Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
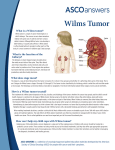
Radiologic Diagnosis of Wilms Tumor Adam Friedman Gillian Lieberman, MD March 2008 Patient presentation • Two year old male with abdominal pain, swelling and constipation. Our patient: RUQ mass on abdominal plain film Study: Abdominal X-Ray Findings: • Dilated large and small bowel, leftward displacement • Soft tissue density in right upper and lower abdomen obscuring lower liver margin Our patient: Heterogeneous mass on ultrasound Study: RUQ ultrasound Findings: • • Heterogeneous, septated, soft tissue mass, 9 x 10 x 6cm, with solid and cystic components (anechoic regions with enhanced throughtransmission). Doppler demonstrates regions of vascular flow in addition to cystic elements Differential diagnosis • • • • Wilms Tumor Neuroblastoma Hepatoblastoma Nephrogenic rests or nephroblastomatosis (multifocal or diffusely bilateral nephroblast remnants) • Other abdominal soft tissue masses: – Rhabdomyosarcoma – Lymphoma – renal cell carcinoma (adults) Our patient: Heterogeneous mass on axial CT mass r. kidney l. kidney Our patient: Heterogeneous mass on coronal CT mass spleen l. kidney r. kidney Our patient: Summary of findings on CT Study: Abdominal CT with oral and IV contrast, late arterial phase Findings: • 10.5 x 9.3 x 12.2 cm cystic heterogeneous mass within the right hemiabdomen, originating from upper/middle poles of kidney • Mass-effect shift of liver • Narrowing and deviation of infrahepatic IVC • “Claw sign” of engulfment by right kidney • No evidence of renal vein or IVC thrombosis • No evidence of pulmonary metastatic disease Diagnosis: Wilms Tumor • Wilms Tumor, with cystic elements and favorable histology. • Stage III due to lymph node metastases and tumor rupture noted intra-operatively, with adherent liver metastases Radiologic features of Wilms Tumor • “Claw Sign”: Concavity of the renal contour with renal parenchyma cupping the tumor/cyst • Clawing suggests organ of tumor origin. • Major differential is neuroblastoma, a neuroendocrine tumor of neural crest origin): • Neuroblastoma: Displacement of kidney, adrenal origin, encasement of IVC/aorta, 90% calcifications • Wilms: Engulfment of kidney, origin from renal parenchyma, displacement of vessels, 15% calcification Neuroblastoma vs. Wilms Tumor companion patient #1 companion patient #2 companion patients #3-4 Neuroblastoma Wilms Tumor Displacement of kidney adrenal origin encasement of IVC/aorta 90% calcifications engulfment of kidney origin from renal parenchyma displacement of vessels 15% calcification Wilms Tumor: embryology, epidemiology, biology • • • • • • • • Derived from remnant rests of embryonic nephroblastic cells Associated with WT1 transcription factor tumor suppressor 6% of all childhood cancers, 1:10,000 incidence, with peak incidence between 2-5 Cure rates ~85% Associated syndromes include (WAGR), Beckwith-Wiedemann, Denys-Drash, horseshoe kidney 5% bilateral, 5% metastatic (lung, lymph nodes, liver); 6% extend into IVC or RV Nephrogenic rests (intralobar or perilobar) increase risk for WT (but only ~1%) Histologically: blastemal, stromal, epithelial cells Wilms Tumor: the role of imaging • Ultrasound: Hypervascular, heterogenous mass • CT: solid, heterogenously enhancing, solitary renal mass (can be bilateral); calcifications in <20% • MRI: Hypointense on T1, hyperintense on T2, with heterogeneous enhancement • CT used for staging due to superior resolution of lung metastases (vs. bone scanning for neuroblastoma) • U/S monitoring of high risk (syndromic) patients every 3-4 mo until 7 yo Wilms Tumor: staging and therapy • Staging: • • • • • I - Unilateral, intact renal capsule, total excision II - Regional tumor extension, total excision III - Residual tumor, confined to abdomen IV - Metastases (lung, liver, bone, brain) V - Bilateral • Treatment: • Nephrectomy (if IVC not involved) • Chemotherapy (vincristine/actinomycin D, +/- doxorubicin, etoposide, carboplatin) • Preoperative chemotherapy in Europe for down-staging, vs. post-op in US. • Radiation (<30%) • Routine U/S monitoring Advanced imaging modalities in Wilms Tumor • 3D MRI tumor perfusion mapping • DWI/ADC MRI mapping • FDG-PET/CT Preoperative 3D mapping of tumor perfusion companion patient #5 • Maximum contrast (absolute) or maximum slope of contrast enhancement during MRI used to correlate areas of necrosis and perfusion of nephroblastomas or neurblastomas for surgical planning. Apparent diffusion coefficient (ADC) mapping companion patient #6 • Contrast-enhanced T1 MRI vs. ADC map • Rim-enhancement and interior architecture prominent with ADC map • ADC mapping may indicate early tumor response, before clear tumor shrinkage (late finding) FDG-PET/CT • • • Companion patient #6 with renal cell carcinoma 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) imaging reveals areas of increased metabolic activity Developing utility in Wilms Tumor: • Targeting biopsy to most aggressive elements • Monitoring treatment response • Identification of metastatic lung foci Summary • • • • • Discussion of 2 y.o. boy with Stage III Wilms Tumor Radiologic diagnosis of WT vs. neuroblastoma Utility of “claw sign” Review of Wilms Tumor embryology, biology Advanced radiologic tools for WT diagnosis and tracking Acknowledgments and References Acknowledgments: • Jay Pahade, M.D. • Gillian Lieberman, M.D. References: • • • • • • • • • Kaste SC, McCarville MB. (2008) “Imaging pediatric abdominal tumors.” Semin Roentgenol., 43(1): 50-9. Günther, P, et al. (2008) “3D Perfusion Mapping and Virtual Surgical Planning in the Treatment of Pediatric Embryonal Abdominal Tumors,” Eur J Pediatr Surg. 18(1):7-12. University Hospitals of Cleveland, www.uhrad.com, 2008. Owens, CM, et al. (2008) “Bilateral disease and new trends in Wilms tumour.” Pediatr Radiol., 38(1): 30-9. Kaste SC, et al. (2008) “Wilms tumour: prognostic factors, staging, therapy and late effects.” Pediatr Radiol., 38(1): 217. Ros, P. (eds), Mortele, K., Pelsser, V., Lee, S. (2007) CT And MRI of the Abdomen And Pelvis: A Teaching File, Lippincott Williams & Wilkins Olsen, OE and Sebire, NJ (2006). “Apparent diffusion coefficient maps of paediatric mass lesions with free-breathing diffusion-weighted magnetic resonance: feasibility study.” Acta Radiol, 47:198–204. Schedl (2007). “Renal abnormalities and their developmental origin.” Nat. Rev. Gen., 8: 791-802. Eubank, WB, et al. (1998). “Imaging of oncologic patients: benefit of combined CT and FDG PET in the diagnosis of malignancy.” AJR Am J Roentgenol., 171(4): 1103-10.