Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
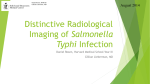
Grant Smith, HMS III Gillian Lieberman, MD March 2012 An Atlas of Complications of ERCP Grant Smith, HMS Year III Dr. Gillian Lieberman, MD Brunicardi FC, Andersen DK, Biliar TR, Dunn DL, Hunter JG, Matthews JB, Polluck, RE: Schwartz’s Principles of Surgery, 9th Edition: http://www.accessmedicine.com Grant Smith, HMS III Gillian Lieberman, MD Teaching Goals 1) 2) 3) 4) Understand how ERCP is performed. Become familiar with the indications for ERCP. Know the common complications of ERCP. Identify the menu of radiologic tests used to diagnose complications of ERCP. 5) Recognize radiologic findings of ERCP complications. 2 Grant Smith, HMS III Gillian Lieberman, MD Endoscopic Retrograde Cholangiopancreatography (ERCP) • ERCP is an endoscopic procedure, in which a specialized side-viewing upper endoscope is guided into the duodenum. • ERCP provides an opportunity for instrumentation to: 1. 2. Perform procedures such as brush cytology, biopsy, sphincterotomy, and stone removal Visualize the biliary tree and pancreatic ducts Brunicardi FC, Andersen DK, Biliar TR, Dunn DL, Hunter JG, Matthews JB, Polluck, RE: Schwartz’s Principles of Surgery, 9th Edition: http://www.accessmedicine.com Abdominal Fluoroscopy during ERCP 3 Grant Smith, HMS III Gillian Lieberman, MD Anatomy of ERCP: Diagram Chandrasoma P, Taylor CR: “Anatomy of the biliary system,” Concise Pathology, 3rd Edition: http://www.accessmedicine.com 4 Grant Smith, HMS III Gillian Lieberman, MD Anatomy of ERCP: Fluoroscopy Endoscope Common Hepatic Duct Gallbladder Cystic Duct Common Bile Duct Pancreatic Duct 2nd Part of Duodenum Ampulla/ Sphincter of Oddi Guntau J. (2006). ERCP: Unauffälliger Gallen- und Pankreasgang, mehrere unterschiedlich große Gallensteine in der Gallenblase und im Gallenblasengang. Endoskopiebilder.de. http://en.wikipedia.org/wiki/File:ERCP_Roentgen .jpgA Abdominal Fluoroscopy during ERCP 5 Grant Smith, HMS III Gillian Lieberman, MD Indications for ERCP NIH Consensus Guidelines & American Society for Gastrointestinal Endoscopy Guidelines – – – – – – – – Diagnosis and treatment of choledocholithiasis Common bile duct (CBD) stone removal after cholecystectomy Pancreatitis or cholangitis secondary to CBD stones Biopsies/Brushings/FNA of suspicious pancreatic masses for tissue diagnosis to initiate chemotherapy and/or radiation Visualization and biopsy of ampullary malignancies Stent placement for bile duct strictures ERCP with sphincter of Oddi manometry for recurrent pancreatitis Drainage of pancreatic pseudocysts 6 Grant Smith, HMS III Gillian Lieberman, MD When ERCP is NOT Appropriate • Asymptomatic cholelithiasis • Acute pancreatitis (unless gallstone pancreatitis is suspected) • Exploration for CBD stones prior to cholecystectomy (when there is a low suspicion for choledocholithiasis) 7 Grant Smith, HMS III Gillian Lieberman, MD Changing Role for ERCP • ERCP has become a modality primarily used for treatment and procedures rather than diagnosis. • Magnetic Resonance Cholangiopancreatography (MRCP) is a non-invasive technique that does not require contrast material to be injected into the biliary tree or pancreatic duct. Greenberger NJ, Blumberg RS, Burakoff R: CURRENT Diagnosis & Treatment: Gastroenterology, Hepatology, & Endoscopy: http://www.accessmedicine.com Abdominal MRI, coronal, heavily-weighted T2 8 Grant Smith, HMS III Gillian Lieberman, MD COMPLICATIONS OF ERCP 9 Grant Smith, HMS III Gillian Lieberman, MD ERCP Complications: A Framework Classification of site, timing, and severity