Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Polysubstance dependence wikipedia , lookup
Prescription costs wikipedia , lookup
Drug discovery wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Clinical trial wikipedia , lookup
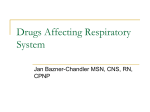
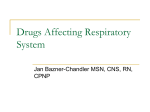
CLINICAL RESEARCH STUDY Long-acting Beta-Agonists with and without Inhaled Corticosteroids and Catastrophic Asthma Events Shelley R. Salpeter, MD, FACP,a,b Andrew J. Wall, MD,a,b Nicholas S. Buckleyc a Stanford University School of Medicine, Stanford, Calif; bSanta Clara Valley Medical Center, San Jose, Calif; cCalifornia Institute for Technology, Pasadena. ABSTRACT BACKGROUND: It is unclear whether long-acting -agonists with concomitant inhaled corticosteroids increase asthma-related intubations and deaths. We pooled data on long-acting -agonists with variable and concomitant inhaled corticosteroids to evaluate the risk for catastrophic asthma events. METHODS: We conducted searches of electronic databases, the US Food and Drug Administration website, clinical-trials registries, and selected references through December 2008. We analyzed randomized controlled trials in patients with asthma, which lasted at least 3 months, evaluated long-acting -agonists compared with placebo or long-acting -agonists with inhaled corticosteroids compared with corticosteroids alone, and included at least 1 catastrophic event, defined as asthma-related intubation or death. RESULTS: In pooled trial data that included 36,588 participants, long-acting -agonists increased catastrophic events 2-fold (Peto odds ratio [OR] 2.10; 95% confidence interval [CI], 1.37-3.22). Statistically significant increases were seen for long-acting -agonists with variable corticosteroids compared with placebo (OR 1.83; 95% CI, 1.14-2.95) and for concomitant treatment with corticosteroids compared with corticosteroids alone (OR 3.65; 95% CI, 1.39-9.55). Similar increases in risk were seen for variable and concomitant corticosteroid use, salmeterol and formoterol, and children and adults. When the analysis was restricted to trials with controlled corticosteroid use, given as part of the study intervention, concomitant treatment still increased catastrophic events compared with corticosteroids alone (OR 8.19; 95% CI, 1.10-61.18). CONCLUSION: Long-acting -agonists increase the risk for asthma-related intubations and deaths, even when used in a controlled fashion with concomitant inhaled corticosteroids. © 2010 Elsevier Inc. All rights reserved. • The American Journal of Medicine (2010) 123, 322-328 KEYWORDS: Asthma; Inhaled corticosteroids; Intubation; Long-acting beta-agonists; Meta-analysis; Mortality There has been growing concern about asthma-related morbidity and mortality associated with the long-acting -agonists salmeterol and formoterol, given with or without concomitant inhaled corticosteroids.1-3 Pooled trial data have consistently shown that long-acting -agonists, when given Funding: Santa Clara Valley Medical Center, San Jose, Calif. Conflict of Interest: None of the authors have any conflicts of interest associated with the work presented in this manuscript. None of the authors have had any relationships with a pharmaceutical company that manufactures a -agonist or other respiratory medications. Dr Salpeter has provided expert testimony on a litigation case involving a long-acting -agonist and was paid on an hourly basis. Authorship: All authors had access to the data and played a role in writing this manuscript. Reprint requests should be addressed to Shelley Salpeter, MD, 751 S. Bascom Ave, San Jose, CA 95128. E-mail address: [email protected] 0002-9343/$ -see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.amjmed.2009.07.035 with variable inhaled corticosteroid use, increase the risk for asthma-related hospitalizations, intubations, and deaths.4-8 In July 2005 an advisory committee to the US Food and Drug Administration (FDA) concluded that Boxed Warnings of an increased risk for asthma-related mortality should be placed on all products containing long-acting -agonists, with recommendations for treatment only after other asthma drugs have failed.1 The FDA subsequently requested data from sponsors of long-acting -agonists (GlaxoSmithKline, Brentford, London, England; AstraZeneca, Wilmington, Del; and Novartis, Basel, Switzerland) on asthma-related intubations and deaths that occurred during published and unpublished randomized trials, as of January 2008.9-11 Several meta-analyses have been performed, most with the cooperation or sponsorship of the pharmaceutical industry, which evalu- Salpeter et al Safety of Long-acting -Agonists 323 ated long-acting -agonists with concomitant inhaled corOutcome Measures ticosteroids.7-15 These analyses consistently reported more Two reviewers independently extracted