Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
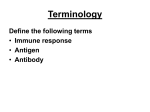
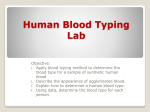
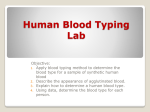
Case D – FBC Warm type Autoimmune Hemolytic Anemia Presented by: Meme Phung Zhi Yuan Quek Alison Wong Scenario A 25 year old female presented with a 2 week history of: progressive tiredness and dyspnoea on exertion. In the previous three weeks she had noted: intermittent migratory arthralgia Two years ago she had an episode of pleurisy. She denied taking any medications. Physical examination showed mucosal pallor with mild scleral icterus. The spleen was palpable (3cm), and the joints normal. Urinalysis showed a strong reaction to urobilinogen, but was negative for bilirubin and blood. Initial investigations included the following: Hb 65 g/L 115-165 MCV 99 fL 80-100 WCC 14.5X 109/L Platelets ESR 4.0-11.0 X109/L 350 X109/L 150-400 X109/L 58 mm/hr 3-9 Blood film Moderate anisocytosis with numerous spherocytes, prominent polychromasia and mild red cell agglutination. Nucleated red cells were present and there was a neutrophilia with occasional band forms. In view of the marked polychromasia, a recticulocyte count was suggested. *Recticulocyte 310 X 109/L 10-80 X 109/L (0.2(18%) 2.0%) In this patient, warm type autoimmune haemolytic anaemia (AIHA) is suspected. Warm type autoimmune haemolytic anaemia (AIHA) AIHA is an uncommon disorder due to a malfunction of the immune system that produces autoantibodies, which attack red blood cells as if they were antigens. Can occur at any age. Affect women more than men. Cause unknown (idiopathic autoimmune hemolytic anaemia) Destruction of RBCs (hemolysis) by autoantibodies may occur abruptly or insidiously. 2 Main types of AIHA 1. Warm type antibody hemolytic anaemia 2. Cold type antibody hemolytic anaemia Warm type antibody hemolytic anaemia 1. A warm reacting, positive direct antiglobulin test, where IgG or C3 (complement C3) is found on the RBC surface at 37C. 2. The antibody has its maximal activity at 37C, resultant hemolysis is called warm antibody induced hemolytic anaemia. 3. Severe life threatening condition. Clinical presentations 1. Symptoms: Symptoms of anaemia (e.g. weakness, tired, fever) Slight splenomegaly (enlarged spleen) Sudden onset of pallor Exercise intolerance Difficulty breathing Jaundice Dark urine 2. Clinical features: Common features of hemolysis (LOW hematocrit and Hb) High MCHC Autoagglutination WCC elevated Raised recticulocytes (= immature RBCs) Raised LDH Low Haptoglobins (=protein in blood that binds to free Hb) Raised serum total bilirubin Spherocytes and Red Cell Agglutination Agglutination = antibodies that agglutinate (‘clump to’) RBCs, causing damage to the RBCs which is subsequently removed in the spleen or liver in a form of extravascular hemolysis. The most common form of AIHA is incomplete or non-agglutinating antibodies. antibodies bind to the RBC membrane, but in insufficient quantity to cause intravascular hemolysis or agglutination. The RBC is then damaged, resulting in spherocyte formation. The RBC is not destroyed until they get phagocytocized in the spleen or liver. Agglutination Figure 1. Autoagglutination is visible on the sides of the blood tube. Figure 2. Microscopic agglutination of erythrocytes is visible in this blood smear Spherocytes Figure 3. Typical spherocyte, appearing as a small erythrocyte that lacks central pallor because of its spherical (rather than biconcave) shape Significance of presence of spherocytes: Show evidence of active hemolysis they’re spheroid because of lost membrane mass. Spherocytes are common features of warm antibody hemolytic anemia Elevated MCHC may be a clue to the presence of spherocytes From the patient’s blood film results: Blood film: moderate anisocytosis with numerous spherocytes prominent polychromasia and mild red cell agglutination. Nucleated red cells were present and there was a neutrophilia with occasional band forms. Warm type AIHA is suspected… Need to confirm diagnosis with Coomb’s antiglobulin