of complications related to ERCP Site Specific Occurring at the point of endoscopic contact or cannulation Nonspecific Occurring in organs not transversed or treated Timing Immediate Occurring during ERCP Early Evident within the recovery period Delayed Specific (occurring within 30 days), Nonspecific (1st symptom within 3 days) Late Evident after months or years Criteria for Severity Mild < or equal to 3 night inpatient stay Moderate 4-10 night inpatient stay Severe > 10 nights, ICU admission, or surgery Fatal Death attributable to procedure within 30 days Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointestinal endoscopy 1991;37(3):383-93. 10 Grant Smith, HMS III Gillian Lieberman, MD Complication Rates Specific complications (pancreatitis, bleeding, sepsis, and perforation) occur in approximately 5.3-6.9% of patients with mortality rate of 0.33-0.34%. Non-specific complications occur in approximately 0.87-1.3% of patients with mortality rate of 0.07%. Specific Complications – – – – – Pancreatitis (4%) Hemorrhage (1%) Cholangitis (1%) Perforation (0.5%) Death (0.1%) Non-Specific Complications – Medication reactions – Oxygen desaturation – Cardiopulmonary events 11 Grant Smith, HMS III Gillian Lieberman, MD Index Patient: Clinical Presentation • 58 year old female presents from OSH 1 day s/p ERCP for choledocholithiasis. • Stones were extracted from the common bile duct and a biliary stent was placed. • A few hours after ERCP, the patient presented with facial swelling, thought to be an allergic reaction. • Later, the patient was noted to have subcutaneous emphysema and transferred to BIDMC for further management. 12 Grant Smith, HMS III Gillian Lieberman, MD Index Patient: Initial CXR Subcutaneous air in cervical area “Gingko Sign” Air between muscle fibers of pectoralis major indicating subcutaneous emphysema Pneumomediastinum BIDMC, PACS Chest X-ray, Portable 13 Grant Smith, HMS III Gillian Lieberman, MD Companion Patient: “Gingko Sign” 37-year-old man 2 weeks after knife wound to chest. “Gingko Sign” seen as air between the muscle fibers of pectoralis major (arrows and stars) indicating subcutaneous emphysema ©2009 by American Roentgen Ray Society Ho M , Gutierrez F R AJR 2009;192:599-612 Chest X-ray, Portable 14 Grant Smith, HMS III Gillian Lieberman, MD Index Patient: Plain Abdominal Film Streaky air surrounding T10, T11, T12, and L1 indicating free air in the abdomen Subcutaneous emphysema Rigler’s Sign (Box) bowel wall etched in white with adjacent lucent line indicating free air in the abdomen (pneumoperitoneum) BIDMC, PACS Abdominal X-ray, Portable, Supine 15 Grant Smith, HMS III Gillian Lieberman, MD Index Patient: Chest CT - Pneumomediastinum and “Ginko Sign” “Ginko Sign” Air separating muscle fibers of pectoralis major Aberrant air in mediastinum indicating pneumomediastinum BIDMC, PACS Chest CT with contrast, axial, lung windows 16 Grant Smith, HMS III Gillian Lieberman, MD Index Patient: Chest CT - Pneumothorax “Ginko Sign” showing air separating muscle fibers of pectoralis major Small pneumothorax Pneumomediastinum BIDMC, PACS Chest CT with contrast, axial, lung windows 17 Grant Smith, HMS III Gillian Lieberman, MD Index Patient: Abdominal CT Pneumoretroperitoneum and Pneumomperitoneum Pneumoperitoneum Subcutaneous Air Pneumoretroperitoneum BIDMC, PACS Abdominal CT with contrast, axial, lung windows 18 Grant Smith, HMS III Gillian Lieberman, MD Index Patient: Abdominal CT Duodenal Diverticulum Duodenal diverticulum Stent BIDMC, PACS Abdominal CT with contrast, axial, abdominal windows 19 Grant Smith, HMS III Gillian Lieberman, MD Index Patient: Abdominal CT - Perforation Extraluminal contrast suggestive of perforation BIDMC, PACS Abdominal CT with contrast, axial, abdominal windows 20 Grant Smith, HMS III Gillian Lieberman, MD Perforation: Overview • Incidence – Approx. 