data from the seasthma intubations and deaths for combined treatment comlected articles, reconciling differences by consensus. Outpared with inhaled corticosteroids alone, but none reached comes assessed were catastrophic asthma events, defined as statistical significance. However, each of these studies reasthma-related intubations or deaths that were reported by stricted their analyses to a subset the investigator or the industry of the total available data, for exsponsor. Attempts were made to ample, including only trials with contact investigators of previous CLINICAL SIGNIFICANCE salmeterol,9,14 formoterol,7,11,13 meta-analyses and the industry adults, 12 asthma deaths, 7 pubsponsors to obtain additional in● There is a 3-fold increase in asthmalished reports of events,15 single formation concerning trials and related intubations and deaths in those drug sponsors,7,9-11,14 or FDA-apevents.  -agonists with contaking long-acting proved dosages8,14,15 of long-actcomitant corticosteroids compared with ing -agonists. Statistical Analysis corticosteroids alone. In December 2008 a follow-up The proportions of patients with a FDA advisory committee meeting ● Similar increases in risk are seen for catastrophic event to those withconcluded that the risks of salmevariable and concomitant corticosteroid out events from each trial were terol (Serevent, GlaxoSmithKline) use, salmeterol and formoterol, children pooled using the fixed-effects and formoterol (Foradil, Novartis) and adults, and fatal and nonfatal method expressed as a Peto odds outweighed the benefits and ratio (OR) with corresponding events. should be banned for use in 95% confidence intervals.17 This ● This information can help assess the asthma for all ages.16 The commethod was chosen because we risks and benefits of the addition of mittee separately evaluated longnoted low event rates and minimal acting -agonists combined with a long-acting -agonists to inhaled corinterstudy heterogeneity in the corticosteroid in a single inhaler, ticosteroids in the treatment of asthma. analysis.17 The results were then such as salmeterol with fluticacompared with those found with sone (Advair, GlaxoSmithKline) the random-effects method.18 Evand formoterol with budesonide idence of interstudy heterogeneity (Symbicort; AstraZeneca), and concluded that further safety was evaluated, with statistical significance set at alstudies were needed to assess risk.1,16 pha ⫽ 0.1. The analysis was performed using Cochrane ReThe objective of this meta-analysis is to pool all the view Manager 4.2 (Cochrane Library Software, Oxford, available data on long-acting -agonists with variable and UK). concomitant inhaled corticosteroids, evaluating the risk for Only trials that reported at least 1 event could be used in asthma-related intubations or deaths. Subgroup analyses the estimation of odds ratios. A subsequent analysis inwill compare results between variable and concomitant corcluded all trials, published and unpublished, with and withticosteroids, salmeterol and formoterol, adults and children, out reported events, to estimate an absolute increase in risk; and fatal and nonfatal events. these results are reported in the “Discussion” section. Subgroup analyses, chosen a priori, were performed to MATERIALS AND METHODS evaluate the difference in results between trials with variable corticosteroids (use in ⬍ 100% of participants) versus Trial Inclusion concomitant corticosteroids (use in 100% of participants), We performed a search of the MEDLINE, EMBASE, and salmeterol versus formoterol, children (aged ⬍ 12 years) Cochrane databases; the US FDA website; clinical-trials versus adults, and fatal versus nonfatal events. Further subregistries of drug manufacturers; and previous meta-analygroup analysis compared results between trials with no ses to identify trials on long-acting -agonist use in patients corticosteroid use at all and trials with the controlled use of with asthma published through December 2008. Studies corticosteroid as a study drug in combination with a longwere included if they were randomized controlled trials of acting -agonist (either in a single inhaler or separate inlong-acting -agonists compared with placebo or long-acthalers). The results of the subgroups were compared with ing -agonists with inhaled corticosteroids compared with each other using the test of interaction.19 an equal or higher dose of inhaled corticosteroids alone of at A sensitivity analysis was performed to evaluate the effect of least 3 months duration that reported at least 1 asthmaexcluding pooled trial data from GlaxoSmithKline, because indirelated intubation or death. We included reports of events vidual trial-level information was not available for these events. that were provided by the investigator in the published trial or by the drug manufacturer in a subsequent account. In Role of the Funding Source addition, we included pooled trial data from GlaxoSmithKline, The funding for this analysis came from salary support from because we were unable to obtain individual trial-level inSanta Clara Valley Medical Center for Drs Salpeter and formation for those events. 