Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
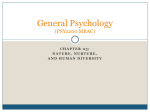
Human Genetics Laboratory 985440 Nebraska Medical Center Omaha, NE 68198-5440 Address Service Requested Over 40 Years of Dedicated Service and Personalized Care Newsletter for health care providers in this issue page 1 ACOG recommends Prenatal Microarray Recent recommendations have increased the use of microarray in the prenatal setting. page 4 FISH for Non-Small Cell Lung Carcinoma (NSCLC) Tiered FISH testing is recommended to detect abnormalities in ALK, ROS1, and RET. page 6 A new approach to comprehensive gene panel testing Next Generation Sequencing (NGS) combined with Deletion/Duplication Analysis allows detection of both sequenced-based variations and intragenic copy number changes. Human Genetics Laboratory Newsletter | Summer 2014 UNMC Human Genetics Laboratory for health care providers Prenatal Microarray O ur laboratory offers a wide range of prenatal genetic testing services, which include chromosome analysis (karyotyping), fluorescence in situ hybridization (FISH), and microarray analysis. Historically, chromosome analysis and FISH have been the predominant assays of choice for indications such as advanced maternal age; abnormal ultrasound findings; abnormal 1st, 2nd, or combined maternal serum screening result; and a family history of a genetic or chromosomal abnormality. These tests continue to provide practitioners and patients with valuable diagnostic information in the prenatal period. More recently, the use of microarray analysis in the prenatal setting has steadily increased, at least partly as a result of the joint opinion put forth by the American College of Obstetrics and Gynecology (ACOG) and the Society of Maternal Fetal Medicine. This opinion recommends the use of microarray analysis when fetal ultrasound anomalies are detected or when a patient is undergoing invasive prenatal diagnostic testing and emphasizes that this analysis should be made available to patients regardless of maternal age.1 In the prenatal setting, our laboratory uses a microarray platform designed specifically for the detection of submicroscopic deletions and duplications in regions of known clinical relevance. In addition, this platform offers whole genome coverage for accurate copy number assessment and includes single nucleotide polymorphisms (SNPs) for enhanced detection of maternal cell contamination. Results for this testing are typically available within 1-2 weeks of specimen receipt in the laboratory. Please contact us for additional information about the benefits of Prenatal Microarray for your patients. 1 The use of chromosomal microarray analysis in prenatal diagnosis. Committee Opinion No. 581. American College of Obstetricians and Gynecologists. Obstet Gynecol, 122:1374-1377, 2013. Genetic Counselors Essential to Laboratory Mission As part of our comprehensive services, the Human Genetics Laboratory team includes licensed and board-certified genetic counselors to assist providers and their patients. Our genetic counselors have current clinical experience as well as dedicated areas of expertise, ranging from prenatal and postnatal genetics to oncology. Serving as a liaison between providers and laboratory services, genetic counselors recommend indication-specific testing strategies, request additional clinical information for improved testing and interpretation, notify providers of STAT results, and discuss test results and pertinent management issues. Our counselors look forward to interacting with you. Human Genetics Laboratory Newsletter | Summer 2014 From the director Our laboratory continues to provide diagnostic genetic testing services to clinicians across a number of specialties, including pediatrics, obstetrics and gynecology, neurology, cardiology, genetic medicine, medical oncology, and pathology. In addition, clinical geneticists and genetic counselors continue to offer consultation in Omaha and across the state of Nebraska. Because genetic testing is constantly evolving, our team remains committed to provider outreach and education and has bolstered our ability to do so in a number of ways over the past year: • We now have a dedicated marketing specialist who serves as a resource for providers. • Our laboratory directors, genetic counselors, and marketing specialist routinely make personal visits to clinics and hospitals. • Our clinical genetics team has expanded their specialty clinics to include adult genetics, autism, complex craniofacial, hereditary cancer, metabolism, neurosensory, and prenatal development. • We have enhanced provider and patient educational materials, including prenatal and postnatal testing booklets, hereditary cancer testing and oncology flyers, and patient brochures. Newsletter | Summer 2014 This