Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
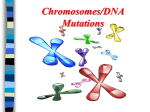
[Cell Cycle 2:3, 202-210, May/June 2003]; © 2003 Landes Bioscience Review Multistep Carcinogenesis A Chain Reaction of Aneuploidizations Peter Duesberg* Ruhong Li Department of Molecular and Cell Biology; Donner Laboratory; UC Berkeley; Berkeley, California USA *Correspondence to: Peter Duesberg; Department of Molecular and Cell Biology; Donner Laboratory; UC Berkeley; Berkeley, California 94720 USA; Tel.: 510.642.6549; Fax: 510.643.6455; Email: [email protected] Received 04/05/03; Accepted 04/10/03 Previously published online as a Cell Cycle Paper in Press at: http://www.landesbioscience.com/journals/cc/toc.php?volume=2&issue=3 KEY WORDS Aneuploidy-dependent malignancy, Cancerspecific aneusomies, Genetic instability, Aneuploidydependent karyotype instability, Aneuploidydependent gene mutation, Mutator genes, Nonmutagenic carcinogens, Drug-resistance, Reversible phenotypes, Immortality We are indebted to the Abraham J. and Phyllis Katz Foundation (New York), Robert Leppo (philanthropist, San Francisco), an American foundation that prefers to be anonymous, other private sources, the Deutsche Krebshilfe and the Forschungsfonds der Fakultaet for Klinische Medizin Mannheim (Germany) for support. 202 ABSTRACT Carcinogenesis is a multistep process in which new, parasitic and polymorphic cancer cells evolve from a single, normal diploid cell. This normal cell is converted to a prospective cancer cell, alias "initiated", either by a carcinogen or spontaneously. The initiated cell typically does not have a new distinctive phenotype yet, but evolves spontaneously—over months to decades—to a clinical cancer. The cells of a primary cancer also evolve spontaneously towards more and more malignant phenotypes. The outstanding genotype of initiated and cancer cells is aneuploidy, an abnormal balance of chromosomes, which increases and varies in proportion with malignancy. The driving force of the spontaneous evolution of initiated and cancerous cells to ever more abnormal phenotypes is said to be their "genetic instability". However, since neither the instability of cancer phenotypes nor the characteristically slow kinetics of carcinogenesis are compatible with gene mutation, we propose here that the driving force of carcinogenesis is the inherent instability of aneuploid karyotypes. Aneuploidy renders chromosome structure and segregation errorprone, because it unbalances mitosis proteins and the many teams of enzymes that synthesize and maintain chromosomes. Thus, carcinogenesis is initiated by a random aneuploidy, which is induced either by a carcinogen or spontaneously. The resulting karyotype instability sets off a chain reaction of aneuploidizations, which generate ever more abnormal and eventually cancer-specific combinations and rearrangements of chromosomes. According to this hypothesis the many abnormal phenotypes of cancer are generated by abnormal dosages of thousands of aneuploid, but un-mutated genes. Carcinogenesis is a very rare process in which a normal cell is converted to a cancer cell via multiple “steps” or “stages” of cellular evolution, which correspond to various pre-neoplastic and neoplastic phenotypes and genotypes.1-4 The clinical and biological phenotypes of the multiple steps of carcinogenesis include hyperplasia, dysplasia, abnormal morphology, anaplasia or dedifferentiation, drug- and multi-drug resistance, immortality, altered histocompatibility including even transplantability to some heterologous species and susceptibility to some heterologous viruses, abnormal metabolism, autonomous growth, invasiveness, and metastasis.1,5-12 Based on various genetic and cytogenetic markers, including structurally altered or marker chromosomes, most cancers are clonal, i.e., derived from a single cell.3,13-15 However, a minority is polyclonal.1,16,17 Despite their clonal origin, “the structure and behavior of tumors are determined by numerous, abnormal characters that, within wide limits, are independently variable, capable of highly varied combinations and assortments and liable to independent progression.”18,19 As a result of this “genetic instability”3 hardly any two cells from a given cancer are ever the same.1,20-26,62,137 Indeed, the specific karyotypes and phenotypes of individual cancer cells can vary at rates of up to a few percent per cell generation and are thus many orders of magnitude less stable than would be expected from conventional gene mutations.11,12,24,27-29 But the mechanism of this genetic instability of cancer cells is still a matter of debate.30-33 In further contrast to gene mutation, the kinetics of carcinogenesis are exceedingly slow. After a sufficient, alias “initiating,” dose of carcinogen it takes a cell a minimum of months and many cell generations to develop clinically detectable cancerous phenotypes in experimental rodents.2,14,34,192 Likewise, experimental transformation of normal, diploid rodent cells to tumorigenic counterparts in vitro takes a minimum of months.23,35 Even the highest survivable doses of carcinogens, supplemented by treatments with tumor promoters, can only accelerate experimental carcinogenesis a few-fold.2,34,36,37,177,192 Carcinogenesis in humans takes even decades from an occupational or accidental exposure to a dose of carcinogen that is sufficient to eventually cause cancer.1,5,14,38-40 Cell Cycle 2003; Vol. 2 Issue 3 MULTISTEP CARCINOGENESIS Transformation of diploid human cells with carcinogens in vitro takes about half a year, and is much less efficient than transformation of rodent cells.41,42 Spontaneous carcinogenesis in humans from unknown initiation any time after birth to clinical phenotypes is estimated to take over 50 years, because the risk of spontaneous cancer rises exponentially, over 1000-fold, from negligible levels under the age of 50 to over 400 cases per million people per year at the age of 80.14,43-45 By contrast, classical gene mutation generates a new and final phenotype within one cell generation, as for example in bacteria. During the long lag between initiation and clinical phenotypes, the prospective cancer cell “progresses” first through various stages of “characters that have no discernible effect at all on clinical behaviour”, such as increased susceptibility to transformation by additional carcinogens, hyperplasia, altered cell morphology and aneuploidy.1 Aneuploidy is defined as an abnormal balance of either intact chromosomes or segments of chromosomes or both.6,46,84 But once the first clinical phenotypes appear, e.g., dysplasia and carcinoma in situ, progression to more malignant phenotypes, such as metastasis, abnormal morphologies, abnormal metabolism and drug-resistance, typically occurs at much higher rates.1,13,47 Since the multiplicity of the malignant phenotypes is not fixed, there is no absolute definition of a cancer cell.1 Aneuploidy stands out as the most consistent marker of malignancy. A simple aneuploidy is the earliest and most distinctive pre-neoplastic genotype.3,6,17,26,48-61 By contrast, a complex aneuploidy is the most typical neoplastic genotype.53,57-59,62-64 The more aneuploid the cell the higher its malignancy.3,13,47,53,62,65-75 According to Foulds, “In general the abnormalities of the karyotypes were of greater complexity in malignant than in non-malignant lesions…”.1 Thus, the degree of malignancy is directly proportional to the degree of aneuploidy. The instability of the karyotype of cancer cells is also proportional to the degree of aneuploidy: It increases from undetectable rates of gains, losses and rearrangements of chromosomes per mitosis in diploid cells to a few percent in highly aneuploid cells.28,29,50 Even the low degrees of aneuploidy of pre-neoplastic cells coincide with karyotype-instability.48,53,60 Thus carcinogenesis is fundamentally different from mutation: It is very slow, timed from an initiating and sufficient dose of carcinogen. It is associated with aneuploidy from its initiation. After initiation, it generates abnormal phenotypes spontaneously, i.e. without further carcinogens, including eventually cancer-specific phenotypes. These phenotypes are unstable and thus typically progress from bad to worse,1 or shift from drug-sensitive to drug-resistant, or from one morphological grade or metabolic state to another—unlike conventional gene mutations.2,4,11,12 MECHANISMS OF CARCINOGENESIS Despite over a century of cancer research, the mechanism of carcinogenesis is still a matter of debate, primarily between two schools of thought.33,76-80 