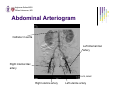
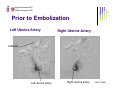
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
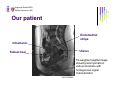
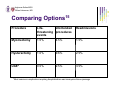
Arghavan Salles MSIV Gillian Lieberman, MD Uterine Artery Embolization Arghavan Salles Advanced Radiology September 15, 2005 Arghavan Salles MSIV Gillian Lieberman, MD Overview I. II. III. IV. V. VI. VII. VIII. Case presentation Imaging and leiomyomata Classification of leiomyomata Selection for UAE UAE technique Post-procedural care and complications Further investigations References Arghavan Salles MSIV Gillian Lieberman, MD History z z z Uterine artery embolizations (UAE, also known as uterine fibroid embolization, UFE) have been performed since the 1970s for hemostasis in women post-partum, post-cesarean, post-abortion, posthysterectomy1-3 It has also been used to treat arteriovenous malformations of the pelvis, placenta previa, and placenta accreta In 1995, Ravina and Herbreteau1 were the first to report the use of UAE for treatment of leiomyomata after having incidentally noted shrinkage of fibroids when using UAE for the above indications Arghavan Salles MSIV Gillian Lieberman, MD Case z z z z z z 46 year old woman with menorrhagia Up to 24 consecutive days of menstruation per cycle Also feels abdominal pressure Past medical and surgical history noncontributory Ultrasound revealed fibroids prior to consultation with the interventionalist Pap smear and endometrial biopsy WNL Arghavan Salles MSIV Gillian Lieberman, MD Work-up of Patients for UAE4 z General medical history and physical examination -important to ask about symptoms, pregnancy history, recent Pap smears, and infection as part of complete history z Gynecologic examination -important to rule out other causes for symptoms z Laboratory testing -typically order CBC, PT/PTT/INR, BUN/creatinine to assess for anemia, coagulopathy, renal insufficiency z Imaging -Ultrasound or MRI z Pap test Arghavan Salles MSIV Gillian Lieberman, MD Epidemiology of Leiomyomata z z z z z z Occur in 20-40% of women of reproductive age4,5 Account for 30-70% of hysterectomies in the United States4-5 Most common benign indication for hysterectomy3 20-50% of women with leiomyomata have menorrhagia, dysmenorrhea, pelvic pressure, urinary frequency, pain, infertility, or a palpable abdominal-pelvic mass4,8 Most common symptoms are heavy menstrual bleeding (78%), pain (59-75%), and bulk-related (82-98%)4,7,9 Occur most often and at a younger age and larger size of lesions in black women7 Arghavan Salles MSIV Gillian Lieberman, MD Differential Diagnosis10 It is important to exclude other pelvic pathology that may be contributing to the patient’s symptoms in order to determine whether UAE is appropriate. z Diffuse adenomyosis (ectopic endometrial glands and stroma within the myometrium) -symptoms are often similar to those resulting from leiomyomata z Focal adenomyosis (adenomyoma) -may be distinguished from leiomyomata on MRI11 Arghavan Salles MSIV Gillian Lieberman, MD Differential Diagnosis, cont. z z Solid adnexal mass Focal myometrial contraction -transient phenomenon that mimics leiomyomata and disappears with repeat imaging z Uterine leiomyosarcoma -often difficult to distinguish on imaging studies -in over 1400 patients who had hysterectomy for presumed leiomyomata followed for five years, 0.49% had leiomyosarcoma12 Arghavan Salles MSIV Gillian Lieberman, MD MRI for Pre-operative Planning z MR is the most accurate imaging technique for detection and localization of leiomyomata for preoperative planning2,4,9,10,12-14 -Ultrasound may be used but is less accurate, especially in obese patients z z z MR is 90% sensitive and specific for adenomyosis11 Treatment options vary depending on characterization of lesions (see Treatment Options) Important to determine