Newsletter is produced by the Human Genetics Laboratory, part of Munroe-Meyer Institute at the University of Nebraska Medical Center. For additional printed copies, or other information, please contact: Nicole (Nikki) Hackendahl Marketing Specialist 402-559-6935 [email protected] Human Genetics Laboratory 985440 Nebraska Medical Center Omaha, NE 68498-5440 [email protected] In addition, clinical and laboratory faculty and genetic counselors are always willing to provide formal educational lectures for your staff. Please contact our marketing specialist, Nicole Hackendahl (see left sidebar), if you would like more information about the educational materials available or if you would like to schedule a formal meeting with one of our faculty. Our dedicated and experienced technical staff is continually researching and developing new, clinically-relevant genetic testing in order to improve the diagnostic yield for your patients. We have expanded our test menu to include high resolution deletion/duplication analysis of clinically-relevant genes to complement our sequencing panels. Over the past year, we also developed and validated a hereditary breast cancer panel designed to detect abnormalities in six high-risk genes associated with breast cancer, and I am pleased to announce that we are expanding this service to other hereditary cancers (including colorectal, ovarian, uterine, endocrine, neuroendocrine, neurologic, pancreatic, and renal) early this fall. We have also validated additional oncology fluorescence in situ hybridization (FISH) probes for clinically relevant loci, such as IGK, IGL, ROS1, and RET. Please continue to check our website for the most up-to-date test offerings and continue to communicate your genetic testing needs to our laboratory team, as your requests serve as the basis for our future assay developments. Thank you for your ongoing loyalty and trust in our genetic services. We are honored to partner with you in service to patients and remain committed to doing so with unparalleled accuracy, efficiency, and compassion. www.unmc.edu/geneticslab Warren G. Sanger, Ph.D. Director, Human Genetics Laboratory Interim Director, Genetic Medicine Munroe-Meyer Institute University of Nebraska Medical Center Newsletter | 2 FACULTY HIGHLIGHTS R. Tanner Hagelstrom, PhD, MBA, FACMG Jennifer N. Sanmann, PhD, MB(ASCP)CMCGCM Dr. Tanner Hagelstrom is an Associate Director of the Human Genetics Laboratory at the Munroe-Meyer Institute. He is a Fellow of the American College of Medical Genetics and Genomics (ACMG) and is board certified in Clinical Cytogenetics and Clinical Molecular Genetics through the American Board of Medical Genetics and Genomics. Following completion of a two year clinical cytogenetics fellowship this June, Dr. Jennifer Sanmann joined the Human Genetics Laboratory as an Associate Director. She is board eligible in the subspecialty of Clinical Cytogenetics through the American Board of Medical Genetics and Genomics. Although her roles and responsibilities in the laboratory have changed over time, Dr. Sanmann has been a member of the Human Genetics Laboratory team since 2005. She completed both her doctoral and clinical postdoctoral training under the direction of Dr. Warren Sanger in 2012 and 2014, respectively. Dr. Hagelstrom received his PhD and MBA from Colorado State University in 2007 and 2010, respectively. Following a postdoctoral training at the Translational Genomics Research Institute in Scottsdale, Arizona, Dr. Hagelstrom completed his Clinical Cytogenetics and Molecular Genetics fellowships at the University of Colorado Anschutz Medical Center. Dr. Sanmann began her academic appointment at UNMC as an Assistant Professor of the Munroe-Meyer Institute on July 1. She currently serves as a board member for the Great Plains Chapter of the Clinical Laboratory Management Association. Dr. Sanmann’s research focuses on understanding the relationship between genotype and phenotype in both the constitutional and oncology settings using a variety of cytogenetic and molecular genetic techniques. Dr. Hagelstrom joined the laboratory in July 2013 and is currently an Assistant Professor of the Munroe-Meyer Institute at UNMC. He serves on the ACMG Program Committee, and his research interests focus primarily on identifying unique genetic changes that can be utilized for diagnostic purposes or treatment decisions in malignancies. Tips & Tools: Preauthorization of Genetic Testing Due to the rapid advancements in genetics, a growing number of practitioners are utilizing genetic testing for the diagnosis and medical management of their patients. Consequently, preauthorization for genetic testing has become increasingly prominent in clinics and hospitals across the country. In order to aid practitioners in this preauthorization process, our laboratory has developed specimen- and diagnosis-specific forms that query the information required for the determination of coverage and preauthorization. The following preauthorization forms are available on the Human Genetics Laboratory website: • prenatal • pregnancy loss • postnatal (peripheral blood) • hematology / oncology Upon request, our laboratory will obtain preauthorization for your patient’s genetic studies. Please contact our billing team with any questions or concerns related to this process. 