One school holds that cancer-specific phenotypes are the result of multiple, specific gene mutations, which either generate dominant oncogenes, or inactivate recessive tumor suppressor genes.2,77,81-86 The competing school holds that cancerspecific phenotypes are the results of the thousands of normal genes whose dosage is altered by reassortments of the corresponding chromosomes or aneuploidy.6,35,76 www.landesbioscience.com ARE THE MULTIPLE STEPS OF CARCINOGENESIS MULTIPLE MUTATIONS? Since the risk of mutations increases linearly with age, but the risk of cancer increases exponentially, over 1000-fold, the proponents of the mutation hypothesis postulate that between 4 and 7 mutations are necessary for carcinogenesis.14,40,43-45 Only complete sets of these genes are thought to cause cancer.14,45,83 However, the problem of where the huge number of random mutations would come from that is necessary to mutate 4–7 specific genes has not been solved. Based on the normal, spontaneous gene mutation rate of about 10-6 per mitosis,87 only 1 in 1024–1042 human cells would ever become cancer cells.6,31,88,89 Since humans consist of 1014 cells,14 only 1 in 1010–1028 humans would ever get cancer. This number would be even lower, if the mutation rates of the recessive cancer genes, as for example the hypothetical tumor suppressor genes, are squared. In other words cancer would hardly exist. To solve this problem, the proponents of the mutation hypothesis have postulated that prior to mutation of prospective cancer genes, another class of cellular genes must be mutated to mutator genes, which in turn would mutate prospective cancer genes to real cancer genes.3,32,88,90,91 The presence of such mutator genes, early in carcinogenesis, could then also explain the spontaneous, or carcinogenindependent, progression of initiated cells to cancer cells. However, in the words of Breslow and Goldsby, “a mutator gene really begs the question … one is left with the problem of accounting for such a high frequency of mutator genes.”92 But, the origin of multiple specific mutations in the same cell is not the only problem of the mutation hypothesis. According to Cairns’ Cancer, Science and Society, “One of the problems is that mutations lead to loss of function rather than creation of new function.”14 Creation of cancer-specific phenotypes is particularly hard to reconcile with mutation because of their multiplicity and extraordinary complexity. Even ardent proponents of the mutation hypothesis acknowledge this problem: “our understanding of the biology of these tumors will become a phenomenology of unlimited complexity.”93 Thus, how could a prospective cancer cell ever survive the “loss of function” that is associated with the high mutation rates, which are necessary to generate the 4–7 specific mutations and possibly further “unlimited complexity” of cancer cells? Since the probability that any one of the 35,000 human genes191 is mutated is 1:35,000, but the probability that 4–7 genes are mutated is only 1:(35,000)4-7, virtually all genes of a prospective cancer cell would have to be mutated before it could turn into a cancer cell. Suppose then a cell with a mutator gene has suffered 1000 random mutations, its chance to become transformed into a cancer cell by 4 specific mutations is only 1 in 1.5 million, and after it has suffered 5000 random mutations, this chance is still only 1 in 2400. But how could any cell carry out the many cell cycles, that set apart initiation from completion of carcinogenesis, in the face of so many mutations? In view of these questions, we have reexamined the merits of the mutation hypothesis by testing whether it could predict a list of 14 basic facts of carcinogenesis, that are summarized in Table 1 (next page). Since the hypothesis fails to predict any of these facts, we conclude that it is not a satisfactory explanation of carcinogenesis. Cell Cycle 203 MULTISTEP CARCINOGENESIS Table 1 DISCREPANCIES BETWEEN THE PREDICTIONS OF THE Predictions of the mutation hypothesis GENE MUTATION-CANCER HYPOTHESIS AND THE FACTS Facts 1 Carcinogens are mutagens. But, half of all known carcinogens, such as polycyclic aromatic hydrocarbons, asbestos, hormones, mineral oil, hydrazine, solid bodies, nickel and cytoplasmic radiations are not mutagenic.6,94-96,193 2 Cancer-phenotypes are determined by cancerspecific mutations. But, about half of all solid cancers of any kind lack hypothetical cancer genes or oncogenes.31,89,97-100,193 In other words oncogenes do “not impart distinct clinical properties on most tumors.”99 Yet, “phenocopies” of known oncogenes are said to cause those cancers in which known oncogenes can not be found.97,101 3 Cancer-specific mutations confer selective advantages for carcinogenesis. But, cancers contain up to 100 times more selectively neutral or silent mutations than normal cells, even in tumorsuppressor genes.32 4 Cancer-causing mutations are present in all transformed cells of a clonal cancer. But, the mutant oncogene K-ras is non-clonal in human colon cancer,102,103 mutant Kras, H-ras and myc are non-clonal in prostate cancers,104,105 mutant H- and N-ras are non-clonal in melanoma,106,107 mutant her/EGFR/neu/erbB-2 is non-clonal in esophageal Barrett's cancers,108 in bladder cancers,109 in malignant gliomas,110,111 and in breast cancers112 together with other non-clonal, hypothetical oncogenes.113 5 Cancers are maintained by the expression of cancer genes But, hypothetical cancer genes are un-expressed in many cancer cells.78,114-116 6 Normal cells are transformed into cancer cells by oncogenes. But, transgenic mice, carrying hypothetical oncogenes in every cell of their body, are viable and fertile and have either a normal or just a moderately higher than normal risk of developing a clonal (not polyclonal!) cancer.6,117-122 7 Since only 4–7 gene mutations are thought to be necessary for carcinogenesis,14,83,84,123 only small numbers of genes should be abnormally expressed in cancer cells. But, thousands of genes are abnormally expressed in cancer cells,114-116 “the sine qua non of malignant transformation”.4 8 Inheritance of 3–6, of the 4–7 mutations thought to to be necessary for carcinogenesis, predicts solid cancer at very young age from a single, somatic mutation in any of billions of susceptible cells. But, the incidence of solid cancer at young age is negligible,14,43-45; For key, see Table 2(#6) 9 In view of the low rates of spontaneous gene mutation, 10-6 per mitosis (see text), mutator genes are necessary for carcinogenesis—even for the spontaneous “progression” of “initiated” cells to cancer cells. But, “mutator genes” are only detectable in a small minority of cancers.24,29,31,32,124-126 And the gene mutation rates of many cancers are normal.127,128 Moreover, mutator genes are typically only detectable at late stages of carcinogenesis, suggesting that they are consequences of neoplastic development.128,129 10 The majority of cancers, ie. those without mutator genes, are genetically stable, like conventional mutations. But, all cancer cells are, more or less, genetically unstable.1,3,11,12,48,60 11 Genetic instability of cancer cells is proportional to the presence and nature of mutator genes. Instead, genetic instability of cancers is proportional to the degree of aneuploidy (see text).28,50,130 12 Congenital mutator genes increase the risk of all cancers. But, the mutator gene of Xeroderma Pigmentosum, which is postulated to cause skin cancer, does not increase the risk of non-skin cancers.131; For key, see Table 2(#1) 13 Certain mutant phenotypes of cancer cells, such as Yet, despite 3 billion years of mutation, none of these desirable phenotypes are ever immortality, resistance to singular or even multiple found in normal organisms! For key, see Table 2(#6) cytotoxic drugs, and resistance to cytotoxic viruses, should be highly attractive for normal animals and humans. 14 Cancer cells are diploid, differing from normal cells only in 4–7 specific mutations. But, unlike all conventional gene mutations, cancers are aneuploid (see below).35,76,77 ARE THE MULTIPLE STEPS OF CARCINOGENESIS MULTIPLE ANEUPLOIDIZATIONS? In an effort to find an alternative cancer hypothesis, we decided to search the literature for facts that are neglected by the mutation hypothesis. Surprisingly, we did not have to look very long to find aneuploidy. But despite a preponderance of evidence in support of the hypothesis that aneuploidy may cause cancer; there is currently a strong bias against this hypothesis.132 In the following we describe: 1. the evidence for aneuploidy; 2. the current bias against the aneuploidy hypothesis; and 3. a unifying hypothesis that answers the scientific objections that have been made against aneuploidy, and that explains all facts of carcinogenesis. 