1.3% of cases • Clinical Manifestations – Abdominal pain – Elevated serum amylase • Risk Factors – – – – – – – – Sphincterotomy Sphincter of Oddi dysfunction Dilated CBD Long procedure Biliary stricture dilatation Duodenal diverticula Aberrant biliary anatomy Post-surgical anatomy (Roux-en-Y gastric bypass) 21 Grant Smith, HMS III Gillian Lieberman, MD Perforation: Radiologic Findings • Menu of Radiologic Tests – Plain Abdominal Film • Free air seen as “Rigler’s Sign” (bowel wall outlined by air) or the “Football Sign” (central lucency with visualization of falciform and medial umbilical ligaments). – Free air is best seen on upright films or left lateral decubitus (if unable to stand) or cross-table lateral view. – Computed Tomography • Ability to see tiny foci of free air not seen on plain films. • Recommended if patient has increase WBC count or pain and fever. • Bile infection and bile leakage through a perforation seen on CT correlates with increased mortality. 22 Grant Smith, HMS III Gillian Lieberman, MD Perforation: Companion Patient • 49 year old female • ERCP performed for evaluation of RUQ found to have acute cholecystitis • The patient had pain immediately after the procedure and a significant amount of free air. • Subcutaneous free air • Pneumoperitoneum • Pneumoretroperitoneum • Pneumomediastinum Pannu HK, Fishman EK. Complications of endoscopic retrograde cholangiopancreatography: spectrum of abnormalities demonstrated with CT. Radiographics 2001;21(6):1441-53. Abdominal CT without contrast, axial, abdominal windows 23 Grant Smith, HMS III Gillian Lieberman, MD Pancreatitis: Overview • Incidence – Approx. 5% of diagnostic cases and 10% of therapeutic cases • Clinical Manifestations – Abdominal pain for >24hrs s/p ERCP • Often epigastric or back pain with nausea – Elevated serum amylase and lipase (3x normal) • Risk Factors – Operator-Related: inadequate training, lack of experience, low case volume – Patient-Related: younger age, females, recurrent pancreatitis, history of post-ERCP pancreatitis, Sphincter of Oddi dysfunction – Procedure-Related factors: difficulty with cannulation, pancreatic duct infection, precut/pancreatic/minor papilla sphincterotomy, or biliary balloon sphincteroplasty. 24 Grant Smith, HMS III Gillian Lieberman, MD Pancreatitis: Radiologic Findings • Menu of Radiologic Tests – Computed Tomography • Heterogeneous enhancement and gland enlargement. • Peripancreatic fat has increased attenuation due to extravasation of pancreatic secretions. • Glandular necrosis appears as hypoattenuation. • Infected necrosis appears as bubbles of gas in devitalized parenchyma. 25 Grant Smith, HMS III Gillian Lieberman, MD Pancreatitis: Companion Patient • 50-year-old man s/p ERCP for a mass in the pancreatic tail • The patient was readmitted 3 days after ERCP with abdominal pain and low-grade fever. • Heterogeneous attenuation of the pancreas. • Low-attenuation areas (*) suggest necrosis. • Thickening of the wall of the antrum of the stomach (arrow) secondary to local inflammation. • Stranding of the peripancreatic fat. Pannu HK, Fishman EK. Complications of endoscopic retrograde cholangiopancreatography: spectrum of abnormalities demonstrated with CT. Radiographics 2001;21(6):1441-53. Abdominal CT with contrast, axial, abdominal windows 26 Grant Smith, HMS III Gillian Lieberman, MD Pancreatitis: Companion Patient – Fat Stranding Fat stranding around the pancreas Pannu HK, Fishman EK. Complications of endoscopic retrograde cholangiopancreatography: spectrum of abnormalities demonstrated with CT. Radiographics 2001;21(6):1441-53 Abdominal CT with contrast, axial, abdominal windows 27 Grant Smith, HMS III Gillian Lieberman, MD Pancreatitis: Index Patient Infected pancreatic necrosis with gas BIDMC, PACS Abdominal CT with contrast, axial, abdominal windows 28 Grant Smith, HMS III Gillian Lieberman, MD Hemorrhage: Overview • Incidence – Approx. 1.3% (with about 29% of bleeds requiring >5 units of transfusions or intervention) • Clinical Manifestations – Drop in hemoglobin/hematocrit – Melena or hematemesis • Risk Factors – – – – – – Sphincterotomy Evidence of bleeding at time of sphincterotomy Prior sphincterotomy Prolonged PTT (at least 2x above normal) Periampullary diverticulum Cholangitis 29 Grant Smith, HMS III Gillian Lieberman, MD Hemorrhage: Radiologic Findings • Menu of Radiologic Tests and Findings – Computed Tomography (CT) • Typically not performed to diagnose hemorrhage; but bleeding may be detected if CT is performed. • Acute hemorrhage is hyperattenuating on noncontrast CT, which can become iso/hypoattenuating in later stages. • Non-contrast CT is used to assess for hematoma, while contrast-enhanced CT angiography is used to assess for site of active extravasation. 30 Grant Smith, HMS III Gillian Lieberman, MD Hemorrhage: Companion Patient #1 • 67-year-old woman s/p ERCP with unsuccessful cannulation of the common bile duct • The patient experienced pain after the procedure. • High attenuation area between the duodenum and pancreas (arrow) representing bleeding Pannu HK, Fishman EK. Complications of endoscopic retrograde cholangiopancreatography: spectrum of abnormalities demonstrated with CT. Radiographics 2001;21(6):1441-53 Abdominal CT with contrast, axial, abdominal windows 31 Grant Smith, HMS III Gillian Lieberman, MD Hemorrhage: Companion Patient #2 • High-attenuation mass (arrow) that appears to be abutting the lumen of the duodenum, a finding compatible with intramural bleeding. Pannu HK, Fishman EK. Complications of endoscopic retrograde cholangiopancreatography: spectrum of abnormalities demonstrated with CT. Radiographics 2001;21(6):1441-53 Abdominal CT with contrast, axial, abdominal windows 32 Grant Smith, HMS III Gillian Lieberman, MD Infection/Cholangitis: Overview • Infection can include many complications • Ascending cholangitis is the most frequent infectious complication of ERCP • Incidence – Approx 1.4% (with range of 0.4-10% depending on the study) • Clinical Manifestations – – – – – – Typically occur 24-72 hours after ERCP Fever Jaundice Charcot’s Triad Abdominal pain (RUQ) May develop confusion and hypotension Elevated WBC count Reynold’s Pentad • Risk Factors – Biliary stents – Combined percutaneous and endoscopic procedures – Unsuccessful drainage of the biliary system (retained stones) 33 Grant Smith, HMS III Gillian Lieberman, MD Infection/Cholangitis: Radiologic Findings • Menu of Radiologic Tests – Computed Tomography (CT) • Bile ducts may appear dilated and bile itself may appear hyperattenuated due to increased debris. • Thickening of wall of ducts and pneumobilia. • Peri-biliary hyperattenuation. • Abscesses may also appear with enhancing capsules. 