Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
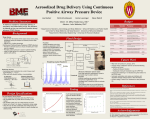
Respiratory Emergencies By Sydorenko O.L. Objectives Upon successful completion of this program, you should be able to: • review the signs and symptoms and field interventions for the patient presenting with COPD, and asthma. • review criteria for the use of CPAP. • review the SOP for Acute Objectives cont’d • review the Whisperflow patient circuit for CPAP used in the field. • review the set up of the albuterol nebulizer kit and in-line Albuterol set-up. CPAP Continuous Positive Airway Pressure A means of providing high flow, low pressure oxygenation to the patient in pulmonary edema CPAP • CPAP, if applied early enough, is an effective way to treat pulmonary edema and a means to prevent the need to intubate the patient • CPAP increases the airway pressures allowing for better gas diffusion & for reexpansion of collapsed alveoli • CPAP allows the refilling of collapsed, airless alveoli • CPAP allows/buys time for administered medications to be able to work CPAP expands the surface area of the collapsed alveoli allowing more surface area to be in contact with capillaries for gas exchange Before CPAP With CPAP Goal of Therapy With CPAP • Increase the amount of inspired oxygen • Decrease the work load of breathing In turn to: Decrease the need for intubation Decrease the hospital stay Decrease the mortality rate Patient Circuit COPD • Chronic obstructive pulmonary disease - a progressive and debilitating collection of diseases with airflow obstruction and abnormal ventilation with irreversible components (emphysema & chronic bronchitis) • Exacerbation of COPD is an increase in symptoms with worsening of the patient’s condition due to hypoxia that deprives tissue of oxygen and hypercapnia (retention of CO2) that causes an acid-base imbalance Obstructive Lung Disease COPD & Asthma • Abnormal ventilation usually from obstruction in the bronchioles • Common changes noted in the airways – bronchospasm - smooth muscle contraction – increased mucous production lining the respiratory tree – destruction of the cilia lining resulting in poor clearance of excess mucus – inflammation of bronchial passages resulting in accumulation of fluid and inflammatory cells Emphysema • Gradual destruction of the alveolar walls distal to the terminal bronchioles • Less area available for gas exchange • Small bronchiole walls weaken, lungs cannot recoil as efficiently, air is trapped • in number of pulmonary capillaries which resistance to pulmonary blood flow which leads to pulmonary hypertension – may lead to right heart failure & cor pulmonale (disease of the heart because of diseased lungs) Alveolar Sac and Capillaries Bronchioles capillary alveolus Interior of alveolus Emphysema • in PaO2 leads to in red blood cell production (to carry more oxygen) • Develop chronically elevated PaCO2 from retained carbon dioxide • Loss of elasticity/recoil; alveoli dilated • More common in men; major contributing factor is cigarette smoking; another contributing factor is environmental exposures • Patients more susceptible to acute respiratory infections and cardiac dysrhythmias Chronic Bronchitis • An increase in the number of mucous-secreting cells in the respiratory tree • Large production of sputum with productive cough • Diffusion remains normal because alveoli not severely affected • Gas exchange decreased due to lowered alveolar ventilation which creates hypoxia and hypercarbia Asthma • Chronic inflammatory disorder of the airways • Airflow obstruction and hyperresponsiveness are often reversible with treatment • Triggers vary from individual environmental allergens cold air; other irritants exercise; stress food; certain medications Asthma’s Two-Phase Reaction • Phase one - within minutes – Release of chemical mediators (ie: histamine) • contraction of bronchial smooth muscle (bronchoconstriction) • leakage of fluid from bronchial capillaries (bronchial edema) • Phase two - in 6-8 hours – Inflammation of the bronchioles from invasion of the mucosa of the respiratory tract from the immune system cells • additional swelling & edema of bronchioles Severe Asthma Attack • One and two word dyspnea • Tachycardia • Decreased oxygen saturation on pulse oximetry • Agitation & anxiety with increasing hypoxia Treatment Goals COPD & Asthma Relieve and correct hypoxia Reverse any bronchospasm or bronchoconstriction Asthma/COPD with Wheezing SOP • Routine medical care • Pulse oximetry (on room air if possible) • Albuterol 2.5 mg / 3ml with oxygen adjusted to 6 l/minute • May repeat Albuterol treatments if needed • May need to consider intubation with in-line administration of Albuterol based on the patient’s condition • EMS to contact Medical Control for possible CPAP in patient with COPD Albuterol Nebulizer Procedure • Medication is added to the chamber which must be kept upright • The T-piece is assembled over the chamber • The patient needs to be coached to breath slowly and as deeply as possible – this will take time and several breathes before the patient can slow down and start breathing deeper; the patient needs a good coach to talk them through the slower/deeper breathing – the medication needs to be inhaled into the lungs to be effective – the patient should be sitting upright Add medication to the chamber Connect the mouthpiece to the T-piece Connect the corrugated tubing to the T-piece Kit connected to oxygen and run at 6 l/minute (enough to create a mist) Encourage slow, deep breathing Albuterol Nebulizer Mask For the patient who is unable to keep their lips sealed around the mouthpiece, take the top T-piece off the kit and replace with an adult or pediatric nebulizer mask Pediatric patient using nebulizer mask. Caregiver may assist in holding the mask. What To Do in Extreme Asthma Attack • At times, the asthma attack is so severe the patient is at risk of dying • To relieve the bronchoconstriction, Albuterol needs to be delivered right into the lungs • To assist with this, the patient may need to be bagged or intubated to deliver the medication • Abuterol is delivered via in-line technique Aerosol Medication via BVM or ETT with BVM (In-line) • Albuterol placed in the chamber as usual • The chamber is connected to the T-piece • Adaptor(s) are used to accommodate bagging the patient with in-line Albuterol as soon as possible – any medication that can be delivered as soon as possible to the target organ (the lungs) will be helpful in promoting bronchodilation • Mouthpiece removed from T-piece and replaced with BVM • Nebulizer still connected to oxygen source • Adaptor placed at distal end of corrugated tubing to connect to BVM mask or ETT Albuterol Delivered Via BVM • #1 Disconnect reservoir bag with L valve from mask • #2 Connect L shaped valve with bag where mouthpiece of albuterol kit would fit • #3 Place corrugated tubing of albuterol kit to the mask over the patient’s mouth • #4 Begin to bag to “blow” the drug into the lungs while waiting to complete intubation #1 #2 #3, #4 To 6l O2 • Adaptor connected to the distal end of the corrugated tubing of Albuterol kit connected to the proximal end of the ETT • ETT placement confirmed in the usual manner – visualization – chest rise & fall – 5 point auscultation – ETCO detector Intubated patient