204 1. The Evidence for Aneuploidy as the Cause of Cancer. The following collection of facts lends correlative, functional and conceptual support to the aneuploidy-cancer hypothesis: Aneuploidy is ubiquitous in solid cancer.25,62,67,133 This is correlative proof for causation. Aneuploidy is also found in about half of all leukemias,134,135 the diploid half being hyperplasias.6 In contrast to the diploid leukemias, the cells of the aneuploid leukemias are dedifferentiated, immortal, and able to mutate to drug-resistance at high rates, just like solid cancers.12,136 The degree of malignancy is proportional to the degree of aneuploidy of a cancer: The more aneuploid the karyotype the more malignant the cancer (see above).3,13,47,59,60,65-75,137 Aneuploidy inevitably causes highly abnormal and complex phenotypes in lower and higher eukaryotes by altering the dosages Cell Cycle 2003; Vol. 2 Issue 3 MULTISTEP CARCINOGENESIS Figure 1. Multistep carcinogenesis via aneuploidizations. The vertical banded bars are chromosomes, the squares are normal diploid, and the circles are abnormal, aneuploid cells. Our model proposes that various specific chromosome assortments or aneusomies cause cancer. According to this model, carcinogenesis is initiated by a random aneuploidy, which is induced either by a carcinogen or spontaneously. Since aneuploidy unbalances mitosis proteins and the many enzymes that synthesize and maintain chromosomes, it renders chromosome segregation error-prone. The resulting karyotype instability sets off a chain reaction of aneuploidizations that generate ever more abnormal chromosome assortments, including non-viable and eventually cancer-specific chromosome assortments. The cancer-specific phenotypes—abnormal metabolism and morphology, invasiveness, drug-resistance, immortality and metastasis—are generated by the abnormal dosages of thousands of normal genes. Since aneuploid chromosome assortments are reversible, cancer-specific phenotypes such as drug-resistance can get lost at the same rates at which they are generated; likewise malignancy of non-tumorigenic cancer-normal-cell hybrids is recovered by loss of chromosomes. The model predicts the heterogeneous phenotypes and karyotypes of cancer cells as mixtures of selectively advantageous, cancer-specific and selectively neutral, random chromosome assortments. The model further predicts that both malignancy and karyotype instability are proportional to the degrees of aneuploidy, which is consistent with the literature (see text). of thousands of normal genes. This was first demonstrated in doublyfertilized sea urchins138 and has since been confirmed in aneuploid drosophila,139 plants,140 yeast,141,142 mice,143 and humans with Down’s syndrome and other congenital aneusomies.144-146 The probable basis of the abnormal phenotypes of aneuploidy is the abnormal dosage and expression of thousands of normal genes.146-148,152 The power of aneuploidy to generate abnormal phenotypes becomes immediately obvious if one compares the cell to a car factory and chromosomes to assembly lines. Unbalance these assembly lines and you get highly abnormal cars from entirely normal parts, e.g., cars with five wheels, no brakes, red headlights, etc. Most of these aneuploid cells would be non-functional, but a few would be able to out-compete normal cells in the permissive habitat of the body. The analogy also explains why a gene mutation, an altered assembly line worker in our analogy, is unlikely to generate the new properties of cancer cells: Any “activating” mutation82 would be buffered by the un-mutated genes of the assembly line working at normal rates.149 Likewise, most inactivating mutations would be buffered, since nearly all enzymes work in the cell at only a very small fraction of their capacity.150,151 Only very rare null mutations would bring the assembly line to a halt, in which case the second allele is usually www.landesbioscience.com sufficient to maintain normal cell function.152 However, if both assembly lines cease to work by mutations, the resulting cell is more likely to die than to develop the highly complex, new phenotypes of cancer cells (see above). Thus, aneuploidy is the simplest explanation for the many dominant and abnormal phenotypes of cancer cells.152 Aneuploidy has even been proposed as a cause of cancer over 100 years ago, first by von Hansemann because of suggestive evidence for its presence in epithelial cancer153 (the exact chromosome number of humans was only determined in 1956), and then by Boveri based on the discovery that aneuploidy can cause abnormal phenotypes in sea urchin embryos.138,154 The first experimental proof was obtained in 1930 by Winge who showed that the skin cancers induced in mice treated with tar were indeed aneuploid.137 2. The Current Bias Against Aneuploidy. In view of a series of new genetic and cytogenetic discoveries (see below), above all the discovery of heterogeneous and thus apparently unspecific karyotypes in most cancers, the original aneuploidy hypothesis was abandoned in the 1960s and 1970s. The resulting bias against the aneuploidycancer hypothesis is now based on the following arguments: 1) Aneuploidy is seen as a consequence or epiphenomenon of cancer. In the 1960s and 1970s it was discovered (a) that most cancers Cell Cycle 205 MULTISTEP CARCINOGENESIS Table 2 PREDICTIONS OF THE ANEUPLOIDY-CANCER HYPOTHESIS AND EXPERIMENTAL SUPPORT FROM THE LITERATURE Prediction Proofs of Principle in Literature 1 Carcinogens function as aneuploidogens. Refs.49,50,94; Key for Table 1 (#12); Aneuploidy by UV.181 2 Aneuploidy precedes and coincides with carcinogenesis. Refs.3,6,17,26,48-56,59,60,182 3 Cancer cells can evolve from aneuploid cells autocatalytically at rates that are dependent on the degree of aneuploidy (which is enhanced by additional aneuploidogens). Refs.47,64,152,177 4 Even after a sufficient dose of carcinogen, cancer does not appear for a long time—namely years to decades—because cancer-specific aneuploidies must evolve from random aneuploidizations. Refs.5,13,14,25,38-40,64 5 Cancer-specific aneuploidies or aneusomies determine cancer-specific phenotypes. Refs.13,25,53,64 6 Cancer typically appears only at advanced age (age bias), because aneuploidy is not heritable,183 and because the de novo generation of cancer-specific aneuploidies via random aneuploidization is very slow. Refs.5,14,43-45; Key for Table 1(#8 and #13); Non-heritability of aneuploidy 7 Congenital chromosomal instability, such as Bloom’s syndrome, Fanconi anemia, or Premature centromere division, induces cancer at young age, because it accelerates spontaneous aneuploidization. Refs.184,185 8 Simultaneous aneuploidization of many cells by carcinogens, eg. by tobacco, may cause “field cancerization”. Refs.16,17,56,186 9 Tumorigenicity of aneuploid cells in culture is proportional to their degrees of aneuploidy. Refs.163,187 10 Transplantability of tumor cells is proportional to the degree of aneuploidy, because more aneuploidy generates more antigenic variation. Ref.7 11 Genetic instability coincides with aneuploidy. Refs.29,48,60 12 Genetic instability is proportional to the degree of aneuploidy. Refs.28,50,152 13 Phenotypes of cancer cells, such as drug-resistance and cell morphology, vary with karyotype variations. Refs.11-13,62,188 14 Human cancer cells may become resistant to human viruses and susceptible to non-human viruses via karyotype variations. Refs.9,10 15 Clonal mutations in cancers derive from pre-neoplastic aneuploidy and non-clonal mutations from neoplastic aneuploidy. Ref.50; See Table 1 16 “Immortality” of aneuploid cells derives from variants that evade lethal mutations or toxins by reassorting chromosomes. Refs.6,11,12,189 17 Transient suppression of tumorigenicity via fusion of cancer cells with normal cells by unbalancing cancer-specific chromosome assortments. Tumorigenicity re-emerges via loss of chromosomes (Fig. 1). Refs.6,119,190; See text 18 Abnormal expression of hundreds or thousands of normal but aneuploid genes – the “sine qua non of malignant transformation”.4 Refs.114-116 are clonal,1,3,4,14,15 and (b) that their karyotypes are heterogeneous —a “confusing plethora”155—and thus non-clonal.1,13,24,62,63,119,156 Since these facts were incompatible with the expectation, that a specific aneuploidy would cause a specific cancer, it was concluded