianmustsignbelowforpatientsundertheageof19: IcertifythatIhavereadandunderstandthisdocument.IauthorizeUniversityofNebraska-OmahaHealthServicesand/or CounselingandPsychologicalServices(CAPS)toprovidemedicaltreatment,mentalhealthand/orsubstanceusetreatmenttomy child: NameofMinorChild:_________________________________________________MinorChild’sDateofBirth:____/____/______ Parent/GuardianNamePrinted:__________________________________________________Relationship:□Parent□Guardian Parent/GuardianSignature:______________________________________________________Date:_____/_____/_______ Revised5/3/2016