324 The American Journal of Medicine, Vol 123, No 4, April 2010 Wall. The institution had no role in the design, conduct, or reporting of the study. The investigators all had complete access to the data, and no sponsorship from the institution or the pharmaceutical industry was provided to conduct this analysis. RESULTS Search Results Figure 1 shows the results of the search for articles. The search identified approximately 6500 articles, of which 211 were potentially relevant trials. Of these, 10 individual trials met the inclusion criteria.20-29 GlaxoSmithKline provided additional pooled trial data for long-acting -agonists with and without concomitant inhaled corticosteroids.9 For the meta-analysis, these data were considered to be 2 pooled trials of long-acting -agonists, one without any concomitant corticosteroid use and one with background corticosteroid use in all patients. Trials were excluded for the following reasons: Two trials were not randomized, 2 trials were of asthma and chronic obstructive pulmonary disease, 19 trials did not have the appropriate comparator groups, 70 trials were of less than 3 months duration, 23 trials provided duplicate data on participants from other trials, and 83 trials did not report adverse events. Figure 1 Trial Characteristics The meta-analysis included a total of 36,588 participants followed for 21,343 patient-years (Table 1, online). The mean trial duration was 7.0 months (range, 3-12 months), with a mean study size of 3183 participants (248-26,353). The mean (standard deviation) age of participants at baseline was 38.3 (1.7) years (45.3% were men) in the -agonist group and 38.7 (1.1) years (44.8% were men) in the control group. The dropout rate was 19.2% in the -agonist group and 21.4% in the control group. All trials were randomized, double-blind trials that performed analysis according to intention-to-treat. Five trials evaluated -agonists with variable inhaled corticosteroid use, with a total of 29,335 participants followed for 14,932 patient-years. Inhaled corticosteroids were used by 47.9% of the participants. Seven trials evaluated -agonists with concomitant inhaled corticosteroids, with a total of 7253 participants followed for 6044 patient-years. All participants received inhaled corticosteroids, either as uncontrolled background use or controlled as part of the study intervention. The combination of -agonist and corticosteroid was compared with an equal dose of corticosteroid in 4 trials, an equal or higher dose of corticosteroid in 1 trial, and a higher dose of corticosteroid in 2 trials (Table 1, online). Flow chart of trials search. Salpeter et al Safety of Long-acting -Agonists 325 Figure 2 Effect of long-acting -agonists on asthma intubations and deaths. 1. Long-acting -agonists with variable inhaled corticosteroids compared with placebo. 2. Long-acting -agonists with concomitant inhaled corticosteroids compared with inhaled corticosteroids alone. n ⫽ number of participants with at least 1 asthma intubation or death; N ⫽ number of participants; SMART ⫽ Salmeterol Multi-center Asthma Research Trial; GSK ⫽ GlaxoSmithKline; OR ⫽ odds ratio; CI ⫽ confidence interval. Asthma-related Intubations and Deaths For all trials combined, there were 59 catastrophic events in the -agonist group and 26 events in the control group (Table 1, online), with a Peto odds ratio of 2.10 (95% confidence interval [CI], 1.37-3.22; Figure 2). For trials with variable corticosteroid use, the odds ratio for catastrophic events for long-acting -agonists was 1.83 (95% CI, 1.14-2.95) compared with placebo. For trials with concomitant corticosteroids, the odds ratio for catastrophic events for long-acting -agonists plus inhaled corticosteroids, compared with inhaled corticosteroids alone, was 3.65 (95% CI, 1.39-9.55). Table 2 Minimal interstudy heterogeneity was noted in the analyses (P ⬎.8). Similar results were seen when the analysis was performed using the random effects method, with significant increases in catastrophic events seen for variable corticosteroid use (OR 1.76; 95% CI, 1.08-2.89) and concomitant corticosteroid use (OR 2.7; 95% CI, 1.06-6.88). In subgroup analysis, there was no statistically significant difference in results between concomitant and variable corticosteroids, with a P value for interaction of 0.24 (Table 2). Similar results were seen for trials with controlled corticosteroid use as part of the study intervention (OR 8.19; 95% CI, 1.1-61.18) and trials that used no corticosteroids at Subgroup Analysis Analysis Subgroup Odds Ratio (95% CI) P