depth of extension into myometrium to minimize risk of uterine perforation for anticipated hysteroscopic resections10 Arghavan Salles MSIV Gillian Lieberman, MD MRI for Pre-operative Planning, cont. z Pedunculated subserosal and submucosal leiomyomata may detach from the uterus after UAE -pedunculated subserosal leiomyomata may settle into the pelvis becoming a nidus of infection -pedunculated submucosal leiomyomata may be passed or may become lodged in the cervix or vagina becoming a nidus of infection10 z z z Uterine arteries seen with MRA may help guide embolization10 MRA may help exclude contributions to the leiomyomata from ovarian or other vessels10 MRI may help predict post-procedural outcome12 Arghavan Salles MSIV Gillian Lieberman, MD Effect of MRI on Diagnosis14 z z z z z Interventional radiologists were asked to give pre-imaging and post-imaging diagnoses and treatment plans for 60 women evaluated for UAE Axial HASTE, Axial GRE, Sagittal T2 TSE, and coronal SHARP series were used Initial diagnoses changed in 18% of cases MRI detected unsuspected pelvic masses, demonstrated adenomyosis, detected degenerated fibroids, and documented lack of pelvic pathology Changed treatment plans in 22% of cases -57/60 were to undergo UAE prior to imaging -After MR, 8 went to surgery, 2 had clinical management, and one had biopsy Arghavan Salles MSIV Gillian Lieberman, MD MRI Characteristics z z Nondegenerated uterine leiomyomata are well-circumscribed masses with homogeneously decreased signal intensity compared to the outer myometrium on T2weighted images10 Cellular leiomyomas may have higher signal intensity on T2-weighted images and enhance post-contrast10 Arghavan Salles MSIV Gillian Lieberman, MD MRI Characteristics, cont. z Degenerated leiomyomata have variable appearances depending on the type of degeneration10 -hyaline or calcific degeneration has low signal on T2-weighted images -Cystic degeneration has high signal on T2-weighted images. Cystic areas do not enhance post-contrast. -Myxoid degeneration has very high signal on T2-weighted images and may enhance minimally post-contrast. -Necrotic lesions have variable intensity on T1-weight images and have low signal on T2-weighted images. z It is important to assess enhancement because lesions that do not enhance are not as likely to respond well to embolization Arghavan Salles MSIV Gillian Lieberman, MD MRI Characteristics, cont. Don’t forget our differential diagnoses: z Focal myometrial contraction -low signal on T2-weighted images11 z Adenomyosis -low myometrial signal intensity, enlarged junctional zone* (>12 mm), high signal intensity foci (myometrial cysts), poor definition of endomyometrial junction, and poor definition of lesion borders11 z Adenomyoma -focal thickening of junctional zone, poorly defined margins, minimal mass effect11 *junctional zone is between the endometrium and myometrium and consists mostly of smooth muscle Arghavan Salles MSIV Gillian Lieberman, MD Normal Uterus Endometrial stripe Uterus Bladder Cervix Vagina T2-weighted sagittal image PACS, BIDMC Arghavan Salles MSIV Gillian Lieberman, MD Our patient Endometrial stripe Intramural Uterus Subserosal T2-weighted sagittal image showing leiomyomata in various locations with homogenous signal characteristics PACS, BIDMC Arghavan Salles MSIV Gillian Lieberman, MD Our patient Endometrial stripe Intramural Uterus T2-weighted axial image of the same patient PACS, BIDMC Arghavan Salles MSIV Gillian Lieberman, MD Vasculature Enhancement PACS, BIDMC T1-weighted post-contrast image in the same patient showing enhancement of leiomyomata with dilated uterine arteries (white arrows) Arghavan Salles MSIV Gillian Lieberman, MD Classification of Leiomyomata10 Most commonly occur in the myometrium of the uterus but may occur in cervix (8% of the time) z Submucosal z -project into endometrial