402.559.5070 FIND US ONLINE www.unmc.edu/geneticslab Human Genetics Laboratory Newsletter | Summer 2014 Any FISH Necessary to Clarify Diagnosis, Clarified We recently modified our Oncology Test Request Form to simplify the ordering process for clinicians and their staff. There is an option on the form within Test Selection that, when checked, authorizes our laboratory to perform any FISH necessary to clarify the patient’s diagnosis. For ease, this option is now located directly below Chromosome Analysis. p Chromosome Analysis p Perform any FISH necessary to clarify diagnosis p FISH [specify]: FISH Analysis: NonLung cancer is the most common cancer worldwide and is the leading cause of cancer death in the United States.1-2 By selecting the “any FISH necessary to clarify diagnosis” option on the test request form, ordering providers eliminate any delay in testing that may occur while authorization is obtained and fulfill the laboratory’s regulatory requirement for written orders without disruption of your clinic or hospital for authorization. Our laboratory staff will only add adjunct FISH when indicated by diagnosis or when needed to clarify an abnormality observed by Chromosome Analysis (karyotyping). In addition, we will always provide a fax notification when tests are added to keep the ordering physician abreast of the pending studies. Please note that this option does not replace the specified FISH test selection, which should still be used in cases where the physician wants to order a specific FISH test at the time of specimen collection. A current list of all of our available hematology, lymphoma, and solid tumor FISH probes is available on our laboratory website. p Chromosome Analysis p Perform any FISH necessary to clarify diagnosis p FISH [specify]: CLL Panel ALK (2p23) Dual Color Breakapart Probe, positive for rearrangement in a polyploidy population Optimized microarray for subotimal specimens, including solid tissue tumors Our laboratory has recently obtained the OncoScanTM microarray platform, which has been designed to circumvent the obstacles typically encountered with these degraded specimens. The Human Genetics Laboratory has performed chromosomal microarray studies on a variety of sample types since the technology’s infancy. However, historical platforms have long been challenged to analyze DNA of suboptimal quality, such as that from formalin fixed paraffin-embedded (FFPE) tissues, which has restricted genomic analysis on certain specimens. This whole genome assay will detect genomic dosage anomalies (deletions and duplications) and copy-neutral loss of heterozygosity at a resolution of 50-100kb in approximately 900 cancerrelated genes and at a resolution of 300kb throughout the remaining genomic backbone. Thus, this platform is ideal for the identification of diagnosis-specific genetic profiles in solid tissue tumors. Currently, the platform is being utilized for research aimed at Newsletter | 4 -Small Cell Lung Carcinoma (NSCLC) Lung cancer is divided into two histologic subgroups: (1) non-small cell lung cancer (NSCLC), which accounts for more than 85% of cases and can be subdivided into non-squamous carcinoma (including adenocarcinoma, large cell carcinoma, other cell types) and squamous cell carcinoma and (2) small cell lung cancer, which accounts for the remaining ~15% of lung cancer cases.2 In recent years, the understanding and knowledge of the pathogenesis of NSCLC, particularly adenocarcinoma, has grown exponentially and has led to the discovery of novel acquired genetic abnormalities that allow for targeted therapies. Several biomarkers have been identified in NSCLC that help drive therapy and predict treatment efficacy. These predictive biomarkers include EGFR, HER2 (ERBB2), and BRAF mutations; ALK, ROS1, and RET rearrangements; and MET amplification.2 The NCCN Guidelines for NSCLC recommend EGFR mutation testing and ALK gene rearrangement analysis for patients with adenocarcinoma; large cell carcinoma; NSCLC not otherwise specified (NOS); or squamous cell carcinoma in never smokers, a small biopsy specimen, or a specimen with mixed histology.2 The NCCN guidelines recommend subsequent consideration should be given to the other genetic biomarker testing following EGFR and ALK as appropriate. To meet clinical testing needs, our laboratory offers assessment of the ALK, ROS1, and RET loci using fluorescence in situ hybridization (FISH). The FISH assay for each of these three loci is designed to detect rearrangement of the gene that, if present, is known to be susceptible to targeted therapies. The ALK, ROS1, and RET FISH testing is typically performed on 4-6 µm sections prepared from paraffin-embedded tumor tissue, and results are available within 3-5 days of specimen receipt. Please contact the laboratory for any questions regarding this testing. REFERENCES 1 World Health Organization. Cancer. Fact Sheet No 297. January 2013. 