Value for Interaction ICS use: variable compared with concomitant use Variable ICS Concomitant ICS No ICS Controlled ICS Salmeterol Formoterol Adults Children Intubations Deaths 1.83 3.65 2.2 8.19 1.94 4.81 2.08 2.58 1.76 4.03 .24 ICS use: no use compared with controlled study drug -agonist used Age of participants Asthma event ICS ⫽ inhaled corticosteroid; CI ⫽ confidence interval. (1.14-2.95) (1.39-9.55) (1.1-4.36) (1.1-61.18) (1.24-3.04) (1.12-20.68) (1.35-3.20) (0.96-6.94) (1.08-9.55) (1.7-9.55) .23 .28 .69 .42 326 all (OR 2.2; 95% CI, 1.1-4.36, P for interaction ⫽ .23). In further subgroup analysis, there was no significant difference in results for formoterol compared with salmeterol, children compared with adults, and asthma deaths compared with intubations (Table 2). In sensitivity analysis, when the pooled data from GlaxoSmithKline were excluded, significant increases in catastrophic events were seen for variable corticosteroid use (OR 1.79; 95% CI, 1.09-2.92) and concomitant corticosteroid use (OR 7.34; 95% CI, 1.42-37.97). DISCUSSION Our pooled data show that the use of long-acting -agonists, with and without concomitant inhaled corticosteroids, was associated with a significant increase in risk for asthmarelated intubations and deaths. The magnitude of risk was, in fact, higher for trials with controlled concomitant corticosteroid use (OR 8.2) than for trials with no corticosteroid use at all (OR 2.2), although the difference between the 2 subgroups was not statistically significant. The results of this meta-analysis are based on a relatively small number of events, so they should be interpreted with caution. However, these findings provide evidence that long-acting -agonists are associated with significant risk, even when used with concomitant inhaled corticosteroids. This is the first meta-analysis to show that concomitant treatment with long-acting -agonists and inhaled corticosteroids increased catastrophic asthma events. This is because our analysis was based almost entirely on reports of events provided by the drug manufacturers to the FDA, which were not released until December 2008.9-11 Of note, only 2 trials reported asthma-related intubations or death in their published article.22,25 We chose to use the composite outcome of asthma-related intubation or death because both of these catastrophic events are increased with long-acting -agonist use.4-8 Similar increases in risk were seen for fatal and nonfatal events. We also chose to pool the data on salmeterol and formoterol, and on adults and children. We thought this was reasonable because little heterogeneity was seen in results between these subgroups. A consistent finding was a greater number of catastrophic events in the -agonist group, compared with the control group, in each of the trials included in the analysis. This meta-analysis was not designed to assess the absolute increase in catastrophic events associated with the addition of long-acting -agonists to inhaled corticosteroids, because only those trials with at least 1 event are included in the calculation of odds ratios. To estimate the total number of patients at risk, we can use the cumulative trial data provided in the briefing material from the drug manufacturers, which includes published and unpublished trials with and without reported events.9,11 If all trials with and without events are included in the analysis, there were 14 events in 35,000 patients treated with combined therapy (0.04%) and 3 events in 29,000 patients treated with corticosteroids alone (0.01%) over an average trial duration of 5 months. The American Journal of Medicine, Vol 123, No 4, April 2010 This would indicate an absolute increase in risk of 3 catastrophic asthma events per 10,000 patients treated over a 5-month period. The magnitude of the potential problem is highlighted by the fact that several million patients are treated with long-acting -agonists in the United States each year, the majority of whom also are receiving inhaled corticosteroids.9,30 One proposed mechanism for the increase in catastrophic asthma events associated with long-acting -agonists is the development of tolerance to their bronchoprotective effects over time.31,32 Regular use of short- and long-acting -agonists is associated with down-regulation and desensitization of -receptors, an increase in airway hyperreactivity, and an increase in asthma deaths and near-deaths.31,33-35 The use of inhaled corticosteroids, on the other hand, is associated with reduced airway reactivity and a reduction in life-threatening and fatal events.26,36,37 Although there is some evidence that corticosteroids might partially protect against the adverse effects of -agonists, regular -agonist use still results in substantial tolerance to its effects over time, despite concomitant treatment with corticosteroids.31,34 The sole