Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
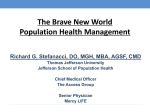
October 30, 2012 (Percentage) (Dollars in Billions) Inpatient Hospital 39 Physician Services 29 Outpatient 14 Skilled Nursing Facility 8 Home Health Agency 6 Hospice 4 Total 2010 Medicare Expenditures:331 Billion 130 96 46 26 20 13 2 Reduce preventable hospital readmissions Safe transition from SNF to home Provide lower cost, high quality alternative to acute care setting Provide patient-centered care 3 Part A (Hospital Insurance) Qualifying Hospital Stay – Inpatient hospital stay of 3 consecutive midnights Doctors orders for skilled services Skilled care required daily Up to100 day episode of care 4 Required for traditional Medicare Fee For Service under Part A Exceptions: ◦ Medicare Advantage (Part C) Tufts, Fallon, Blue Cross Blue Shield, etc. ◦ PACE-Program of All Inclusive Care for the Elderly ◦ SCO (Dual Eligible)-Senior Care Options ◦ MGH Waiver Program 5 UTI Dehydration Pneumonia COPD CHF Diabetes Hypertension 6 Part A (Hospital Insurance) Services provided under a plan of care established & reviewed regularly by a physician Require one or more of the following ◦ Skilled nursing care less than 7 days/week ◦ PT, OT or ST Certified homebound by physician Up to 60 day episode of care; 30 day window 7 24 – hour-a-day care at home Meals delivered to home Homemaker Services Personal Care (bathing, dressing and using the bathroom) when this is the only required care 8 Communicate with Skilled Nursing Facility and PCP Provides Consistent Care Givers Telemedicine – Early symptoms recognition and monitoring 9 Mismanagement of medications Moderate to severe functional impairment Inadequate patient/family education Lack of family safety net Comorbidities Patient reluctant to allow care givers in home Failure to keep follow up appointments Poor diet, insulin management Substance abuse 10 Discharge planning starts on admit date Communication with patient, family, PCP and home health agency Care management meetings with patient, nursing, therapy and case management Discharge meeting with home health care Family and Patient education PCP notification – medication, lab, pending tests and any special needs Electronic medical records 11 C.O.A.C. H. ◦ ◦ ◦ ◦ ◦ Communicate Expectations Organize goals Assign coach Continued review Handoff homework 12 Home Health Care Agency (HHCA) Case Manager ◦ Reviews patient chart w/SNF Interdisciplinary Team (IDT) ◦ Attends Discharge Planning Meeting at SNF ◦ Coordinates required services (Nursing, Therapy, etc.) with IDT SNF Case Manager ◦ Schedules Home evaluation ◦ Orders DME ◦ Provides education to family care givers 13 Conducts follow up calls with patient/family (within 48 hours) ◦ ◦ ◦ ◦ ◦ Seek feedback-How patient is succeeding at home Follow up on patient concerns Provide over the phone education Assist in providing additional/services if needed Readmit to facility within 30 days (3 day inpatient hospitalization not required) 14 Include home health care providers in the discharge process Educate home health care work force on SNF rules of participation, clinical capabilities, positive patient outcomes Create an image; the SNF is part of the continuum Common names; Rehab, Short Stay, Post Acute, Transitional Care Section 87 State Health Care Reform Law 15 Coordinate readmission process between home health nurses and SNF Track & trend outcome data and communicate results with stakeholders Expand Circle Events to include direct admits from physician offices and emergency rooms when appropriate Proposed State waiver of qualifying hospital stay 16