canal -least common subtype but most often symptomatic z Intramural -within myometrium -most common subtype, usually asymptomatic z Subserosal -beneath the serosa -if pedunculated, may torse and cause pain or infection Ghai, et al. Arghavan Salles MSIV Gillian Lieberman, MD Examples of Leiomyomata Subserosal Adenomyosis (junctional zone measures ~15 mm) Intramural Submucosal T2-weighted sagittal image PACS, BIDMC Arghavan Salles MSIV Gillian Lieberman, MD More examples Endometrial Submucosal stripe T2-weighted sagittal image Intramural Endometrial stripe T2-weighted sagittal image PACS, BIDMC Arghavan Salles MSIV Gillian Lieberman, MD Enhancement Leiomyoma Enhancement T1-weighted axial image prior to administration of contrast showing homogeneous low signal in leiomyomata T1-weighted axial image after administration of contrast showing enhancement of leiomyoma PACS, BIDMC Arghavan Salles MSIV Gillian Lieberman, MD Indications for Intervention10 z Bleeding -most frequent symptom, usually manifests as menorrhagia or menometrorrhagia -menstrual irregularities may be due to loss of symmetric uterine contractions z Pressure on adjacent organs -mass effect on the bladder may cause urinary frequency or incontinence -may cause hydroureter or hydronephrosis if impinging on the ureter -may cause constipation due to effects on the rectum Arghavan Salles MSIV Gillian Lieberman, MD Indications for Intervention, cont. z Pain -usually due to acute degeneration which can often occur during pregnancy -may be secondary to torsion of subserosal lesions or prolapse of submucosal lesions z Infertility -may occur as a result of compression of the fallopian tubes from intramural leiomyomata in the cornual regions or intraligamentous regions -may be a result of faulty implantation due to submucosal lesions Arghavan Salles MSIV Gillian Lieberman, MD Treatment Options10 z Medical Management -GnRH inhibits the secretion of gonadotropinsÆhypoestrogenic stateÆamenorrheaÆdecreased size of fibroids/uterus -regrowth if stop treatment -risk osteoporosis -may use pre-operatively prior to hysterectomy, myomectomy, or hysteroscopic myomectomy z Hysterectomy -traditional option, does not preserve fertility z Myolysis -neodymium:yttrium-aluminum-garnet laser or bipolar needle electrodes -thermal injury leads to degeneration -may also lead to pelvic adhesions Arghavan Salles MSIV Gillian Lieberman, MD Treatment Options, cont. z Myomectomy -enucleation of leiomyoma with preservation of uterus -can be performed open, hysteroscopically, laparoscopically -risk of recurrence is 27% at 10 years10, 10% at 5 years6 Hysteroscopic: -60% rate of pregnancy after hysteroscopic myomectomy10 -appropriate for submucosal or submucosal-intramural leiomyomata -risk of uterine perforation Laparoscopic: -appropriate for pedunculated subserosal leiomyomata z Uterine Artery Embolization -inject various particles into uterine artery to achieve stasis -may preserve fertility (see Fertility? slides) Arghavan Salles MSIV Gillian Lieberman, MD Comparing Options15 z z 400 consecutive patients were followed after UAE Complications were categorized using two classification systems: -Society of Cardiovascular and Interventional Radiology -American College of Obstetricians and Gynecologists z Date on complications over the first 30 days were reported Arghavan Salles MSIV Gillian Lieberman, MD Comparing Options15 Procedure LifeUnintended threatening procedures events Readmissions Myomectomy 1.5% 4.5% 1.5% Hysterectomy 1.0% 9.6% 2.5% UAE* 0.5% 2.5% 3.5% *Most common complication requiring hospitalization was leiomyoma tissue passage Arghavan Salles MSIV Gillian Lieberman, MD Selection for UAE4 z z z Symptomatic leiomyomata Exclusion of those who are pregnant, have a pelvic malignancy, or have active pelvic infection Patient choice Arghavan Salles MSIV Gillian Lieberman, MD Relative