purpose of this meta-analysis was to evaluate the risk for catastrophic events associated with long-acting -agonists. The study did not evaluate the benefits of longacting -agonists and therefore could not assess the risk-tobenefit ratio of these agents. A recent advisory committee to the FDA reviewed the available evidence and concluded that the risks of salmeterol (Serevent) and formoterol (Foradil) for asthma outweighed the benefits and should be banned for use in asthma for all ages.16 The committee agreed that further safety studies were still needed to clarify the risk of combination products, such as salmeterol with fluticasone (Advair) and formoterol with budesonide (Symbicort).16 If long-acting -agonists were not used in the treatment of asthma, other treatment options include inhaled and oral corticosteroids, leukotriene inhibitors, shortacting anticholinergic agents, and as-needed short-acting -agonists.38-41 In the United States, the asthma mortality rate peaked in the 1990s and has now been steadily declining over the past several years.42 This reduction in mortality, despite the continued use of long-acting -agonists, has been used as evidence against an adverse mortality effect of these drugs.9,14 However, one possible explanation for this trend could be that the asthma mortality rates are related to the ratio of -agonist use to inhaled corticosteroid use over time.42 The sales of long-acting -agonists were increasing over the past several years, but the sales of inhaled corticosteroids increased even faster during this time period, so that the ratio of -agonist to inhaled corticosteroid use has gradually decreased at a rate that is proportional to the decreasing trend in asthma mortality rates.9,42,43 If there were, in fact, a causal relationship between the ratio of -agonist to corticosteroid use and asthma mortality in the United States, then we would expect a further decrease in asthma deaths if the sales of long-acting -agonists were curtailed. Salpeter et al Safety of Long-acting -Agonists 327 STUDY LIMITATIONS Our analysis has several limitations. Standard meta-analytic results can be uncertain when the numbers of events per study are small, as is the case with catastrophic asthma events. The assessment of intubations and deaths was further hindered by the fact that many trials did not report the events even when they occurred and by the difficulty in ascertaining the true cause of respiratory failure or death. We chose to include only those events reported by the investigator or drug manufacturer to be asthma-related intubations or deaths. If we had chosen to include other life-threatening events thought to be due to “status asthmaticus” or “severe acute asthma” without documentation of intubation, or to include respiratory arrests and sudden deaths of unclear cause, there would be 12 more events, with 9 occurring in the long-acting -agonist group and 3 occurring in the control group. We chose to compare the combination of -agonist and corticosteroid with an equal or higher dose of corticosteroid to assess whether the addition of long-acting -agonists to inhaled corticosteroids carried a greater risk than the use of corticosteroids alone. We also chose to exclude from the analysis trials that used an active-comparator drug, such as a short-acting -agonist, in the control group. However, our analysis of the pooled data provided by GlaxoSmithKline indicates that the long-acting -agonist salmeterol increases the risk for asthma intubation or death by 2-fold compared with active-comparator controls (OR 2.09; 95% CI, 1.04-4.21]).9 CONCLUSIONS Despite these limitations, our pooled data suggest that longacting -agonists increase the risk for asthma-related intubations and deaths, even when used in a controlled fashion with concomitant inhaled corticosteroids. At present, guidelines suggest that long-acting -agonists be added to inhaled corticosteroids in patients with moderate or severe asthma that is not well controlled with inhaled corticosteroids alone,38 but this approach might not in fact confer a meaningful health benefit compared with the use of other standard therapies.1 The results of this meta-analysis suggest that long-acting -agonists carry significant risk for catastrophic asthma events, even when used concomitantly with inhaled corticosteroids. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. ACKNOWLEDGMENT The authors thank Hau Liu, MD, for assistance during the preparation of this manuscript. Dr Liu received no compensation for this contribution. References 1. US Food and Drug Administration Office of Surveillance and Epidemiology. Risks and benefits of long-acting beta adrenergic agonists in the treatment of asthma. Available at: http://www.fda.gov/ohrms/ 17. 18. 