that aneuploidy must be a consequence, rather than a cause of cancer.13,25,62,79,119,131,157,158 2) Aneuploidy unknown as source of neoplastic phenotypes. Aneuploidy is also disregarded as a cause of cancer, because phenotype alteration by aneuploidy is simply unknown in cancer research. By contrast, phenotype alteration by gene mutation is canonical knowledge. For example, Foulds writes in Neoplastic Development in 1975, “The interpretations of the observations [of aneuploidy] on dysplasia and carcinoma in situ and on progression in these lesions …are still controversial.”1 Cairns writes in 1981 in Nature, “the observed changes in karyotype could … be trivial secondary events that occur after the rate limiting steps of carcinogenesis have been completed.”131 Cancer Biology, by Ruddon, says about “aneuploidy” in 1987, “Although the more subtle changes in the genome—namely point mutations, gene deletions, and gene rearrangements—may be associated with initiation of the malignant transformation process, gross changes in the number of chromosomes usually occur as tumors 206 progress to malignancy.”13 Mitelman et al. state in 1997, “the pathogenic significance of such abnormalities [aneuploidy] is totally unknown.”158 Orr-Weaver and Weinberg point out in 1998 “Aneuploidy has long been speculated to be causally involved in tumorigenesis, but its importance has not been demonstrated.”159 An editorial in Science comments in 1999 that it is “still unresolved…whether an increase in ploidy contributes to, or is a consequence of, tumor development.”148 Zimonjic et al. deplore in 2001 that aneuploidy, “confounds attempts to determine the precise cohort of genetic changes that are required for the transformation of normal human cells to a tumorigenic state...”.160 In line with this disregard for aneuploidy, the identification of suspected cancer genes and the analysis of the multiple steps of carcinogenesis are now routinely conducted in highly aneuploid cell lines, above all the mouse 3T3 and C3H 10T1/2 lines, which are assumed to be not tumorigenic because they resemble normal diploid fibroblasts morphologically.2,82,84,161 However, the relevance of results obtained with aneuploid cell lines to carcinogenesis must be called into question, because most, if not all of them are tumorigenic irrespective of their morphology.162,163 Indeed, the 3T3 and C3H cells are already sarcomagenic prior to morphological Cell Cycle 2003; Vol. 2 Issue 3 MULTISTEP CARCINOGENESIS transformation with hypothetical cancer genes or with carcinogens.164 Moreover, complete chromosome balances of multiple cells of human cancers, which are necessary to distinguish specific from unspecific aneuploidy, are not even reported in the recent literature, based on our experience. As a result of this bias, modern textbooks of biology do not even mention aneuploidy in the context of carcinogenesis.84,85,170 3) Aneuploidy said to be not necessary for cancer. The existence of presumably diploid cancers is cited as an argument that aneuploidy is not necessary for cancer. However, each of these cases fails to provide adequate documentation either for diploidy or for malignancy of the respective tumors.8,33,76,79,80,165,166 For example, Zimonjic et al. state in 2001 that, “a limited set of genes suffices to induce human cell transformation…[and] that widespread genomic changes involving large arrays of cellular genes [alias aneuploidy] are not required …”.160 But not even one in over 46 of their reportedly diploid, human tumor cells proved to be diploid in a subsequent cytogenetic analysis conducted by us.77 Further, Loeb et al. exclude aneuploidy as a cause of cancer—“it is neither a clonal marker nor an initial event”— based on the normal karyotype of “a premalignant condition”.91 4) Aneuploidy said to be not sufficient for cancer. Since some hybrids of normal and cancer cells are not tumorigenic, it has been argued that, unless certain normal genes are mutated, aneuploidy is not sufficient for carcinogenesis.2,4,119 However, all non-tumorigenic hybrids readily revert to tumorigenicity by spontaneous loss of chromosomes (see below and Fig. 1).2,4,119 This argument also ignores that the vast majority of such hybrids, including all the mouse lymphocyte- myeloma hybrids or hybridomas, are immortal and tumorigenic a priori.2,6,84,167 5) Aneuploidy interpreted as support for the gene mutation hypothesis. Recently aneuploidy has been reconsidered as a cause of cancer, if only as a mechanism to alter the dosage of hypothetical cancer genes or to generate new ones by mutation. For example, Lengauer et al. proposed in 1997 that aneuploidy may “select for gains of chromosomes containing activated oncogenes and for losses of chromosomes containing tumour-suppressor genes”,29 and, in a subsequent study, that it can “accelerate the acquisition of growth promoting mutations”,48 possibly by rearranging genes at breakpoints of rearranged chromosomes.30,158 In 2002, Weinberg et al. also proposed “that aneuploidy facilitates the acquisition of the genetic alterations that lead to cancer.”168 A recent review in Nature simply reduces Boveri’s chromosomal theory to the current oncogene theory of cancer, “if we substitute the word ‘gene’ for ‘chromosome’, this vision clearly predicted the Nobel Prize-winning discovery of cellular protooncogenes by Harold Varmus and Mike Bishop in the 1970s…”.169 Thus, for all those who have recently been looking for alternative causes of cancer, aneuploidy proved to be, at best, a diamond in the rough.33,79,80 3. A Unifying Hypothesis—Multistep Carcinogenesis via a Chain Reaction of Aneuploidizations. Intrigued by the enormous mutagenic potential of aneuploidy, its ubiquity in cancer and its proportionality with the degree of malignancy, we took up the challenge to develop an aneuploidy hypothesis, that: 1. would explain the origin of aneuploidy in cancer; 2. the spontaneous but characteristically slow evolution of an initiated cell to a cancer cell; and 3. how non-clonal and unstable karyotypes cause cancer. We think the model, that carcinogenesis results from a chain reaction of aneuploidizations, meets this challenge (see Fig. 1). According to our model the various phenotypes of cancer are www.landesbioscience.com consequences of cancer-specific aneuploidies, which alter the dosages of thousands of normal genes.64 These cancer-specific aneuploidies are products of a stepwise karyotype evolution that is initiated by a random aneuploidy. The initiating aneuploidy is caused either by a physical or chemical carcinogen, or is spontaneous.6 Since aneuploidy unbalances, via the corresponding genes, numerous, long-established teams of synergistic mitosis-proteins, and even the numbers of centrosomes,171-174 it renders chromosome segregation error-prone.6,152,175 Thus aneuploidy generates ever-new karyotypes autocatalytically— like a chemical chain-reaction. Additional carcinogens and tumor promoters2 can accelerate this evolution hetero-catalytically.176,177,192 Most of the randomly generated chromosome assortments would be lethal or less viable than normal ones, but some would be able to out-compete normal cells in the permissive habitat of the body and would thus be able to cause cancer. Since most random changes of chromosomes are unlikely to generate chromosome assortments that out-perform normal ones, the appearance of a cancer-specific aneuploidy is a rare and most probably a multistep event—analogous to the evolution of a new species. Indeed, carcinogenesis and phylogenesis both depend on alterations of chromosome numbers and structures. This is the reason, why it typically takes a long time to develop cancer. The end-product of this multistep evolution would be a maximally aneuploid or near-triploid, and thus also a maximally unstable and hence adaptable karyotype,152 which is the karyotype of the most malignant cancer cells.6,62,67,178 The inherent instability of highly aneuploid karyotypes explains the notorious heterogeneity or non-clonality of the karyotypes of clonal cancers as superpositions of selectively advantageous, cancerspecific and selectively neutral, random chromosome assortments. Thus cancer is clonal for aneuploidy and for various specific aneusomies, but not for a unique karyotype.64 Since aneuploidy also unbalances the many teams of DNA synthesis- and DNA maintenance-genes,84,179 and the genes that maintain nucleotide pools,180 aneuploidy also destabilizes the structure of the chromosomes and genes of cancer cells50—a state that is collectively called “genetic instability”.3,33 According