Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
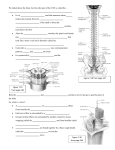
PNS Chapter 13 Peripheral Nervous System (PNS) • Provides links from and to world outside body • All neural structures outside brain – Sensory receptors – Peripheral nerves and associated ganglia – Efferent motor endings Sensory Receptors • Specialized to respond to changes in environment (stimuli) • Activation results in graded potentials that trigger nerve impulses • Sensation (awareness of stimulus) and perception (interpretation of meaning of stimulus) occur in brain Classification of Receptors • Based on – Type of stimulus they detect – Location in body – Structural complexity Classification by Stimulus Type • Mechanoreceptors—respond to touch, pressure, vibration, and stretch • Thermoreceptors—sensitive to changes in temperature • Photoreceptors—respond to light energy (e.g., retina) • Chemoreceptors—respond to chemicals (e.g., smell, taste, changes in blood chemistry) • Nociceptors—sensitive to pain-causing stimuli (e.g. extreme heat or cold, excessive pressure, inflammatory chemicals) Classification by Location • Exteroceptors – Respond to stimuli arising outside body – Most special sense organs • Interoceptors (visceroceptors) – Respond to stimuli arising in internal viscera and blood vessels • Proprioceptors – Inform brain of body movements Classification by Receptor Structure • General senses (simple receptors) – Tactile sensations (touch, pressure, stretch, vibration), temperature, pain, and muscle sense – Modified dendritic endings of sensory neurons • Non-encapsulated (free nerve endings) • Encapsulated • Special senses – Vision, hearing, equilibrium, smell, and taste (Chapter 15) Sensory Integration • Somatosensory system – part of sensory system serving body wall and limbs – Receives inputs from Exteroceptors, proprioceptors, and interoceptors – Input relayed toward head, but processed along way – Levels of neural integration in sensory systems: 1. Receptor level—sensory receptors 2. Circuit level—processing in ascending pathways 3. Perceptual level—processing in cortical sensory areas Adaptation of Sensory Receptors • Adaptation is change in sensitivity in presence of constant stimulus – Phasic (fast-adapting) receptors signal beginning or end of stimulus • Examples - receptors for pressure, touch, and smell – Tonic receptors adapt slowly or not at all • Examples - nociceptors and most proprioceptors Processing at the Perceptual Level • Interpretation of sensory input depends on specific location of target neurons in sensory cortex • Aspects of sensory perception: – Perceptual detection—ability to detect a stimulus (requires summation of impulses) – Magnitude estimation—intensity coded in frequency of impulses – Spatial discrimination—identifying site or pattern of stimulus (studied by two-point discrimination test) Perception of Pain • Warns of actual or impending tissue damage protective action • Impulses travel on fibers that release neurotransmitters glutamate and substance P • Some pain impulses are blocked by inhibitory endogenous opioids (e.g., endorphins) • All perceive pain at same stimulus intensity, but pain tolerance varies – "Sensitive to pain" means low pain tolerance, not low pain threshold – Pain tolerance, and response to pain medication, is rooted in genetics. Homeostatic Imbalance • Hyperalgesia (pain amplification), – NMDA receptors-allow spinal cord to "learn" hyperalgesia • Phantom limb pain – felt in limb no longer present – epidural use during anesthesia to prevent Visceral and Referred Pain • Stimulation of visceral organ receptors – Felt as vague aching, gnawing, burning – Activated by tissue stretching, ischemia, chemicals, muscle spasms • Referred pain – Pain from one body region perceived from different region – Visceral and somatic pain fibers travel in same nerves; brain assumes stimulus from common (somatic) region Structure of a Nerve • Connective tissue coverings include: – Endoneurium—loose connective tissue that encloses axons and their myelin sheaths – Perineurium—coarse connective tissue that bundles fibers into fascicles – Epineurium—tough fibrous sheath around a nerve Classification of Nerves • Most nerves are mixtures of afferent and efferent fibers and somatic and autonomic (visceral) fibers – Pure sensory (afferent) or motor (efferent) nerves are rare – Types of fibers? • Peripheral nerves classified as cranial or spinal nerves • Ganglia – Contain neuron cell bodies associated with nerves Regeneration of Nerve Fibers • Mature neurons are amitotic • If the soma of a damaged nerve is intact, axon will regenerate • Involves coordinated activity