Contraindications to UAE2,4 z z z z z z z z Coagulopathy Severe allergy to contrast material Renal impairment Immunocompromised Previous pelvic irradiation or surgery Chronic endometritis Strong desire for future fertility Suberosal pedunculated lesions (usually safe if the attachment to the uterus spans more than 50% of the diameter of a subserosal lesion) Arghavan Salles MSIV Gillian Lieberman, MD Seldinger Technique16 z z z z z z Technique used for interventional procedures Insert needle Insert wire through needle Enlarge skin incision Exchange needle for sheath and dilator Remove dilator and use sheath Arghavan Salles MSIV Gillian Lieberman, MD Vascular Anatomy17 Arghavan Salles MSIV Gillian Lieberman, MD Angiographic Safety z Minimize radiation dose to the patient during all interventional procedures2,3 -collimate images -small gap between patient and image intensifier -take as few images as possible Arghavan Salles MSIV Gillian Lieberman, MD UAE Technique: I 4,15 z z Usually unilateral femoral approach using 4 or 5 French catheter Perform abdominal arteriogram with digital subtraction with ileofemoral run-off to visual vessels -assess for arteriovenous malformations, shunting, collateral vessels (ovarian, round ligament, cervical, pelvic) Arghavan Salles MSIV Gillian Lieberman, MD Abdominal Arteriogram Catheter in aorta Left internal iliac artery Right internal iliac artery PACS, BIDMC Right uterine artery Left uterine artery Arghavan Salles MSIV Gillian Lieberman, MD UAE Technique: II z Then perform arteriogram from both internal iliac vessels using Bookstein catheter18 -vascular supply to leiomyomata often comes from both uterine arteries so both are embolized z Access uterine arteries using Tracker catheter and perform arteriogram Arghavan Salles MSIV Gillian Lieberman, MD Prior to Embolization Left Uterine Artery Right Uterine Artery Catheter Left uterine artery Right uterine artery PACS, BIDMC Arghavan Salles MSIV Gillian Lieberman, MD UAE Technique: III z z z z Inject embolization agent of choice Target is distal occlusion of arteries feeding leiomyomata End-point is usually complete occlusion of vessels Access both uterine arteries and perform arteriogram again to demonstrate decreased flow Arghavan Salles MSIV Gillian Lieberman, MD Embolization Materials z z z z Polyvinyl alcohol (usually 355-500 microns) Tris-acryl gelatin microspheres Gelatin sponge particles Must avoid vasospasm for adequate delivery of particles9 -may use nitroglycerin to treat vasospasm Arghavan Salles MSIV Gillian Lieberman, MD After embolization Left Internal Iliac Artery Right Internal Iliac Artery Catheter Right uterine artery—occluded Left uterine artery—occluded PACS, BIDMC Arghavan Salles MSIV Gillian Lieberman, MD Consequences of UAE5 z z Myoma necrosis Reduced uterine volume -most decrease may occur within the first six months although further decrease occurs after that12,13 z z Improved menorrhagia Decreased pelvic pain Arghavan Salles MSIV Gillian Lieberman, MD Efficacy of UAE z z z z z z z z z z z Return to work after 17 days9 Usually feel better within 1 week2,3 83-84% noted improved menorrhagia9,13 86% improved urinary frequency/urgency13 79% improved pain9 Decreased duration of menstruation (7.6 to 5.4 days)13 82% had decreased bloating or swelling9 91-97% satisfied with the procedure9,13 Average shrinkage of fibroids by 42-73%9,13 Average shrinkage of uterine volume 35%13 May be less effective for pedunculated subserosal leiomyomata because these may have an alternate blood supply from ovarian arteries or from other organs to which they may be attached12 Arghavan Salles MSIV Gillian Lieberman, MD Efficacy, cont. z z z z z Control symptoms in 80-94% of women9 Most effective in those with high blood flow or high cellularity3 Some women go on to have normal pregnancies7 Failure rates 4-21%13 Amenorrhea 