to our model many gene mutations of cancer cells would then be consequences of aneuploidy. Thus, our model predicts that malignancy, karyotypic and genetic instability are all proportional to the degrees of aneuploidy, which is consistent with the literature50 (see Table 1, Table 2 and Fig. 1). Our model also predicts that aneuploid chromosome assortments—but not rearrangments— are reversible. In support of this, some cancer-specific phenotypes such as drug-resistance can get lost at the same rates at which they are generated,11,12 and malignancy of non-tumorigenic cancer-normal-cell hybrids is recovered by loss of chromosomes (Fig. 1).62,119 Our model is not only relevant to the origin of cancer from normal cells but also from hyperplasias with balanced karyotypes that carry a higher than normal risk of aneuploidization, as for example Barrett’s esophagus61 or the chronic phase of myeloid leukemia with the Philadelphia chromosome.4,6 However, our model is not relevant to the origin of diploid hyperplasia. For example, UVlight causes benign,hyperplastic papillomas in a small fraction of the mice in which it causes carcinomas—compatible with an aneuploidyindepdent mechanism.192 Our model of carcinogenesis confirms and extends the one proposed by Nowell in 1976.3 Like Nowell, we propose that the steps of progression of an initiated cell are aneuploidizations, although Nowell left open whether aneuploidy or gene mutation were causing cancer, “the genetic-versus-epigenetic debate”. But in contrast to Cell Cycle 207 MULTISTEP CARCINOGENESIS Nowell’s model, which holds that “It is certainly clear that visible alterations in chromosome structure are not essential to the initial change”, our model proposes that initiation is a random aneuploidy induced by a carcinogen, along the lines of Boveri’s hypothesis. Most importantly our hypothesis explains the origin of “genetic instability” by autocatalytic karyotype variation of aneuploid cells. As observed by Nowell, “this important characteristic has not been satisfactorily explained.”3 To prove our model, we have tested 18 of its predictions either by conducting new experiments or by selecting predicted experimental results from the large literature on cancer. It is shown in Table 2, that the literature, including our own work, does indeed support all of these 18 predictions made by the aneuploidy-cancer hypothesis. Thus the hypothesis, that multistep carcinogenesis is a chain reaction of aneuploidizations, can explain and predict all facts of carcinogenesis, particularly those that are paradoxical in view of the gene mutation hypothesis (Table 1). RELEVANCE OF THE ANEUPLOIDY HYPOTHESIS FOR THE CONTROL OF CANCER The chromosome hypothesis promises several benefits for the control of cancer. For example, eliminating from food and drugs substances that cause aneuploidy could prevent cancer. Identifying pre-cancerous cells in biopsies based on aneuploidy could revolutionize cancer therapy by eliminating affected tissues before they turn malignant. Even the treatment of clinical cancer could possibly be improved based on the risks that particular chromosome combinations may present. In principle this is already being proposed now based on genome-wide transcription profiles derived from micro-arrays of thousands of cellular genes.114-116 Acknowledgments We thank Peter Nowell (University of Pennsylvania, Philadelphia) for a critical review of the manuscript, David Rasnick, Rainer Sachs, Hung-Hsi Wu (U.C. Berkeley), Alice Fabarius and Ruediger Hehlmann (Mannheim, Germany) for information and discussions, and Mikhail Blagosklonny for inviting this review. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 208 Foulds L. Neoplastic Development; Vol 2. New York: Academic Press, 1975. Pitot HC. Fundamentals of Oncology; 4th ed. New York: Marcel Dekker, Inc., 2002. Nowell PC. The clonal evolution of tumor cell populations. Science 1976; 194:23-8. Ruddon RW. Cancer Biology. New York: Oxford University Press, 1981. Bauer KH. Das Krebsproblem; 2d ed. Berlin: Springer Verlag, 1963. Duesberg P, Rasnick D. Aneuploidy, the somatic mutation that makes cancer a species of its own. Cell Motil Cytoskeleton 2000; 47:81-107. Hauschka TS, Levan A. Inverse Relationship Between Chromosome Ploidy and HostSpecificity of Sixteen Transplantable Tumors. Exp. Cell Res 1953; 4:457-67. Hauschka TS. The chromosomes in ontogeny and oncogeny. Cancer Res 1961; 21:957-81. Hauschka TS. Correlation of Chromosomal and Physiologic Changes in Tumors. J Cell Comp Physiol 1958; 52(Suppl.):197-233. Vogt M. A Genetic Change in a Tissue Culture Line of Neoplastic Cells. J Cell Comp Physiol 1958; 52(Suppl.):271-85. Duesberg P, Stindl R, Hehlmann R. Explaining the high mutation rates of cancer cells to drug and multidrug resistance by chromosome reassortments that are catalyzed by aneuploidy. Proc Natl Acad Sci USA 2000;97:14295-14300. Duesberg P, Stindl R, Hehlmann R. Origin of multidrug resistance in cells with and without multidrug resistance genes: Chromosome reassortments catalyzed by aneuploidy. Proc Natl Acad Sci USA 2001; 98:11283-8. Ruddon RW. Cancer Biology, 2nd ed. New York: Oxford University Press, 1987. Cairns J. Cancer: Science and Society. San Francisco: W. H. Freeman and Company, 1978. Fialkow PJ. Clonal origin of human tumors. Annu Rev Med 1979; 30:135-43. Heim S, Mandahl N, Mitelman F. Genetic convergence and divergence in tumor progression. Cancer Res 1988; 48:5911-6. Ai H, Barrera JE, Pan Z, Meyers AD, Varella-Garcia M. Identification of individuals at high risk for head and neck carcinogenesis using chromosome aneuploidy detected by fluorescence in situ hybridization. Mutat Res 1999; 439:223-32. Foulds L. Tumor progression: a review. Cancer Res 1954; 14:327-39. 19. Foulds L. Neoplastic Development; Vol 2. New York: Academic Press, 1969. 20. Ahlstroem U. Chromosomes of primary carcinomas induced by 7,12-dimethylbenz(a)anthracene in the rat. Hereditas 1974; 78:235-44. 21. Levan G, Levan A. Specific chromosome changes in malignancy: studies in rat sarcomas induced by two polycyclic hydrocarbons. Hereditas 1975; 79:161-98. 22. Bartholdi MF, Ray FA, Cram LS, Kraemer PM. Karyotype instability of Chinese hamster cells during in vivo tumor progression. Somatic Cell Mol Genetics 1987; 13:1-10. 23. Bloch-Shtacher N, Sachs L. Identification of a chromosome that controls malignancy in Chinese hamster cells. J Cell Physiol 1977; 93:205-12. 24. Heppner G, Miller FR. The cellular basis of tumor progression. Int Rev Cytol 1998; 177:1-56. 25. Heim S, Mitelman F. Cancer Cytogenetics; 2nd ed. New York: Wiley-Liss, 1995. 26. Danielsen HE, Brogger A, Reith A. Specific gain of chromosome 19 in preneoplastic mouse liver cells after diethylnitrosamine treatment. Carcinogenesis 12:1777-80. 27. Mitelman F, ed. ISCN (1995): An International system for human cytogenetic nomenclature. Basel: S. Karger, 1995. 28. Duesberg P, Rausch C, Rasnick D, Hehlmann R. Genetic instability of cancer cells is proportional to their degree of aneuploidy. Proc Natl Acad Sci USA 1998; 95:13692-7. 29. Lengauer C, Kinzler KW, Vogelstein B. Genetic instability in colorectal cancers. Nature 1997; 386:623-7. 30. Lengauer C. How do tumors make ends meet? Proc Natl Acad Sci USA 2001; 98:12331-3. 31. Strauss BS. The origin of point mutations in human tumor cells. Cancer Res 1992; 52:249-53. 32. Strauss BS. The stability of the genome and the genetic instability of tumors. Perspect Biol Med Winter 2000; 43:286-300. 33. Marx J. Debate surges over the origins of genomic defects in cancer. Science 2002; 297:544-6. 34. Berenblum I, Shubik P. An experimental study of the initiating stage of carcinogenesis, and a re-examination of the somatic cell mutation theory of cancer. Br J Cancer 1949; 3:109-18. 35. Li R, Yerganian G, Duesberg P, Kraemer A, Willer A, Rausch C, Hehlmann R. Aneuploidy correlated 100% with chemical transformation of Chinese hamster cells. Proc Natl Acad Sci USA 1997; 94:14506-11. 36. Bradley MO, Bhuyan B, Francis MC, Langenbach R, Peterson A, Huberman E. Mutagenesis by chemical agents in V79 chinese hamster cells: a review and analysis of the literature. A report of the Gene-Tox Program. Mutat Res 1981; 87:81-142. 37. Scribner JD, Suess R. Tumor initiation and promotion. Int Rev Exp Pathol 1978; 18:137-87. 38. Boice JD, Jr., Monson RR. Breast cancer in women after repeated fluoroscopic examinations of the chest. J Natl Cancer Inst 1977; 59:823-32. 