test. Direct Antiglobulin Test (DAT) / Coomb’s Test What is it? To detect the presence of autoantibodies against the body’s own red blood cells Antibodies sometimes destroy red blood cells and cause anaemia Hallmark of AIHA warm-reacting, postive DAT IgG or C3 found on RBC surface at 37oC Principle Behind Results positive or negative false negative test results perform dilutions of the Coombs’ reagent to decrease the chance of false negative reactions false positive test results rarely occur 3 Types of Direct Antiglobulin Reactions 1. Direct antiglobulin positive with antiIgG and negative with anti-C3 idiopathic AIHA and in -methyldopaand penicillin-induced cases 2. Direct antiglobulin positive with antiIgG and anti-C3 SLE and idiopathic AIHA, not in drugassociated cases 3. Direct antiglobulin positive with anti-C3 but negative with anti-IgG idiopathic AIHA when IgG antibody low affinity, in some drug-associated cases and in cryopathic forms Back to patient: DAT positive; both IgG and complement demonstrated on red cells Signs and symptoms of SLE and not taking medications Conditions & Medications Associated with warm AIHA Disease associations with AIHA: 1. 2. 3. 4. 5. 6. Idiopathic Infections Neoplasms/Malignancies Autoimmunity Immune deficiency Miscellaneous Drug associations with AIHA: (eg. -methyldopa, levodopa, high-dose penicillin or cephalosporins, gold) Mechanisms implicated (when DAT positive) a) Drug absorption mechanism (hapten mechanism) b) Immune complex mechanism (“innocent bystander” mechanism) c) Autoantibody mechanism d) Membrane modification mechanism Patient has history of arthralgias and pleurisy, suggesting SLE underlying disease associated with her AIHA Systemic Lupus Erythematous What is SLE? Is an autoimmune disorder The cause is usually unknown Occurs predominantly in younger women Is a chronic inflammatory connective tissue disorder that can involve joints, kidneys, mucous membranes and blood vessel walls. It can range in severity from mild to life threatening. What are the symptoms? Fatigue, fever, anorexia, nausea weight loss, joint pain, and arthritis muscle pain facial or other skin rash, often made worse by sun exposure (commonly a "butterfly rash" that occurs over the nose and cheeks of the face) hair loss, depression, confusion, headache, chest pain, dry eyes and/or dry mouth repeated miscarriages Characteristics of Lupus At least four of the following symptoms are generally present for a diagnosis to be made: Malar rash Discoid rash Photosensitivity Oral ulcers Arthritis Serositis Leucopoenia (< 4000 mL), lymphonia (< 1500 /mL), haemolytic anaemia or thrombocytopenia (< 100,000/ mL) Neurologic disorder Anti-DNA antibody, anti-Sm antibody or evidence of antiphospholipid antibody Antinuclear antibodies on raised titer Laboratory Findings The fluorescent test for ANA (antinuclear antibody) screens for SLE It is present in a very high percentage (over 90%) of lupus patients Positive ANA tests (usually in high titer) occur in > 98 % of SLE patients Laboratory Findings Leads to more specific tests for anti-double stranded DNA antibodies High titers of anti-double stranded DNA antibodies are highly specific for SLE Other ANA and anticytoplasmic antibodies are diagnostically valuable in SLE eg anti-Ro, anti Sm, anti La, RNP, Jo-1 False positive serologic tests for syphilis occur in 5 to 10% of SLE patients Table 1. Numbers (percentage) of patients with SLE with anti-dsDNA antibodies and antinucleosome antibodies (n=95) From: Cairns: Ann Rheum Dis, Volume 62(3).March 2003.272-273 Treatment Mild Lupus NSAIDs, low dose Aspirin, hydroxychloroquine,chloroquine Severe Lupus immediate corticosteroid such as prednisone sometimes immunosuppressive drugs azathioprine or cyclophosphamide Conclusion Patient diagnosed with warm type AIHA This patient has a history of arthralgia and pleurisy suggesting SLE. Patient needs to confirm the diagnosis of SLE with a ANA test and anti-double stranded DNA test Haemolytic anaemia is associated with severe SLE which may require immediate corticosteroid therapy