19. dockets/ac/08/briefing/2008-4398b1-01-FDA.pdf. Accessed December 6, 2008. Kramer JM. Balancing the benefits and risks of inhaled long-acting beta-agonists–the influence of values. N Engl J Med. 2009;360:15921595. Drazen JM, O’Byrne PM. Risks of long-acting beta-agonists in achieving asthma control. N Engl J Med. 2009;360:1671-1672. Salpeter SR, Buckley NS, Ormiston TM, Salpeter EE. Long-acting beta-agonists increase severe asthma exacerbations and asthma-related deaths: meta-analysis of randomized controlled trials. Ann Intern Med. 2006;144:904-912. Cates CJ, Cates MJ. Regular treatment with salmeterol for chronic asthma: serious adverse events. Cochrane Database Syst Rev. 2008: CD006363. Cates CJ, Cates MJ, Lasserson TJ. Regular treatment with formoterol for chronic asthma: serious adverse events. Cochrane Database Syst Rev. 2008(4):CD006923. Sears MR, Ottosson A, Radner F, Suissa S. Long-acting beta-agonists: a review of formoterol safety data from asthma clinical trials. Eur Respir J. 2009;33:21-32. Levenson M. Long-acting beta-agonists and adverse asthma events meta-analysis. Statistical briefing package for Joint Meeting of the Pulmonary-Allergy Drugs Advisory Committee, Drug Safety and Risk Management Advisory Committee and Pediatric Advisory Committee on December 10-11, 2008. Available at: http://www.fda.gov/ohrms/ dockets/ac/08/briefing/2008-4398b-01-FDA.pdf. Accessed December 6, 2008. GlaxoSmithKline. Sponsor briefing information. Benefit risk assessment of salmeterol for the treatment of asthma in adults and children. Available at: http://www.fda.gov/ohrms/dockets/ac/08/briefing/20084398b1-04-GSK.pdf. Accessed December 6, 2008. Novartis. Foradil. FDA Advisory Committee meeting on the safety of long-acting beta2-agonists for the treatment of asthma in adults and children (December 10-11, 2008). Briefing document. Available at: http://www.fda.gov/ohrms/dockets/ac/08/briefing/2008-4398b1-02Novartis.pdf. Accessed December 6, 2008. AstraZeneca. AstraZeneca briefing materials: Review of the benefits and risks of formoterol-containing products. Available at: http://www/ fda.gov/ohrms/dockets/ac/08/briefing/2008-4398b1-03-AstraZeneca. pdf. Accessed December 6, 2008. Jaeschke R, O’Byrne PM, Mejza F, et al. The safety of long-acting beta-agonists among patients with asthma using inhaled corticosteroids: systematic review and metaanalysis. Am J Respir Crit Care Med. 2008;178:1009-1016. Jaeschke R, O’Byrne PM, Nair P, et al. The safety of formoterol among patients with asthma using inhaled corticosteroids. Systematic review and meta-analysis. Pol Arch Med Wewn. 2008;118:627-635. Bateman E, Nelson H, Bousquet J, et al. Meta-analysis: effects of adding salmeterol to inhaled corticosteroids on serious asthma-related events. Ann Intern Med. 2008;149:33-42. Rodrigo GJ, Moral VP, Marcos LG, Castro-Rodriguez JA. Safety of regular use of long-acting beta agonists as monotherapy or added to inhaled corticosteroids in asthma. A systematic review. Pulm Pharmacol Ther. 2009;22:9-19. US Food and Drug Administration. Summary minutes of the joint Pulmonary-Allergy Drugs Advisory Committee, Drug Safety and Risk Management Advisory Committee, and Pediatric Advisory Committee, December 10-11, 2008. Available at: http://www.fda.gov/ohrms/ dockets/AC/08/minutes/2008-4398m1-final.pdf. Accessed February 6, 2009. Bradburn MJ, Deeks JJ, Berlin JA, Russell Localio A. Much ado about nothing: a comparison of the performance of meta-analytical methods with rare events. Stat Med. 2007;26:53-77. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177-188. Altman DG, Bland JM. Interaction revisited: the difference between two estimates. BMJ. 2003;326:219. 328 20. U.S Food and Drug Association. Center for Drug Evaluation and Review. Foradil (Formoterol Fumarate inhalation) aerolizer. Part 4. Available at: http://www.fda.gov/cder/foi/nda/2001/20831_ Foradil_medr_P4.pdf. Accessed September 3, 2005. 21. U.S Food and Drug Association. Center for Drug Evaluation and Review. Foradil (Formoterol Fumarate inhalation) aerolizer. Part 5. Available at: http://www.fda.gov/cder/foi/nda/2001/20831_ Foradil_medr_P5.pdf. Accessed September 3, 2005. 22. Nelson HS, Weiss ST, Bleecker ER, et al. The Salmeterol Multicenter Asthma Research Trial: a comparison of usual pharmacotherapy for asthma or usual pharmacotherapy plus salmeterol. Chest. 2006;129: 15-26. 23. Ind PW, Dal Negro R, Colman NC, et al. Addition of salmeterol to fluticasone propionate treatment in moderate-to-severe asthma. Respir Med. 2003;97:555-562. 24. Kelsen SG, Church NL, Gillman SA, et al. Salmeterol added to inhaled corticosteroid therapy is superior to doubling the dose of inhaled corticosteroids: a randomized clinical trial. J Asthma. 1999;36:703715. 25. Kemp JP, Cook DA, Incaudo GA, et al. Salmeterol improves quality of life in patients with asthma requiring inhaled corticosteroids. Salmeterol Quality of Life Study Group. J Allergy Clin Immunol. 