39. Doi M, Yukutake M, Tamura K, Watanabe K, Kondo K, Isobe T, Awaya T, Shigenobu T, Oda Y, Yanmakido K, Koyama K, Kohno N. A retrospective cohort study on respiratory tract cancers in the workers of the Japanese army poison-gas-factory operated from 1929 to 1945. Paper presented at: 38 th Annual Meeting of the American Society of Clinical Oncology; May 18-21, 2002; Orlando, FL. 40. Vogelstein B, Kinzler KW. The multistep nature of cancer. Trends Genet 1993; 9:138-41. 41. Walen KH, Stampfer MR. Chromosome analyses of human mammary epithelial cells at stages of chemical-induced transformation progression to immortality. Cancer Genet Cytogenet 1989; 37:249-61. 42. Fusenig NE, Boukamp P. Multiple stages and genetic alterations in immortalization, malignant transformation, and tumor progression of human skin keratinocytes. Mol Carcinog 1998; 23:144-58. 43. Nordling CO. A new theory on the cancer-inducing mechanism. Br J Cancer 1953; 7:68-72. 44. Armitage P, Doll R. The Age Distribution of Cancer and a Multi-Stage Theory of Carcinogenesis. Br J Cancer 1954; 8:1-12. 45. Renan MJ. How many mutations are required for tumorigenesis? Implications from human cancer data. Mol Carcinog 1993; 7:139-46. 46. Friehl JP. Dorland's Illustrated Medical Dictionary. 26th ed. Philadelphia: W.B. Saunders Co., 1985. 47. Frankfurt OS, Chin JL, Englander LS, Greco WR, Pontes JE, Rustum YM. Relationship between DNA ploidy, glandular differentiation, and tumor spread in human prostate cancer. Cancer Res 1985; 45:1418-23. 48. Shih IM, Zhou W, Goodman SN, Lengauer C, Kinzler KW, Vogelstein B. Evidence that genetic instability occurs at an early stage of colorectal tumorigenesis. Cancer Res 2001; 61:818-22. 49. Duesberg P, Li R, Rasnick D, Rausch C, Willer A, Kraemer A, Yerganian G, Hehlmann R. Aneuploidy precedes and segregates with chemical carcinogenesis. Cancer Genet Cytogenet 2000; 119:83-93. 50. Fabarius A, Hehlmann R, Duesberg P. Instability of chromosome structure in cancer cells increases exponentially with degrees of aneuploidy. Cancer Genet Cytogenet 2003:143:59-72. 51. Rachko D, Brand KG. Chromosomal aberrations in foreign body tumorigenesis of mice. Proc Soc Exp Biol Med 1983; 172:382-388. 52. Vanderlaan M, Steele V, Nettesheim P. Increased DNA content as an early marker of transformation in carcinogen-exposed rat tracheal cell cultures. Carcinogenesis 1983; 4:721-7. 53. Ried T, Heselmeyer-Haddad K, Blegen H, Schrock E, Auer G. Genomic changes defining the genesis, progression, and malignancy potential in solid human tumors: a phenotype/genotype correlation. Genes Chromosomes Cancer 1999; 25:195-204. 54. Nasiell M, Kato H, Auer G, Zetterberg A, Roger V, Karlen L. Cytomorphological grading and Feulgen DNA-analysis of metaplastic and neoplastic bronchial cells. Cancer 1978; 41:1511-21. 55. Jin Y, Jin C, Salemark L, Wennerberg J, Persson B, Jonsson N. Clonal chromosome abnormalities in premalignant lesions of the skin. Cancer Genet Cytogenet 2002; 136:48-52. 56. Sudbo J, Kildal W, Risberg B, Koppang HS, Danielsen HE, Reith A. DNA content as a prognostic marker in patients with oral leukoplakia. N Engl J Med 2001; 344:1270-8. Cell Cycle 2003; Vol. 2 Issue 3 MULTISTEP CARCINOGENESIS 57. Atkin NB, Baker MC. Possible differences between the karyotypes of preinvasive lesions and malignant tumours. Brit J Cancer 1969; 23:329-36. 58. Spriggs AI. Cytogenetics of cancer and precancerous states of the cervix uteri. In: German J, ed. Chromosomes and cancer. New York: John Wiley, 1974:423. 59. Rubin CE, Haggitt RC, Burmer GC, Brentnall TA, Stevens AC, Levine DS, Dean PJ, Kimmey M, Perera DR, Rabinovitch PS. DNA aneuploidy in colonic biopsies predicts future development of dysplasia in ulcerative colitis. Gastroenterology 1992; 103:1611-20. 60. Willenbucher RF, Aust DE, Chang CG, Zelman SJ, Ferrell LD, Moore DH, 2nd, Waldman FM. Genomic instability is an early event during the progression pathway of ulcerative-colitis-related neoplasia. Am J Pathol 1999; 154:1825-30. 61. Reid BJ, Blount PL, Rubin CE, Levine DS, Haggitt RC, Rabinovitch PS. Flow-cytometric and histological progression to malignancy in Barrett's esophagus: prospective endoscopic surveillance of a cohort. Gastroenterology 1992; 102(4 Pt 1):1212-9. 62. Koller PC. The Role of Chromosomes in Cancer Biology. New York: SpringerVerlag,1972. 63. Sandberg AA, Kakati S. Chromosome alterations and oncogenes in human neoplasia. In: Sharma T, ed. Trends in chromosome research: Springer-Verlag, 1990:190-203. 64. Fabarius A, Willer A, Yerganian G, Hehlmann R, Duesberg P. Specific aneusomies in Chinese hamster cells at different stages of neoplastic transformation, initiated by nitrosomethylurea. Proc Natl Acad Sci USA 2002; 99:6778-83. 65. Bocking A, Chatelain R. Diagnostic and prognostic value of DNA cytometry in gynecologic cytology. Anal Quant Cytol Histol 1989; 11:177-86. 66. Pilch H, Gunzel S, Schaffer U, Tanner B, Heine M. Evaluation of DNA ploidy and degree of DNA abnormality in benign and malignant melanocytic lesions of the skin using video imaging. Cancer 2000; 88:1370-7. 67. Sandberg AA. The chromosomes in human cancer and leukemia. Second ed. New York: Elsevier Science Publishing; 1990. 68. Atkin NB, Baker MC. Chromosome abnormalities as primary events in human malignant disease: evidence from marker chromosomes. J Natl Cancer Inst. 1966; 36:539-57. 69. Atkin NB. Chromosomes in human malignant tumors: A review and assessment. In: German J, ed. Chromosomes and cancer. New York: John Wiley & Sons, 1974:375-422. 70. Shackney SE, Berg G, Simon SR, Cohen J, Amina S, Pommersheim W, Yakulis R, Wang S, Uhl M, Smith CA, et al. Origins and clinical implications of aneuploidy in early bladder cancer. Cytometry 1995; 22:307-16. 71. Giaretti W. A model of DNA aneuploidization and evolution in colorectal cancer. Lab Invest 1994; 71:904-10. 72. Russo A, Bazan V, Migliavacca M, Tubiolo C, Macaluso M, Zanna I, Corsale S, Latteri F, Valerio MR, Pantuso G, Morello V, Dardanoni G, Latteri MA, Colucci G, Tomasino RM, Gebbia N. DNA aneuploidy and high proliferative activity but not K-ras-2 mutations as independent predictors of clinical outcome in operable gastric carcinoma: results of a 5year Gruppo Oncologico dell'Italia Meridonale (GDIM) prospective study. Cancer 2001; 92:294-302. 73. Flagiello D, Gerbault-Seureau M, Padoy E, Dutrillaux B. Near Haploidy in Breast Cancer: A Particular Pathway of Chromosome Evolution. Cancer Genet Cytogenet 1998; 102:54-8. 74. Magennis DP. Nuclear DNA in histological and cytological specimens: measurement and prognostic significance. Br J Biomed Sci 1997; 54:140-8. 75. Amiel A, Ohali A, Fejgin M, Sardos-Albertini F, Bouaron N, Cohen IJ, Yaniv I, Zaizov R, Avigad S. Molecular cytogenetic parameters in Ewing sarcoma. Cancer Genet Cytogenet 2003; 140:107-12. 76. Li R, Sonik A, Stindl R, Rasnick D, Duesberg P. Aneuploidy versus gene mutation hypothesis of cancer: recent study claims mutation, but is found to support aneuploidy. Proc Natl Acad Sci USA 2000; 97:3236-41. 77. Li R, Rasnick D, Duesberg P. Correspondence re: D. Zimonjic et al., Derivation of human tumor cells in vitro without widespread genomic instability. Cancer Res 2001; 61: 883844; Cancer Res 2002; 62:6345-8; discussion 6348-9. 78. Duesberg P. Are cancers dependent on oncogenes or aneuploidy? Cancer Genet Cytogenet 2003; 143:89-91. 79. Webb T. When theories collide: Experts develop different models for carcinogenesis. J Natl Cancer Inst 2001; 93:92-4. 80. Gibbs WW. Dissident or Don Quixote? Challenging the HIV theory got virologist Peter H. Duesberg all but excommunicated from scientific orthodoxy. Now he claims that science has got cancer all wrong. Sci Am 2001; 285:30-2. 81. Bishop JM. Enemies within: genesis of retrovirus oncogenes. Cell. 1981;23:5-6. 82. Tabin CJ, Bradley SM, Bargmann CI, Weinberg RA, Papageorge AG, Scolnick EM, Dhar R, Lowy DR, Chang EH. Mechanism of activation of a human oncogene. Nature 1982; 300:143-9. 83. Kinzler K, Vogelstein B. Lessons from hereditary cancer. Cell 1996; 87:159-70. 84. Lewin B. Genes VI. Oxford: Oxford University Press; 1997. 85. Lodish H, Berk A, Zipursky SL, Matsudaira P, Baltimore D, Darnell J. Molecular Cell Biology; 4th ed. New York : W. H. Freeman & Co., 1999. 86. Weinstein IB. Addiction to oncogenes--the Achilles heal of cancer. Science 2002; 297:63-4. 87. Vogel F, Motulsky AG. Human genetics: problems and approaches. New York: Springer Verlag, 1986. 88. Loeb LA. Mutator phenotype may be required for multistage carcinogenesis. Cancer Res 1991; 51:3075-9. 89. Duesberg PH, Schwartz JR. Latent viruses and mutated oncogenes: no evidence for pathogenicity. Prog Nucleic Acid Res Mol Biol. 1992;43:135-204. 90. Cahill DP, Kinzler KW, Vogelstein B, Lengauer C. Genetic instability and darwinian selection in tumours. Trends in Biological Sciences (TIBS). 