2-15%13 -thought to be due to decreased uterine vascularity, inadvertent occlusion of ovarian vessels, or possible effect of radiation z Ovarian collateral supply, unrecognized malignancy, misdiagnosis of adenomyosis, underembolization may all lead to treatment failure4,13 Arghavan Salles MSIV Gillian Lieberman, MD Complications3,15 Based on two separate studies of 400 women in each study: z Febrile morbidity (2%) -post-embolization fever is common within the first few postprocedural days z z z Hemorrhage (0.75%) Unintended procedure (2.5%) Life-threatening events (0.5%) -pulmonary embolus -one case of septic shock Arghavan Salles MSIV Gillian Lieberman, MD Complications, cont. z Readmission (3.5%) -infection was most likely to occur in women with large fibroids or pedunculated subserosal fibroids z z z Overall morbidity (5%) Fibrosis of uterus (rare) Premature ovarian failure, infections, uterine discharge, necrosis, death from sepsis Arghavan Salles MSIV Gillian Lieberman, MD Periprocedural Concerns z z z z z Usually conscious sedation is used during the procedure Some may give antibiotics, but there is no consensus on what to use Important to monitor patient’s radiation dose Most interventionalists admit the patients for a short stay Pain -most women experience severe pain which is worst in the first 24 hours -may discharge most patients post-procedural day 1 with adequate medication and follow-up z Nausea -second most common complaint post-procedure Arghavan Salles MSIV Gillian Lieberman, MD Post-procedural Care4 z z Follow-up phone call within 24-48 hours to monitor pain/nausea control If patient develops temperature more than four days after the procedure or has increasing pain, should be readmitted9 -should then obtain blood cultures, urinalysis/urine culture, CBC, vaginal swabs, MRI -start on antibiotics z Office visit 1-3 weeks after procedure -assess symptoms, healing z z Imaging 3-6 months after procedure Long-term follow-up necessary -check for infections, expulsion of materials, chronic endometritis, chronic vaginal discharge, irregular menses, amenorrhea which may all develop more than one year after the procedure Arghavan Salles MSIV Gillian Lieberman, MD MR Monitoring: 1/3/05 Pre-embolization, T2-weighted axial image showing large intramural fibroids Pre-embolization, Post-gadolinium T1weighted image shows the lesions are avidly enhancing. PACS, BIDMC Arghavan Salles MSIV Gillian Lieberman, MD MR Monitoring: Successful Embolization Axial T1 pre-contrast (LAVA) Axial T1 post-contrast (LAVA) Patient had embolization 2/11/05. These images were acquired 3/8/05. Uterine size prior to embolization was 25 cmx15 cmx9.4 cm and is now 13.6 cmx8.4 cmx9.3 cm. Large intramural fibroid was 7 cmx4.7 cmx5.3 cm and now is 5.3 cmx6.0 cmx5.6 cm. On post-contrast images, the mass is now devascularized. PACS, BIDMC Arghavan Salles MSIV Gillian Lieberman, MD Questions z z Is UAE effective in treating patients with adenomyosis? Does UAE preserve fertility? Arghavan Salles MSIV Gillian Lieberman, MD Adenomyosis z z z z The efficacy is UAE in patients with adenomyosis is difficult to assess as most patients with adenomyosis also have leiomyomata There is currently one study following women with symptomatic adenomyosis without leiomyomata11 Results thus far indicate that 55% of patients show clinical improvement 2 years after UAE11 Most patients with both leiomyomata and adenomyosis are treated with UAE because it is difficult to definitively attribute their symptoms to one or the other Arghavan Salles MSIV Gillian Lieberman, MD Fertility? z z z It is unclear whether UAE preserves fertility in women Some series have included women who have gone on to have normal pregnancies (12 patients in a series of 400 women9)1 Amenorrhea after UAE is often transient due to decreased uterine vascularity Arghavan Salles MSIV Gillian