1998; 101(2 Pt 1):188-195. 26. O’Byrne PM, Barnes PJ, Rodriguez-Roisin R, et al. Low dose inhaled budesonide and formoterol in mild persistent asthma: the OPTIMA randomized trial. Am J Respir Crit Care Med. 2001;164(8 Pt 1):13921397. 27. O’Byrne PM, Bisgaard H, Godard PP, et al. Budesonide/formoterol combination therapy as both maintenance and reliever medication in asthma. Am J Respir Crit Care Med. 2005;171:129-136. 28. Von Berg A, Papageorgiou Saxoni F, Wille S, et al. Efficacy and tolerability of formoterol Turbuhaler in children. Int J Clin Pract. 2003;57:852-856. 29. U.S Food and Drug Administration. NDA 020831 Formoterol fumarate clinical review. Available at: http://www.fda.gov/ohrms/dockets/ ac/05/briefing/2005-4148B1_03_03-FDA-Clinical-Review.pdf. Accessed September 3, 2005. 30. Patterns of medication use in the United States, 2006. A Report from the Slone Survey. Available at: http://www.bu.edu/slone/SloneSurvey/ The American Journal of Medicine, Vol 123, No 4, April 2010 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. AnnualRpt/SloneSurveyWebReport2006.pdf. Accessed February 21, 2009. Salpeter SR, Ormiston TM, Salpeter EE. Meta-analysis: respiratory tolerance to regular beta2-agonist use in patients with asthma. Ann Intern Med. 2004;140:802-813. Lipworth BJ. Long-acting beta(2)-adrenoceptor agonists: a smart choice for asthma? Trends Pharmacol Sci. 2007;28:257-262. Epub 2007 Apr 26. Sears MR, Taylor DR, Print CG, et al. Regular inhaled beta-agonist treatment in bronchial asthma. Lancet. 1990;336:1391-1396. Kalra S, Swystun VA, Bhagat R, Cockcroft DW. Inhaled corticosteroids do not prevent the development of tolerance to the bronchoprotective effect of salmeterol. Chest. 1996;109:953-956. Spitzer WO, Suissa S, Ernst P, et al. The use of beta-agonists and the risk of death and near death from asthma. N Engl J Med. 1992;326: 501-506. Kerrebijn KF, van Essen-Zandviet EEM, Neijens JJ. Effects of longterm treatment with inhaled corticosteroids and beta-agonists on the bronchial responsiveness in children with asthma. J Allergy Clin Immunol. 1987;79:653-659. Suissa S, Ernst P. Inhaled corticosteroids: impact on asthma morbidity and mortality. J Allergy Clin Immunol. 2001;107:937-944. Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007. J Allergy Clin Immunol. 2007;120(5 Suppl):S94-S138. Gross NJ. Anticholinergic agents in asthma and COPD. Eur J Pharmacol. 2006;533:36-39. Currie GP, Lee DK, Srivastava P. Long-acting bronchodilator or leukotriene modifier as add-on therapy to inhaled corticosteroids in persistent asthma? Chest. 2005;128:2954-2962. Kanazawa H. Anticholinergic agents in asthma: chronic bronchodilator therapy, relief of acute severe asthma, reduction of chronic viral inflammation and prevention of airway remodeling. Curr Opin Pulm Med. 2006;12:60-67. Salpeter SR, Buckley NS. Author’s response: Asthma-related death rate. Available at: http://www.annals.org/cgi/eletters/144/12/904#3689. Accessed February 22, 2009. Wijesinghe M, Perrin K, Harwood M, et al. The risk of asthma mortality with inhaled long acting beta-agonists. Postgrad Med J. 2008;84:467-472. (online) Studies Included in Meta-Analysis Study, Reference Duration Intervention No. (n) Mean Age Dropout (%) Percent on ICS Comments Foradil 040 trial20 12 wk -agonist Control Foradil 041 trial21 12 wk -agonist Control Foradil 230729 trial 12 wk -agonist Control GSK pooled trials9 Not stated -agonist Control SMART22 28 wk -agonist Control Formoterol 12 g or 24 g BID Placebo 269 35.5 5.9 135 35.5 6.7 Formoterol 12 g and 24 g BID Placebo 275 32.6 6.2 45 141 33.5 6.4 49 Formoterol 12 g and 24 g BID Placebo 1054 38.8 13.8 65 514 37.8 15.2 66.7 Salmeterol, dose not stated Placebo 296 Not stated Not stated 0 298 Not stated Not stated 0 13,174 39.2 22.5 49 13,179 39.1 23.8 49 633 Not stated Not stated 100 642 Not stated Not stated 100 Salmeterol 50 g BID Placebo Not stated Phase 3 study sponsored by Novartis (Basel, Switzerland), NDA20-831, Protocol 040. There was 1 nonfatal asthma intubation in patient aged ⬎ 12 y. Reported in Novartis FDA briefing material.10 Not reported in original trial. Phase 3 study sponsored by Novartis, NDA20-831, Protocol 041 One respiratory arrest with nonfatal intubation in patient aged ⬎ 12 y. One asthma death in 66-year-old woman not on ICS, receiving formoterol 24 g BID. Events reported in Novartis FDA briefing material.10 Asthma death reported in original trial but thought not to be related to study drug. Phase 4 safety study sponsored by Novartis, For258D-2307. One asthma intubation in a 53-year-old African-American man receiving formoterol 12 g BID and 1 asthma intubation in a 51-year-old Caucasian man receiving formoterol 24 g BID. Both events were reported in a clinical safety review on FDA website in 2005, but they were not reported in the Novartis FDA briefing material in 