1999; 24:M57-M60. 91. Loeb LA, Loeb KR, Anderson JP. Multiple mutations and cancer. Proc Natl Acad Sci USA 2003; 100:776-81. www.landesbioscience.com 92. Breslow RE, Goldsby RA. Isolation and characterization of thymidine transport mutants of Chinese hamster cells. Exptl Cell Res 1969; 55:339-46. 93. Hahn WC, Weinberg RA. Rules for making human tumor cells. N Engl J Med 2002; 347:1593-603. 94. Oshimura M, Barrett JC. Chemically induced aneuploidy in mammalian cells: mechanisms and biological significance in cancer. Environ Mutagen 1986; 8:129-59. 95. Lijinsky W. A view of the Relation Between Carcinogenesis and Mutagenesis. Env Mol Mutagenesis 1989; 14(Suppl.16):78-84. 96. Ashby J. Reflections on the declining ability of the salmonella assay to detect rodent carcinogens as positive. In: Langenbach R, et al., eds. Tumor Promotors: Biological Approaches for Mechanistic Studies and Assay Systems. New York: Raven Press, 1988:417-30. 97. Haber DA, Fearon ER. The promise of cancer genetics. Lancet 1998; 351:SII 1- 8. 98. Cowell J. Molecular Genetics of cancer. San Diego: Academic Press/Bios Scientific Publishers, 2001. 99. McCormick F. The polymerase chain reaction and cancer diagnosis. Cancer Cells 1989;1:56-61. 100. Vogelstein B, Fearon ER, Stanley BA, Hamilton R, Kern SE, Preisinger AC, Leppert M, Nakamura Y, White R, Smits AMM, Bos JL. Genetic alterations during colorectal-tumor development. N Engl J Med 1988; 319:525-32. 101. Hanahan D, Weinberg RA. The hallmarks of cancer. Cell 2000; 100:57-70. 102. Giaretti W, Monaco R, Pujic N, Rapallo A, Nigro S, Geido E. Intratumor heterogeneity of K-ras2 mutations in colorectal adenocarcinomas: association with degree of DNA aneuploidy. Am J Pathol 1996;149:237-45. 103. Baisse B, Bouzourene H, Saraga EP, Bosman FT, Benhattar J. Intratumor genetic heterogeneity in advanced human colorectal adenocarcinoma. Int J Cancer 2001; 93:346-52. 104. Konishi N, Hiasa Y, Matsuda H, Tao M, Tsuzuki T, Hayashi I, Kitahori Y, Shiraishi T, Yatani R, Shimazaki J, Lin IC. Intratumor cellular heterogeneity and alterations in ras oncogene and p53 tumor suppressor gene in human prostate carcinoma. Am J Pathol 1995; 147:1112-22. 105. Jenkins RB, Qian J, Lieber MM, Bostwick DG. Detection of c-myc oncogene amplification and chromosomal anomalies in metastatic prostatic carcinoma by fluorescence in situ hybridization. Cancer Res 1997; 57:524-31. 106. Albino AP, Le Strange R, Oliff AI, Furth ME, Old LJ. Transforming ras genes from human melanoma: a manifestation of tumor heterogeneity? Nature 1984; 308:69-72. 107. van Elsas A, Zerp S, van der Flier S, Kruse-Wolters M, Vacca A, Ruiter DJ, Schrier P. Analysis of N-ras mutations in human cutaneous melanoma: tumor heterogeneity detected by polymerase chain reaction/single-stranded conformation polymorphism analysis. Recent Results Cancer Res 1995; 139:57-67. 108. Walch A, Bink K, Gais P, Stangl S, Hutzler P, Aubele M, Mueller J, Hofler H, Werner M. Evaluation of c-erbB-2 overexpression and Her-2/neu gene copy number heterogeneity in Barrett's adenocarcinoma. Anal Cell Pathol 2000; 20:25-32. 109. Sauter G, Moch H, Moore D, Carroll P, Kerschmann R, Chew K, Mihatsch MJ, Gudat F, Waldman F. Heterogeneity of erbB-2 gene amplification in bladder cancer. Cancer Res 1993; 53(Suppl.10):2199-203. 110. Strommer K, Hamou MF, Diggelmann H, de Tribolet N. Cellular and tumoural heterogeneity of EGFR gene amplification in human malignant gliomas. Acta Neurochir (Wien). 1990; 107:82-7. 111. Park SH, Maeda T, Mohapatra G, Waldman FM, Davis RL, Feuerstein BG. Heterogeneity, polyploidy, aneusomy, and 9p deletion in human glioblastoma multiforme. Cancer Genet Cytogenet 1995; 83:127-35. 112. Szollosi J, Balazs M, Feuerstein BG, Benz CC, Waldman FM. ERBB-2 (HER2/neu) gene copy number, p185HER-2 overexpression, and intratumor heterogeneity in human breast cancer. Cancer Res 1995; 55:5400-7. 113. Shen CY, Yu JC, Lo YL, Kuo CH, Yue CT, Jou YS, Huang CS, Lung JC, Wu CW. Genome-wide search for loss of heterozygosity using laser capture microdissected tissue of breast carcinoma: an implication for mutator phenotype and breast cancer pathogenesis. Cancer Res 2000; 60:3884-92. 114. Zhang L, Zhou W, Velculescu VE, Kern SE, Hruban RH, Hamilton SR, Vogelstein B, Kinzler KW. Gene expression profiles in normal and cancer cells. Science 1997; 276:126872. 115. Pollack JR, Sorlie T, Perou CM, Rees CA, Jeffrey SS, Lonning PE, Tibshirani R, Botstein D, Borresen-Dale AL, Brown PO. Microarray analysis reveals a major direct role of DNA copy number alteration in the transcriptional program of human breast tumors. Proc Natl Acad Sci USA 2002; 99:12963-8. 116. van 't Veer LJ, Dai H, van de Vijver MJ, He YD, Hart AA, Mao M, Peterse HL, van der Kooy K, Marton MJ, Witteveen AT, Schreiber GJ, Kerkhoven RM, Roberts C, Linsley PS, Bernards R, Friend SH. Gene expression profiling predicts clinical outcome of breast cancer. Nature 2002; 415:530-6. 117. Kim SH, Roth KA, Moser AR, Gordon JI. Transgenic mouse models that explore the multistep hypothesis of intestinal neoplasia. J Cell Biol 1993; 123:877-93. 118. Donehower LA, Harvey M, Siagle BL, McArthur MJ, Montgomery CA, Jr., Butel JS, Bradley A. Mice deficient for p53 are developmentally normal but susceptible to spontaneous tumors. Nature 1992; 356:215-21. 119. Harris H. The cells of the body; a history of somatic cell genetics. Plainview, NY: Cold Spring Harbor Lab Press, 1995. 120. Purdie CA, Harrison DJ, Peter A, Dobbie L, White S, Howie SE, Salter DM, Bird CC, Wyllie AH, Hooper ML, et al. Tumour incidence, spectrum and ploidy in mice with a large deletion in the p53 gene. Oncogene 1994; 9:603-9. 121. Thomas H, Hanby AM, Smith RA, Hagger P, Patel K, Raikundalia B, Camplejohn RS, Balkwill FR. An inbred colony of oncogene transgenic mice: diversity of tumours and potential as a therapeutic model. Br J Cancer 1996; 73:65-72. Cell Cycle 209 MULTISTEP CARCINOGENESIS 122. Li B, Rosen JM, McMenamin-Balano J, Muller WJ, Perkins AS. neu/ERBB2 cooperates with p53-172H during mammary tumorigenesis in transgenic mice. Mol Cell Biol 1997; 17:3155-63. 123. Hahn WC, Counter CM, Lundberg AS, Beijersbergen RL, Brooks MW, Weinberg RA. Creation of human tumour cells with defined genetic elements. Nature (London) 1999; 400:464-8. 124. Harris CC. Chemical and physical carcinogenesis: Advances and perspective for the 1990s. Cancer Res 1991; 51:5023s-44s. 125. Barrett JC, Tsutsui T, Tsly T, Oshimura M. Role of genetic instability in carcinogenesis. In: Harris CC, Liotta LA, eds. Genetic Mechanisms in Carcinogenesis and Tumor Progression. New York: Wiley-Liss, 1990:97-114. 126. Jakubezak RJ, Merlino G, French JE, Muller WJ, Paul B, Adhya S, Garges S. Analysis of genetic instability during mammary tumor progression using a novel selection-based assay for in vivo mutations for a bacterial transgene target. Proc Natl Acad Sci USA 1996; 93:9073-8. 127. Wang TL, Rago C, Silliman N, Ptak J, Markowitz S, Willson JK, Parmigiani G, Kinzler KW, Vogelstein B, Velculescu VE. Prevalence of somatic alterations in the colorectal cancer cell genome. Proc Natl Acad Sci USA 2002; 99:3076-80. 128. Tomlinson I, Bodmer W. Selection, the mutation rate and cancer: insuring that the tale does not wag the dog. Nature Med 1999; 5:11-2. 129. Haigis KM, Caya JG, Reichelderfer M, Dove WF. Intestinal adenomas can develop with a stable karyotype and stable microsatellites. Proc Natl Acad Sci USA 2002; 99:8927-31. 130. Abdel-Rahman WM, Katsura K, Rens W, Gorman PA, Sheer D, Bicknell D, Bodmer WF, Arends MJ, Wyllie AH, Edwards PA. Spectral karyotyping suggests additional subsets of colorectal cancers characterized by pattern of chromosome rearrangement. Proc Natl Acad Sci USA 2001; 98:2538-43. 131. Cairns J. The origin of human cancers. Nature. 1981;289:353-357. 132. Stock RP, Bialy H. The sigmoidal curve of cancer. Nat Biotechnol 2003; 21:13-4. 133. Atkin NB, Baker MC. Are human cancers ever diploid–or often trisomic? Conflicting evidence from direct preparations and cultures. Cytogenet Cell Genet 1990; 53:58-60. 134. Grimwade D, Walker H, Harrison G, Oliver F, Chatters S, Harrison CJ, Wheatley K, Burnett AK, Goldstone AH. The predictive value of hierarchical cytogenetic classification in older adults with acute myeloid leukemia (AML): analysis of 1065 patients entered into the United Kingdom Medical Research Council AML11 trial. Blood 2001; 98:1312-20. 