Lieberman, MD Fertility?, cont. z The rate of amenorrhea after the procedure is significantly higher in older women -3% in women under age 4013 -41% in women age 50 or older13 -2% under age 4515 -rate of ovarian failure in the general population is 4% under age 4515 z Amenorrhea may be attributed to: -transient decreased uterine vascularity -anastomoses between uterine and ovarian arteries causing embolization materials to inadvertently decrease vascular supply to the ovaries13 Arghavan Salles MSIV Gillian Lieberman, MD Conclusion z z z z z UAE has fewer complications than other interventions9,15 Minimally invasive, safe way to treat uterine leiomyomata Shorter hospital stay and reduced cost compared to surgical treatment8,9 Has been shown to be more cost-effective than hysterectomy19 Adenomyosis and fertility need to be further investigated Arghavan Salles MSIV Gillian Lieberman, MD References 1. Ravina JH, Herbreteau D. Arterial embolisation to treat uterine myomata. Lancet 1995;346:671-2. 2. Goodwin SC, Wong GCH. Uterine artery embolization for uterine fibroids: A radiologist’s perspective. Clin Ob Gyn 2001;44:412-424. 3. Zupi E, Pocek M, Dauri M, et al. Selective uterine artery embolization in the management of uterine myomas. Fertil Steril 2002;79:107-111. 4. Andrews RT, Spies JB, Sacks D, et al. Patient care and uterine artery embolization for leiomyomata. J Vasc Interv Radiol 2004;15:115-120. 5. Kjerulff KH, Erickson AB, Langerberg PW. Chronic gynecologic conditions reported by US women: Findings from the National Health Interview Survey, 1984 to 1992. Am J Public Health 1996;86:195-6. 6. Broder MS, Goodwin S, Chen G, et al. Comparison of long-term outcomes of myomectomy and uterine artery embolization. Ob Gyn 2002;100:864-8. 7. Pron G, Cohen M, Soucie J, et al. The Ontario uterine fibroid embolization trial. Part 1. Baseline patient characteristics, fibroid burden, and impact on life. Fertil Steril 2003;79:112-9. 8. Buttram VC Jr, Reiter RC. Uterine leiomyomata: etiology, symptomatology, and management. Fertil Steril 1981;36:433-445. Arghavan Salles MSIV Gillian Lieberman, MD References, cont. 9. Walker WJ, Pelage JP. Uterine artery embolization for symptomatic fibroids: clinical results in 400 women with imaging follow up. BJOG 2002;109:12621272. 10. Murase E, Siegelman ES, Outwater EK, et al. Uterine leiomyomas: Histopathologic features, MR imaging findings, differential diagnosis, and treatment. RadioGraphics 1999;19:1179-1197. 11. Pelage JP, Jacob D, Fazel A, et al. Midterm results of uterine artery embolization for symptomatic adenomyosis: Initial experience. Radiology 2005;234:948-953. 12. Ghai S, Rajan DK, Benjamin MS, et al. Uterine artery embolization for leiomyomas: Pre- and postprocedural evaluation with US. RadioGraphics 2005;25:1159-1176. 13. Pron G, Bennett J, Common A, et al. The Ontario uterine fibroid embolization trial. Part 2. Uterine fibroid reduction and symptom relief after uterine artery embolization for fibroids. Fertil Steril 79:120-7. 14. Omary RA, Vasireddy S, Chrisman HB, et al. The effect of pelvic MR imaging on the diagnosis and treatment of women with presumed symptomatic uterine fibroids. J Vasc Interv Radiol 2002;13:1149-1153. Arghavan Salles MSIV Gillian Lieberman, MD References, cont. 15. Spies JB, Spector A, Roth AR, et al. Complications after uterine artery embolization for leiomyomas. OB Gyn 2002;100:873-880. 16. Roberts: Clinical Procedures in Emergency Medicine, 4th ed. 2004 Elsevier. Accessed online 8/13/05. 17. Gray, Henry. Anatomy of the Human Body, 20th Ed. Accessed on bartleby.com 9/13/05. 18. Fellmeth B, Bookstein JJ, Lurie A. Ultralong, reverse-curve angiographic catheter. Radiol 1989;172:872-3. 19. Beinfeld MT, Bosch JL, Isaacson KB, et al. Cost-effectiveness of uterine artery embolization and hysterectomy for uterine fibroids. Radiol 2004;230:207-213.