Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
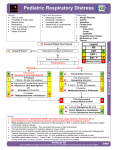
9/18/2014 Sam Delaune, MD Niswonger Children’s Hospital Emergency Department September 19, 2014 Objectives Initial assessment of severity Specific approach to patient based on severity Mild Moderate Severe More aggressive adjuncts Hospitalization Intubation 4:30 pm on a Friday afternoon 6 yo female Known history of asthma URI symptoms and fever for 48 hours Wheezing at home Albuterol via neb machine every 3 hours Still wheezing per mom 1 9/18/2014 Physical HR: 128 BP: 128/54 Wt: 27kg O₂ sat: 90% (on room air) General Moderate respiratory distress Speaking in brief sentences HEENT MMM TMs retracted bilaterally without effusion No conjunctival irritation Cardivascular Mild tachycardia No murmur Well perfused, cap refill 2‐3 seconds Resp Inspiratory / Expiratory wheezing No rales or rhonchi Suprasternal and intercostal retractions GI Abdomen soft, non‐tender Musculoskeletal/Neuro Moving all extremities well No focal neuro deficits Assessment of Severity Multiple objective and subjective factors Vital signs Clinical exam – be sure to take off shirt Asthma history – controller meds, albuterol frequency Admission history – Floor and PICU Regardless, first priority is to improve respiratory status as quickly as possible Mild Intermittent cough Exertional dyspnea Expiratory wheezing, occasionally intermittent Increased use of β agonists, but still with adequate response O₂ sat >95% 2 9/18/2014 Moderate Persistent cough Normal mental status Abbreviated speech Dyspnea at rest Minimal or transient response to β agonist, using more than q4 hours O₂ sat 90‐95% Severe Altered mental status Difficulty speaking Marked respiratory distress Tachycardia No / minimal response to β agonists O₂ sat <89% Our patient Cough Awake and alert Speaking, but with difficulty Dyspnea Some effect from Albuterol, but transient Relative hypoxia at 90% Moderate 3 9/18/2014 Basic treatment outline Β‐agonist first line Albuterol Either nebulized or through MDI with spacer 80% of airway dilation occurs in 5 minutes Continuous vs. back‐to‐back treatments Clinical effectiveness Re‐observation Basic treatment outline Anti‐cholinergic medications Atrovent (Ipratropium bromide) Reduced hospitalization rates Virtually side effect free Corticosteroids Oral vs IV/IM Dosing Prednisone/Prednisolone vs. Dexamethasone Mild ‐ Treatment Aerosolized albuterol 30 kg and under – 2.5 mg neb Over 30 kg – 5 mg neb Oral steroids, typically prednisolone 1‐2 mg/kg, max dose 60 mg Typically, mild will not require O₂ If drop in sat with albuterol, consider chest xray 4 9/18/2014 Moderate – Treatment Aerosolized albuterol 30 kg and under – 2.5 mg neb x 3, given at 20 minute intervals Over 30 kg – 5 mg neb x 3, given at 20 minute intervals Ipratropium Bromide 20 kg and under – 0.25mg x 3, given with albuterol Over 20 kg – 0.5 mg x 3, given with albuterol Or Moderate ‐ Treatment Continuous hour long nebulized treatment 5‐10 kg 10 mg Albuterol + 0.75 mg Ipratropium 10‐20 kg 15 mg Albuterol + 0.75 mg Ipratropium Over 20 kg 20 mg Albuterol + 1.5 mg Ipratropium And Moderate ‐ Treatment Oral steroids if tolerated Prednisolone 1‐2 mg/kg, max 60 mg IV/IM Methylprednisolone 1mg/kg, max 60 mg Oxygen as needed 5 9/18/2014 Severe ‐ Treatment Aerosolized albuterol Continuous hour long nebulized treatment 5‐10 kg 10 mg Albuterol + 0.75 mg Ipratropium 10‐20 kg 15 mg Albuterol + 0.75 mg Ipratropium Over 20 kg 20 mg Albuterol + 1.5 mg Ipratropium Severe ‐ Treatment Corticosteroids IV/IM Methylprednisolone 1mg/kg, max 60 mg Oxygen as needed Resistant cases Epinephrine IM/Sub Q Best in patients with poor inspiratory flow 1:1000 concentration 0.01 mg/kg, max 0.4 mg Magnesium IV 25‐40 mg/kg, run over 20 minutes Will cause hypotension Pair with a bolus Terbutaline Sub Q 0.01 mg/kg, max 0.4 mg Heliox Primarily an ICU modality Mixture of helium and oxygen Decreased resistance in airway 6 9/18/2014 Decision to hospitalize Period of observation History of prior admissions Response to ED management Hypoxia Distance from hospital Intubation Relatively rare RSI if possible Ketamine as induction agent Potent bronchodilator Paralysis only as necessary ED Discharge plans Parental education Controller vs Rescue medications Continued β agonists Every 4 hours Home corticosteroids Prompt follow up with PCP 24‐48 hours Clear reasons to return Albuterol > every 4 hours Difficulty breathing (retractions, head bobbing, grunting/wheezing) 7 9/18/2014 Questions? Disclosure Statement of Financial Interest I, Sam Delaune, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation 8