34 Grant Smith, HMS III Gillian Lieberman, MD Infection/Cholangitis: Companion Patient • 67 year old man with common bile duct stones • In this case, has not undergone ERCP but demonstrates findings of biliary obstruction • Diffuse, mottled enhancement of the liver parenchyma • Dilatation of the intrahepatic bile ducts (arrows) Kim SW, Shin HC, Kim HC, Hong MJ, Kim IY. Diagnostic performance of multidetector CT for acute cholangitis: evaluation of a CT scoring method. The British journal of radiology. Abdominal CT with contrast, axial, abdominal windows 35 Grant Smith, HMS III Gillian Lieberman, MD Summary • ERCP is an endoscopic procedure primary used for therapeutic intervention. • ERCP is appropriately used to remove stones from the CBD, assist in diagnosis of pancreatic/ampullary masses, and stent placement for biliary obstruction. • The main complications of ERCP include perforation, pancreatitis, hemorrhage, and infection. • Computed tomography is a good first choice for investigating for complications of ERCP when patients become acutely ill within 24-48 hours after ERCP. 36 Grant Smith, HMS III Gillian Lieberman, MD 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. References Cohen S, Bacon BR, Berlin JA, et al. National Institutes of Health State-of-the-Science Conference Statement: ERCP for diagnosis and therapy, January 14-16, 2002. Gastrointestinal endoscopy 2002;56(6):803-9. Adler DG, Baron TH, Davila RE, et al. ASGE guideline: the role of ERCP in diseases of the biliary tract and the pancreas. Gastrointestinal endoscopy 2005;62(1):1-8. Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointestinal endoscopy 1991;37(3):383-93. Andriulli A, Loperfido S, Napolitano G, et al. Incidence rates of post-ERCP complications: a systematic survey of prospective studies. The American journal of gastroenterology 2007;102(8):1781-8. Williams EJ, Taylor S, Fairclough P, et al. Risk factors for complication following ERCP; results of a large-scale, prospective multicenter study. Endoscopy 2007;39(9):793-801. Wang P, Li ZS, Liu F, et al. Risk factors for ERCP-related complications: a prospective multicenter study. The American journal of gastroenterology 2009;104(1):31-40. Zissin R, Shapiro-Feinberg M, Oscadchy A, Pomeranz I, Leichtmann G, Novis B. Retroperitoneal perforation during endoscopic sphincterotomy: imaging findings. Abdominal imaging 2000;25(3):279-82. Cohen SA, Siegel JH, Kasmin FE. Complications of diagnostic and therapeutic ERCP. Abdominal imaging 1996;21(5):38594. Scarlett PY, Falk GL. The management of perforation of the duodenum following endoscopic sphincterotomy: a proposal for selective therapy. The Australian and New Zealand journal of surgery 1994;64(12):843-6. Pannu HK, Fishman EK. Complications of endoscopic retrograde cholangiopancreatography: spectrum of abnormalities demonstrated with CT. Radiographics 2001;21(6):1441-53 Balthazar EJ. CT diagnosis and staging of acute pancreatitis. Radiologic clinics of North America 1989;27(1):19-37. Balthazar EJ, Freeny PC, vanSonnenberg E. Imaging and intervention in acute pancreatitis. Radiology 1994;193(2):297306. Testoni PA, Mariani A, Giussani A, et al. Risk factors for post-ERCP pancreatitis in high- and low-volume centers and among expert and non-expert operators: a prospective multicenter study. The American journal of gastroenterology;105(8):1753-61 Kim SW, Shin HC, Kim HC, Hong MJ, Kim IY. Diagnostic performance of multidetector CT for acute cholangitis: evaluation of a CT scoring method. The British journal of radiology. Carr-Locke DL. Therapeutic role of ERCP in the management of suspected common bile duct stones. Gastrointestinal endoscopy 2002;56(6 Suppl):S170-4. Ho ML, Gutierrez FR. Chest radiography in thoracic polytrauma. Ajr 2009;192(3):599-612. 37 Special Thanks To: • Dr. Gillian Lieberman • Dr. Mai-Lan Ho • Dr. Mark Ashkan 38