among: – Macrophages—remove debris – Schwann cells—form regeneration tube and secrete growth factors – Axons—regenerate damaged part • CNS oligodendrocytes bear growth-inhibiting proteins that prevent CNS fiber regeneration Endoneurium Schwann cells Droplets of myelin 1 The axon becomes fragmented at the injury site. Fragmented axon Site of nerve damage Figure 13.4 (1 of 4) Schwann cell Macrophage 2 Macrophages clean out the dead axon distal to the injury. Figure 13.4 (2 of 4) Aligning Schwann cells form regeneration tube 3 Axon sprouts, or filaments, grow through a regeneration tube formed by Schwann cells. Fine axon sprouts or filaments Figure 13.4 (3 of 4) Schwann cell Site of new myelin sheath formation 4 The axon regenerates and a new myelin sheath forms. Single enlarging axon filament Figure 13.4 (4 of 4) Cranial Nerves • Twelve pairs of nerves associated with the brain • Most are mixed in function; two pairs are purely sensory • Each nerve is identified by a number (I through XII) and a name “On occasion, our trusty truck acts funny—very good vehicle anyhow” Frontal lobe Temporal lobe Infundibulum Facial nerve (VII) Vestibulocochlear nerve (VIII) Glossopharyngeal nerve (IX) Vagus nerve (X) Accessory nerve (XI) Hypoglossal nerve (XII) Filaments of olfactory nerve (I) Olfactory bulb Olfactory tract Optic nerve (II) Optic chiasma Optic tract Oculomotor nerve (III) Trochlear nerve (IV) Trigeminal nerve (V) Abducens nerve (VI) Cerebellum Medulla oblongata (a) Figure 13.5 (a) Cranial nerves I – VI I II III IV V Olfactory Optic Oculomotor Trochlear Trigeminal VI Abducens Cranial nerves VII – XII VII Facial VIII Vestibulocochlear IX X XI XII (b) Glossopharyngeal Vagus Accessory Hypoglossal Sensory function Motor function PS* fibers Yes (smell) Yes (vision) No No Yes (general sensation) No No Yes Yes Yes No No Yes No No No Yes No Sensory function Motor function PS* fibers Yes (taste) Yes (hearing and balance) Yes Some Yes No Yes (taste) Yes (taste) No No Yes Yes Yes Yes Yes Yes No No *PS = parasympathetic Figure 13.5 (b) I: The Olfactory Nerves • Purely sensory (olfactory) function • Afferent impulses for sense of smell • Injury diagnosis: partial or total loss of smell (anosmia) Table 13.2 II: The Optic Nerves • Pass through the optic canals, converge and partially cross over at the optic chiasma • Purely sensory (visual) function • Injury diagnosis: blindness or partial loss of vision in affected eye Table 13.2 III: The Oculomotor Nerves • Functions in raising the eyelid, directing the eyeball, constricting the iris (parasympathetic), and controlling lens shape • Injury: eye cannot be moved (up, down, inward) or rotates laterally when at rest, upper eyelid droops, double vision, and difficulty focusing on close objects Table 13.2 IV: The Trochlear Nerves • Primarily a motor nerve that directs the eyeball • Injury: double vision, reduced ability to rotate eye inferolaterally • Tested w/ III Table 13.2 V: The Trigeminal Nerves • Three divisions – – – – Ophthalmic (V1) Maxillary (V2) Mandibular (V3) Convey sensory impulses from various areas of the face (V1) and (V2), and supplies motor fibers (V3) for mastication • Injury: produces excruciating pain for a few seconds to a minute, recurring many times a day and by various causes (brushing teeth, breeze hitting the face) VI: The Abducens Nerves • Primarily a motor nerve, innervating the lateral rectus muscle • Injury: eye cannot be moved laterally, at rest eyeball rotates medially VII: The Facial Nerves • Chief motor nerves of the face with 5 major branches – Temporal, zygomatic, buccal, mandibular, cervical • Motor functions include facial expression, parasympathetic impulses to lacrimal and salivary glands • Sensory function (taste) from the anterior two-thirds of the tongue • Injury: Bell’s palsy VIII: The Vestibulocochlear Nerves • Mostly sensory function; small motor component for adjustment of sensitivity of receptors • Injury: – Cochlear: deafness – Vestibular: dizziness, rapid involuntary eye movements, loss of balance, nausea, vomiting IX: The Glossopharyngeal Nerves • Motor functions: innervate part of the tongue and pharynx for swallowing, and provide parasympathetic fibers to the parotid salivary glands • Sensory functions: fibers conduct taste and general sensory impulses from the pharynx and posterior tongue, and impulses from carotid chemoreceptors and baroreceptors • Injury: Impaired swallowing or taste X: The Vagus Nerves • Fibers from the medulla exit the skull via the jugular foramen • Most motor fibers are parasympathetic fibers that help regulate the activities of the heart, lungs, and abdominal viscera • Sensory fibers carry impulses