2008. Pooled trial data in GSK (Brentford, London, England) FDA briefing material. Three asthma intubations in the salmeterol group and 1 asthma intubation in the control group. All events occurred in randomized placebo-controlled trials without ICS use. After communication with Steven Yancey of GSK on 2/2/09, we were informed that GSK declined to provide individual triallevel information. Phase 4 safety study, sponsored by GSK, Trial SLGA5011. There were 13 asthma deaths and 24 intubations in the salmeterol group, and 3 asthma deaths and 19 intubations in the placebo group. All events reported in original trial. Safety of Long-acting -Agonists Long-acting -Agonist Compared with Placebo, with Variable Corticosteroid Use Salpeter et al Table 1 Long-acting -Agonist with ICS Compared with ICS Alone GSK pooled trials9 Not stated -agonist Control Salmeterol, dose not stated Placebo Pooled trial data provided in GSK FDA briefing material. There were 8 asthma intubations in the salmeterol group and 3 asthma intubations in the placebo group. All events occurred in randomized placebocontrolled trials with concomitant ICS use in GSK database. After communication with Steven Yancey of GSK on 2/2/09, we were informed that GSK declined to provide individual trial-level information 328.e1 328.e2 Table 1 Continued Study, Reference Duration 23 Ind et al 24 wk Intervention -agonist Control Kelsen et al24 24 wk -agonist Control Kemp et al25 12 wk -agonist Control -agonist Control O’Byrne et al27 52 wk -agonist Control Von Berg et al28 12 wk -agonist Control Mean Age Dropout (%) Percent on ICS Salmeterol 50 g ⫹ fluticasone 250 g BID Fluticasone 250 or 500 g BID Salmeterol 42 g ⫹ beclomethasone 168 g BID Beclomethasone 336 g BID Salmeterol 42 g BID Placebo 173 44.8 15.7 100 329 44.8 11.4 100 239 42.4 20 100 244 42.0 20 100 252 42.0 9.9 100 254 41.6 18.5 100 Formoterol 4.5 g ⫹ budesonide 200 g or 400 g BID Budesonide 200 g or 400 g BID 869 34.8 16 100 862 35.4 16 100 Formoterol 4.5 ⫹ budesonide 80 g BID Budesonide 320 g BID 1834 35.5 3.2 100 926 36.0 3.1 100 Formoterol 4.5 g and 9 g BID Placebo 165 11.4 6.1 100 83 11.3 3.6 100 Comments Sponsored by GSK, Trial SLGB4010. There was 1 asthma death in the salmeterol/fluticasone group. Event reported in GSK briefing material9 and GSK-sponsored meta-analysis,14 so we removed the event from GSK pooled data. Not reported in original trial. Unpublished information received by Steven Yancey of GSK on 11/11/08. Sponsored by GSK, Trial SLGA5017. There was 1 asthma intubation in the salmeterol/beclomethasone group. Reported in GSK briefing material9 and GSK-sponsored meta-analysis,14 so we removed the event from GSK pooled data. Unpublished information received by Steven Yancey of GSK on 11/11/08. Sponsored by GSK, Trial SLGA5001. All patients on ICS, with 1 asthma intubation in the salmeterol group. Reported in original trial as respiratory failure, judged to be possibly related to study drug. Asthma intubation reported in meta-analysis by Jaeschke et al,12 but not reported in GSK-sponsored meta-analysis.9 After communication with Steven Yancey of GSK on 4/22/09, he informed us that this event was not reported in their pooled data. OPTIMA study sponsored by AstraZeneca (Wilmington, DE), Trial SD-037-0345. One asthma intubation due to status asthmaticus in formoterol/budesonide group, with subsequent death due to septic shock. Reported in AstraZeneca FDA briefing material as asthma intubation;11 reported in AstraZeneca-sponsored meta-analysis as asthma death.7 No event reported in original trial. We report event as intubation in our analysis. Unpublished information received from Anders Ottosson of AstraZeneca on 11/5/08. Sponsored by AstraZeneca, Trial SD-039-0673. One asthma death in formoterol/budesonide group. Reported in AstraZeneca-sponsored meta-analysis as death due to asthma in 65-year-old woman.7 Not reported as a drug-related asthma event in AstraZeneca FDA briefing material11 or original trial. Unpublished information received by Anders Ottosson of AstraZeneca on 11/5/08. Sponsored by AstraZeneca, Trial SD-037-0003 (sponsorship not disclosed in trial). All patients receiving inhaled or oral corticosteroids. One death reported in AstraZeneca-sponsored meta-analysis as asthma-related respiratory failure and death in 13-year-old boy who was taking ICS.7 Death reported in trial as due to subarachnoid hemorrhage and judged unlikely to be due to study drug. Not reported as a drug-related asthma event in AstraZeneca FDA briefing material.11 Unpublished information received by Anders Ottosson of AstraZeneca on 11/5/08. BID ⫽ 2 times per day; FDA ⫽ Food and Drug Administration; GSK ⫽ GlaxoSmithKline; ICS ⫽ inhaled corticosteroid; SMART ⫽ Salmeterol Multi-center Asthma Research Trial. The American Journal of Medicine, Vol 123, No 4, April 2010 O’Byrne et al26 52 wk No. (n)