2 National Comprehensive Cancer Network (NCCN). Non-Small Cell Lung Cancer (Version 4.2014) Education and Outreach improving our understanding of the genetic hallmarks of various pediatric brain tumors. The Human Genetics Laboratory was represented at the national American College of Medical Genetics and Genomics (ACMG) meeting in Nashville in March. The meeting provided a great opportunity for several of our faculty and staff to learn about the latest advancements in the field and to reconnect with colleagues. Additionally, this platform is being validated for use in the clinical setting (FFPE or otherwise suboptimal specimens) and is projected to be available for order in the fall of 2014. In addition, the ACMG meeting afforded our team the opportunity to share our newest clinical test offerings with attendees and to present our latest research efforts in the postnatal realm, which included the following: If you would like more information about how this assay may assist with your research goals, or if you would like additional information as this assay transitions to a clinical test offering, please contact Dr. Sanmann for details. [email protected] • Clinical and Laboratory Collaboration: Team Approach to Next Generation Sequencing Variant Interpretation (D.L. Bishay, et al.) • Genetic Testing for Dilated Cardiomyopathy: Ethical Dilemmas Including PSEN1 and PSEN2 (A.C. Carter, et al.) • Hajdu-Cheney syndrome: patient with rare complex heart defect (L.J. Starr, et al.) • Psychiatric Disease is Common and Undertreated in Ehlers-Danlos Syndrome Hypermobile Type (E.T. Rush, et al.) • Utility of Fluorescence In Situ Hybridization (FISH) to Confirm Copy Number Changes Identified by Microarray (J.N. Sanmann, et al.) 2014 Human Genectics Laboratory ACMG booth. Abstracts above available upon request. Human Genetics Laboratory Newsletter | Summer 2014 A COMPREHENSIVE APPROACH TO GENE PANEL TESTING G enetic changes that result in disease come in several different forms, including sequence-based mutations (changes in the DNA at the basepair level) and intragenic deletions/duplications (copy number changes within the target gene). Regardless of the type of disease-causing change observed, these genetic aberrations often result in a similarly aberrant protein product. Current technology does not allow for both sequence-based variations and intragenic copy number changes to be detected reliably in a single assay. Thus, comprehensive analysis of genes for disease-causing aberrations typically requires a multi-assay approach. In order to ensure comprehensive analysis of clinically-relevant genes of interest, our laboratory recently added high resolution deletion/duplication analysis for all of the genes that we have traditionally sequenced using our next generation sequencing (NGS) technology. Therefore, we are able to evaluate a panel of indication-specific genes for both sequence-based mutations and small-scale deletions or duplications in a time- and costefficient manner. This combination of testing can be easily ordered on our test request form by selecting the “comprehensive testing” box for any of our panel tests. When comprehensive testing is selected, testing is performed in a tiered manner to eliminate unnecessary costs to the patient. The tiered approach for each indication-specific panel is outlined next to the comprehensive testing selection on the test request form for easy reference. Craniosynostosis Gene Panel The Human Genetics Laboratory offers a panel designed to detect aberrations in four genes known to be associated with craniosynostosis, the premature closure of one or more sutures in an individual’s skull. With an incidence of 1 in every 2,000-2,500 births, many craniosynostosis syndromes exist and often have additional clinical features, making a single panel for the evaluation of these various syndromes ideal for both the clinician and the patient.1 Additionally, aberrations in these genes can inhibit or alter bone growth; therefore, several skeletal dysplasias are also covered by this panel. SUSPECTED SYNDROMES: • Achondroplasia • Antley-Bixler syndrome COMPREHENSIVE TESTING EXAMPLE • Apert syndrome