from thoracic and abdominal viscera, baroreceptors, chemoreceptors, and taste buds of posterior tongue and pharynx X: The Vagus Nerves • Injury: Hoarseness or loss of voice, difficulty swallowing, impaired digestive system motility. • Total destruction is incompatible with life XI: The Accessory Nerves • Rootlets pass into the cranium via each foramen magnum • Accessory nerves exit the skull via the jugular foramina to innervate the trapezius and sternocleidomastoid muscles • Injury: head turns toward side of injury, shrugging of that shoulder difficult XII: The Hypoglossal Nerves • Innervate extrinsic and intrinsic muscles of the tongue that contribute to swallowing and speech • Injury: difficulties in speech/swallowing, problems with the tongue. Spinal Nerves • 31 pairs of mixed nerves named according to their point of issue from the spinal cord – 8 cervical (C1–C8) – 12 thoracic (T1–T12) – 5 Lumbar (L1–L5) – 5 Sacral (S1–S5) – 1 Coccygeal (C0) Spinal Nerves: Roots • Each spinal nerve connects to the spinal cord via two roots – Ventral roots • Contain motor (efferent) fibers from the ventral horn motor neurons – Dorsal roots • Contain sensory (afferent) fibers from sensory neurons in the dorsal root ganglia • Dorsal + Ventral = spinal nerves Spinal Nerves: Rami • Each spinal nerve branches into mixed rami – Dorsal ramus – Ventral ramus - larger – Meningeal branch – tiny, reenters vertebral canal, innervates meninges and blood vessels – Rami communicantes (autonomic pathways) join ventral rami in thoracic region Spinal Nerves: Rami • All ventral rami (except T2–T12) form nerve plexuses (cervical, brachial, lumbar, and sacral) • Back innervated by dorsal rami via several branches • Ventral rami of T2–T12 as intercostal nerves supply muscles of ribs, anterolateral thorax, and abdominal wall • Spinal roots get longer as move inferiorly in cord – Lumbar and sacral roots extend as cauda equina Spinal Nerves: Plexuses • Within plexus fibers criss-cross – Each branch contains fibers from several spinal nerves – Fibers from as single ventral ramus go to body periphery via several routes • Each limb muscle innervated by more than one spinal nerve Cervical Plexus and the Neck • Formed by ventral rami of C1–C4 • Most branches form cutaneous nerves – Innervate skin of neck, ear, back of head, and shoulders – Other branches innervate neck muscles Phrenic nerve • Major motor and sensory nerve of diaphragm (receives fibers from C3–C5) • Irritation hiccups Brachial Plexus and Upper Limb • Formed by ventral rami of C5–C8 and T1 (and often C4 and/or T2) • Gives rise to nerves that innervate upper limb Figure 13.10a The brachial plexus. Anterior divisions Posterior divisions Trunks Roots Dorsal scapular Nerve to subclavius Suprascapular Cords Roots (ventral rami): C4 C5 C6 Posterior divisions C7 Lateral C8 Posterior T1 Upper Middle Trunks Lower Long thoracic Medial Medial pectoral Lateral pectoral Axillary Upper subscapular Musculocutaneous Lower subscapular Radial Thoracodorsal Median Ulnar Roots (rami C5–T1), trunks, divisions, and cords © 2013 Pearson Education, Inc. Medial cutaneous nerves of the arm and forearm Brachial Plexus: Five Important Nerves • • • • • Axillary Musculocutaneous Median Ulnar Radial Lumbar Plexus • Arises from L1–L4 • Innervates thigh, abdominal wall, and psoas muscle • Femoral nerve—innervates quadriceps and skin of anterior thigh and medial surface of leg • Obturator nerve—passes through obturator foramen to innervate adductor muscles Figure 13.11 The lumbar plexus. Ventral rami Ventral rami: L1 L2 Iliohypogastric Ilioinguinal Iliohypogastric Femoral Ilioinguinal Lateral femoral cutaneous Genitofemoral Lateral femoral cutaneous L3 Obturator L4 Anterior femoral cutaneous Saphenous Obturator Femoral L5 Lumbosacral trunk Ventral rami and major branches of the lumbar plexus Distribution of the major nerves from the lumbar plexus to the lower limb Sacral Plexus • Arises from L4–S4 • Serves the buttock, lower limb, pelvic structures, and perineum • Sciatic nerve – Longest and thickest nerve of body – Innervates hamstring muscles, adductor magnus, and most muscles in leg and foot – Composed of two nerves: tibial and common fibular Innervation of Skin • Dermatome: the area of skin innervated by the cutaneous branches of a single spinal nerve • All spinal nerves except C1 participate in dermatomes • Most dermatomes overlap, so destruction of a single spinal nerve will not cause complete numbness Stimulus Reflex Arc Skin 1 Receptor Interneuron 2 Sensory neuron 3 Integration center 4 Motor neuron 5 Effector Spinal cord (in cross section) Figure 13.14 Spinal Reflexes • Spinal somatic reflexes – Integration center is in the spinal cord – Effectors are skeletal muscle • Testing of somatic reflexes is important clinically to assess the condition of the nervous system Stretch and Golgi Tendon Reflexes • For skeletal muscle activity to be smoothly coordinated, proprioceptor input is necessary – Muscle spindles inform the nervous system of the length of the muscle – Golgi tendon organs inform the brain as to the amount of tension in the muscle and tendons Stretch Reflexes • Maintain muscle tone in large postural muscles • Cause muscle contraction in response to increased muscle length (stretch) • How a stretch reflex works: – Stretch activates the muscle spindle – sensory neurons synapse directly with motor neurons in the spinal cord – motor neurons cause the stretched muscle to contract Stretch Reflexes • All stretch reflexes are monosynaptic and ipsilateral • Reciprocal inhibition also occurs – fibers synapse with interneurons that inhibit the motor neurons of antagonistic muscles • Example: In the patellar reflex, the stretched muscle (quadriceps) contracts and the antagonists (hamstrings) relax Stretched muscle spindles initiate a stretch reflex, causing contraction of the stretched muscle and inhibition of its antagonist. The events by which muscle stretch is damped 1 When muscle spindles are activated 2 The sensory neurons synapse directly with alpha motor neurons (red), which excite extrafusal fibers by stretch, the associated sensory of the stretched muscle. Afferent fibers also neurons (blue) transmit afferent impulses synapse with interneurons (green) that inhibit motor at higher frequency to the spinal cord. neurons (purple) controlling antagonistic muscles. Sensory neuron Cell body of sensory neuron Initial stimulus (muscle stretch) Spinal cord Muscle spindle Antagonist muscle 3a Efferent impulses of alpha motor neurons 3b Efferent impulses of alpha motor cause the stretched muscle to contract, which resists or reverses the stretch. neurons to antagonist muscles are reduced (reciprocal inhibition). Figure 13.17 (1 of 2) The patellar (knee-jerk) reflex—a specific example of a stretch reflex 2 Quadriceps (extensors) 1 3a 3b 3b Patella Muscle spindle Spinal cord (L2–L4) Hamstrings (flexors) Patellar ligament 1 Tapping the patellar ligament excites muscle spindles in the quadriceps. 2 Afferent impulses (blue) travel to the spinal cord, where synapses occur with motor neurons and interneurons. 3a The motor neurons (red) send + – Excitatory synapse Inhibitory synapse activating impulses to the quadriceps causing it to contract, extending the knee. 3b The interneurons (green) make inhibitory synapses with ventral horn neurons (purple) that prevent the antagonist muscles (hamstrings) from resisting the contraction of the quadriceps. Figure 13.17 (2 of 2) Golgi Tendon Reflexes • Polysynaptic reflexes • Help to prevent damage due to excessive stretch • Important for smooth onset and termination of muscle contraction Golgi Tendon Reflexes • Produce muscle relaxation (lengthening) in response to tension – Contraction or passive stretch activates Golgi tendon organs – Afferent impulses are transmitted to spinal cord – Contracting muscle relaxes and the antagonist contracts (reciprocal activation) – Information transmitted simultaneously to the cerebellum is used to adjust muscle tension 1 Quadriceps strongly 2 Afferent fibers synapse contracts. Golgi tendon organs are activated. with interneurons in the spinal cord. Interneurons Quadriceps (extensors) Spinal cord Golgi tendon organ Hamstrings (flexors) + Excitatory synapse – Inhibitory synapse 3a Efferent impulses 3b Efferent to muscle with stretched tendon are damped. Muscle relaxes, reducing tension. impulses to antagonist muscle cause it to contract. Figure 13.18 Flexor and Crossed-Extensor Reflexes • Flexor (withdrawal) reflex – Initiated by a painful stimulus – Causes automatic withdrawal of the threatened body part – Ipsilateral and polysynaptic Flexor and Crossed-Extensor Reflexes • Crossed extensor reflex – Occurs with flexor reflexes in weight-bearing limbs to maintain balance – Consists of an ipsilateral flexor reflex and a contralateral extensor reflex • The stimulated side is withdrawn (flexed) • The contralateral side is extended + Excitatory synapse – Inhibitory synapse Interneurons Efferent fibers Afferent fiber Efferent fibers Extensor inhibited Flexor stimulated Site of stimulus: a noxious stimulus causes a flexor reflex on the same side, withdrawing that limb. Arm movements Flexor inhibited Extensor stimulated Site of reciprocal activation: At the same time, the extensor muscles on the opposite side are activated. Figure 13.19