135. Grimwade D, Walker H, Oliver F, Wheatley K, Harrison C, Harrison G, Rees J, Hann I, Stevens R, Burnett A, Goldstone A. The importance of diagnostic cytogenetics on outcome in AML: analysis of 1,612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children's Leukaemia Working Parties. Blood 1998; 92:2322-33. 136. Duesberg P, Stindl R, Li R, Hehlmann R, Rasnick D. Aneuploidy versus gene mutation as cause of cancer. Current Science 2001; 81:490-500. 137. Winge O. Zytologische Untersuchungen ueber die Natur maligner Tumoren. II. Teerkarzinome bei Maeusen. Zeitschrift fuer Zellforschung und Mikroskopische Anatomie 1930; 10:683-735. 138. Boveri T. On multipolar mitosis as a means of analysis of the cell nucleus (originally published 1902). In: Willier BH, Oppenheimer JM, eds. Foundations of Experimental Embryology. Englewood Cliffs, NJ: Prentice-Hall, 1964:74-97. 139. Lindsley DL, Sandler L, Baker BS, Carpenter ATC, Denell RE, Hall JC, Jacobs PA, Gabor Miklos GL, Davis BK, Gethmann RC, Hardy RW, Hessler A, Miller SM, Nozawa H, Parry DM, Gould-Somero M. Segmental aneuploidy and the genetic gross structure of the Drosophila genome. Genetics 1972; 71:157-84. 140. Matzke MA, Mittelsten-Scheid O, Matzke AJM. Rapid structural and epigenetic changes in polyploid and aneuploid genomes. BioEssays 1999; 21:761-7. 141. Mayer VW, Aguilera A. High levels of chromosome instability in polyploids of Saccharomyces cerevisiae. Mutat Res 1990; 231:177-86. 142. Hughes TR, Roberts CJ, Dai H, Jones AR, Meyer MR, Slade D, Burchard J, Dow S, Ward TR, Kidd MJ, Friend SH, Marton MJ. Widespread aneuploidy revealed by DNA microarray expression profiling. Nat Genet 2000; 25:333-7. 143. Liu P, Zhang H, McLellan A, Vogel H, Bradley A. Embryonic lethality and tumorigenesis caused by segmental aneuploidy on mouse chromosome 11. Genetics 1998; 150:1155-68. 144. Lejeune J, Turpin R, Gautier M. Le Mongolisme, premier exemple d'abberation autosomique humaine. Ann Genet 1959; 2:41-9. 145. Reeves RH. Recounting a genetic story. Nature 2000; 405:283-4. 146. Epstein C. The Consequences of Chromosome Imbalance: Principles, Mechanisms, and Models. New York: Cambridge University Press, 1986. 147. Kurnit DM. Down syndrome; gene dosage at the transcriptional level in skin fibroblasts. Proc Natl Acad Sci USA 1979; 76:2372-5. 148. Hieter P, Griffiths T. Polyploidy – more is more or less. Science 1999; 285:210-1. 149. Cornish-Bowden A. Kinetics of multi-enzyme systems. In: Rehm H-J, Reed G, eds. Biotechnology. Vol 9. New York: VCH, 1995:121-36. 150. Kacser H, Burns JA. Molecular democracy: who shares the controls? Biochem Soc Trans 1979; 7:1149-60. 151. Kacser H, Burns JA. The molecular basis of dominance. Genetics 1981; 97:639-66. 152. Rasnick D, Duesberg P. How aneuploidy affects metabolic control and causes cancer. Biochem J 1999; 340:621-30. 153. Hansemann D. Ueber asymmetrische Zelltheilung in Epithelkrebsen und deren biologische Bedeutung. Virchows Arch Pathol Anat 1890; 119:299-326. 154. Boveri T. Zur Frage der Entstehung maligner Tumoren. Jena, Germany: Gustav Fischer Verlag, 1914. 155. Heim S, Mitelman F. Cancer Cytogenetics. New York: Alan R. Liss, Inc., 1987. 156. Rous P. Surmise and fact on the nature of cancer. Nature 1959; 183:1357-61. 210 157. Johansson B, Mertens F, Mitelman F. Primary vs. secondary neoplasia-associated chromosomal abnormalities – balanced rearrangements vs. genomic imbalances? Genes Chromosom Cancer 1996; 16:155-63. 158. Mitelman F, Mertens F, Johansson B. A breakpoint map of recurrent chromosomal rearrangements in human neoplasia. Nature Genet 1997; Suppl.15:S417-74. 159. Orr-Weaver TL, Weinberg RA. A checkpoint on the road to cancer. Nature 1998; 392:223-4. 160. Zimonjic D, Brooks MW, Popescu N, Weinberg RA, Hahn WC. Derivation of human tumor cells in vitro without widespread genomic instability. Cancer Res 2001; 61:8838-44. 161. Kennedy AR, Cairns J, Little JB. Timing of the steps in transformation of C3H 10T1/2 cells by X-irradiation. Nature 1984; 307:85-6. 162. McAllister RM, Corriell LL. Tumorigenicity of tissue culture cells. Cancer Res 1959; 19:1040-4. 163. Gershwin ME, Lentz D, Owens RB. Relationship between karyotype of tissue culture lines and tumorigenicity in nude mice. Exp Cell Biol 1984; 52:361-70. 164. Boone CW, Jacobs JB. Sarcomas routinely produced from putatively nontumorigenic Balb/3T3 and C3H/10T1/2 cells by subcutaneous inoculation attached to plastic platelets. J Supramol Struct 1976; 5:131-7. 165. Bayreuther K. Chromosomes in Primary Neoplastic Growth. Nature 1960; 186:6-9. 166. Lippmann SM. Molecular Markers of the Risk of Oral Cancer. N Engl J Med 2001; 344:Editorial. 167. American Type Culture Collection. Catalogue of Cell Lines and Hybridomas; 7th ed. Rockville, MD: American Type Culture Collection, 1992. 168. Zimonjic D, Brooks MW, Popescu N, Weinberg RA, Hahn WC. Correspondence re: D. Zimonjic et al., Derivation of human tumor cells in vitro without widespread genomic instability. Cancer Res 2002; 62:6348-9. 169. Balmain A. Cancer genetics: from Boveri and Mendel to microarrays. Nat Reviews 2001; 1:77-82. 170. Alberts B, Bray D, Lewis J, Raff M, Roberts K, Watson JD. Molecular Biology of the Cell. New York: Garland Publishing, Inc.,1994. 171. Lingle WL, Lutz WH, Ingle JN, Maihle NJ, Salisbury JL. Centrosome hypertrophy in human breast tumors: implications for genomic stability and cell polarity. Proc Natl Acad Sci USA 1998; 95:2950-5. 172. Duesberg P. Are centrosomes or aneuploidy the key to cancer? Science 1999; 284:2091-2. 173. Pihan GA, Purohit A, Wallace J, Knecht H, Woda B, Quesenberry P, Doxsey SJ. Centrosome defects and genetic instability in malignant tumors. Cancer Res 1998; 58:3974-85. 174. Brinkley BR, Goepfert TM. Supernumerary centrosomes and cancer: Boveri's hypothesis resurrected. Cell Motil Cytoskeleton 1998; 41:281-8. 175. Holliday R. Chromosome error propagation and cancer. Trends Genet 1989; 5:42-5. 176. Parry JM, Parry EM, Barrett JC. Tumour promoters induce mitotic aneuploidy in yeast. Nature 1981; 294:263-5. 177. Iversen OH. The skin tumorigenic and carcinogenic effects of different doses, numbers of dose fractions and concentrations of 7,12-dimethylbenz[a]anthracene in acetone applied on hairless mouse epidermis. Possible implications for human carcinogenesis. Carcinogenesis 1991; 12:493-502. 178. Atkin NB. Nuclear Size in Premalignant Conditions of the Cervix Uteri. Nature 1964:201. 179. Wood RD, Mitchell M, Sgouros J, Lindahl T. Human DNA repair genes. Science 2001; 291:1284-9. 180. Das SK, Kunkel TA, Loeb LA. Effects of altered nucleotide concentrations on the fidelity of DNA replication. Basic Life Sci 1985; 31:117-26. 181. Pavarino EC, Antonio JR, Pozzeti EM, Larranaga HJ, Tajara EH. Cytogenetic study of neoplastic and nonneoplastic cells of the skin. Cancer Genet Cytogenet 1995; 85:16-9. 182. Bremner R, Balmain A. Genetic changes in skin tumor progression: correlation between presence of a mutant ras gene and loss of heterozygosity on mouse chromosome 7. Cell 1990; 61:407-17. 183. Hassold TJ. Chromosome abnormalities in human reproductive wastage. Trends in Genetics 1986; 2:105-10. 184. German J. Bloom's syndrome. II. The prototype of genetic disorders predisposing to chromosome instability and cancer. In: German J, ed. Chromosomes and Cancer. New York: John Wiley & Sons, 1974:601-17. 185. Plaja A, Perez C, Miro R. Chromosome aneuploidy and cancer: lessons from a chromosomal instability syndrome. Cancer Genet Cytogenet 2001; 131:144-5. 186. Jin C, Jin Y, Wennerberg J, Akervall J, Dictor M, Mertens F. Karyotypic heterogeneity and clonal evolution in squamous cell carcinomas of the head and neck. Cancer Genet Cytogenet 2002; 132:85-96. 187. Cram LS, Bartholdi MF, Ray FA, Travis GL, Kraemer PM. Spontaneous neoplastic evolution of Chinese hamster cells in culture: Multistep progression of karyotype. Cancer Res 1983; 43:4828-37. 188. Kraemer PM, Deaven LL, Crissman HA, Steinkamp HA, Petersen DF. On the Nature of Heteroploidy. Cold Spring Harbor Symposium 1973; 38:133-44. 189. Hayflick L. The limited in vitro lifetime of human diploid cell strains. Exp Cell Res 1965; 37:614-36. 190. Barski G, Cornefert F. Charactersitics of “hybrid”-type clonal cell lines obtained from mixed cultures in vitro. J Natl Cancer Inst 1962; 28:801-21. 191. Lander ES, Linton LM, Birren B, Nusbaum C, Zody MC, Baldwin J, et al. Initial sequencing and analysis of the human genome. Nature 2001; 409:860-921. 192. de Last A, van der lun JC, de Gruijl FR. Carcinogenesis induced by UVA (365-nm) radiation: the dose-time dependence of tumor formation in hairless mice. Carcinogenesis 1997; 18:1013-20. 193. Little JB. Radiation carcinogenesis Carcinogenesis 2000; 21:397-404. Cell Cycle 2003; Vol. 2 Issue 3