Connective Tissue Disorders Panel • Beare-Stevenson syndrome p Comprehensive testing [includes: seq, reflex to del/dup] p Sequencing only p Del/dup only Alternatively, individual tests, such as sequencing only or high resolution deletion/duplication analysis only, can be selected easily on the test request form, as indicated below. • CATSHL (tall stature, hearing loss) • Crouzon syndrome • Hypochondroplasia • Jackson-Weiss syndrome • Kallmann syndrome • LADD SINGLE TESTING EXAMPLE • Muenke syndrome Connective Tissue Disorders Panel • Pfeiffer syndrome p Comprehensive testing [includes: seq, reflex to del/dup] p Sequencing only Del/dup only p • Rhizomelic limb shortening • Radioulnar synostosis • Robinow-Sorauf syndrome • Saethre-Chotzen syndrome Please contact the laboratory if you have any questions about this new test offering or the updated postnatal test request form. Newsletter | 6 Connective Tissue Disorders Gene Panel Individuals with inherited connective tissue disorders frequently harbor an aberration in a gene involved in the structure or function of connective tissue. Such disorders typically include medical issues with the joints, eyes, skin, and cardiovascular system, though other body systems are commonly affected. Often, genetic testing is useful for the establishment of an appropriate diagnosis and medical management plan for an affected individual or family. To aid in the diagnosis of patients with connective tissue disorders, the Human Genetics Laboratory launched an indication-specific gene panel in the fall of 2013. CLINICAL INDICATIONS FOR TESTING: Craniosynostosis Facial features such as proptosis (bulging eyes), ptosis, widely spaced eyes, flattened midface, temporal bossing Syndactyly, clinodactyly, broad toes, broad thumbs Short stature or shortened long bones Palatal abnormalities (cleft or high palate) Bone fusions, especially carpal, tarsal, and radioulnar synostosis Developmental delay, hearing loss, or vision concerns in a person suspected to have craniosynostosis or skeletal dysplasia GENES COVERED2: FGFR1 5% Pfeiffer syndrome type 1 100% Apert syndrome <100% Beare-Stevenson syndrome 100% Crouzon syndrome FGFR2 100% Jackson-Weiss syndrome 95% Pfeiffer syndrome type 1 100% Pfeiffer syndrome types 2 and 3 100% FGFR2-related isolated coronal synostosis FGFR3 TWIST Our laboratory is pleased to announce that as of June 1, 2014, the connective tissue disorders panel has been expanded to include a total of 33 clinically useful genes. CLINICAL INDICATIONS FOR TESTING: Joint issues: hypermobility, dislocations, chronic pain Skin findings: cutis laxa, abnormal or atrophic scars, poor wound healing, spontaneous bruising Ocular findings: ectopia lentis, myopia, retinal detachment Pneumothorax Cardiac findings: congenital heart defect, mitral valve prolapse, aortic root enlargement, thoracic aneurysm, aortic dissection, other aneurysms/ dissections Skeletal variants: Tall or short stature, pectus excavatum, pectus carinatum, arachnodactyly, brachydactyly, pes planus, long wingspan Personal or family history of sudden cardiac death, aneurysm/dissection, rupture of internal organ, rectal or uterine prolapse Craniofacial anomalies or dysmorphic features SUSPECTED SYNDROMES: • Arterial tortuosity syndrome • Congenital contractural arachnodactyly (Beals syndrome) • Ehlers-Danlos syndrome (all subtypes) • ELN-related conditions: >50% Saethre-Chotzen syndrome 1 Greenwood, Jaclyn, Pamela Flodman, Kathryn Osann, Simeon A. Boyadjiev, and Virginia Kimonis. “Familial Incidence and Associated Symptoms in a Population of Individuals with Nonsyndromic Craniosynostosis.” Genetics in Medicine (September 26, 2013). doi:10.1038/gim.2013.134. 2 Robin, Nathaniel H, Falk, Marni J, and Haldeman-Englert, Chad R. "FGFR-Related Craniosynostosis Syndromes". In GeneReviewsTM, edited by Roberta A Pagon, Margaret P Adam, Thomas D Bird, Cynthia R Dolan, Chin-To Fong, and Karen Stephens. Seattle (WA): University of Washington, Seattle, 1993. http://www.ncbi.nlm.nih.gov/books/NBK1455/. FBN1 FBN2 ATP7A FKBP14 CBS FLNA CHST14 MYH11 COL1A1 MYLK COL1A2 PLOD1 COL2A1 SKI -- Marfan syndrome -- MASS phenotype -- Weill-Marchesani syndrome -- Isolated ectopia lentis COL3A1 SLC2A10 COL5A1 SLC39A13 COL5A2 SMAD3 FLNA-related cardiac valvular disease Homocystinuria Loeys-Dietz syndrome, types I, II, III, IV Myhre syndrome Shprintzen-Goldberg syndrome Stickler syndrome, types I, II, III, IV, V COL9A1 SMAD4 COL9A2 TGFB2 COL9A3 TGFBR1 COL11A1 TGFBR2 COL11A2 TNXB • Familial thoracic aneurysms and aortic dissections (TAAD) • FBN1-related disorders • • • • • • ABCC6 ACTA2 -- Autosomal dominant supravalvular aortic stenosis -- Cutis laxa 100% Crouzon syndrome with acanthosis nigricans 100% Muenke syndrome GENE LIST: ELN Human Genetics Laboratory Newsletter | Summer 2014