Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
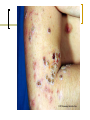
Skin – Immune Disorders Jan Bazner-Chandler CPNP, CNS, MSN, RN Key Function of Skin Protection – shield from internal injury. Immunity – contains cells that ingest bacteria and other substances. Thermoregulation – heat regulation through sweating, shivering, and subcutaneous insulation Communication / sensation / regeneration Developmental Variances Sweat glands function by the time the child is 3-years-old. The visco-elastic property of the dermis becomes completely functional at about 2 years. The neonate’s dermis is thin and very hydrated, thus is at greater risk for fluid loss and serves as an ineffective barrier. Diagnostic Tests Cultures Scraping Skin biopsy Skin testing Woods lamp Woods Lamp Neonatal skin lesions Vascular birth marks: hemangioma Port wine stain Abnormal pigmentation: Mongolian spots Neonatal acne: small red papules and pustules appear on face trunk. Milia: white or yellow, 1-2mm papules appearing on cheeks, nose, chin, and forehead Inflammatory Skin Disorders Diaper dermatitis Contact dermatitis Atopic dermatitis or eczema Diaper Dermatitis Diaper Dermatitis Identify causative agent Cleanse with mild cleaner Apply barrier Expose to air Teach hazards of baby powder Cradle Cap Rash that occurs on the scalp. It may cause scaling and redness of the scalp. It may progress to other areas. Treatment If confined to the scalp Wash area with mild baby shampoo and brush with a soft brush to help remove the scales. Do not apply baby oil or mineral oil to the area - this will only allow for more build up of the scales. Cradle Cap Baby Care Atopic dermatitis or Eczema Chronic, relapsing inflammation of the dermis and epidermis characterized by itching, edema, papules, erythema, excoriation, serous discharge and crusting. Patients have a heightened reaction to a variety of allergens. Dermatitis Assessment History of asthma, allergic rhinitis Lesions generally occur in creases. Management: Control the itching: OTC Benadryl Reduce inflammation: topical corticosteroids Hydrate the skin Elidel Cream Preventing infection Acne Vulgaris A chronic, inflammatory process of the pilosebaceous follicles. Occurrence; 85% of teenager aged 15 to 17 years. More common in females than males. Acne Over activity of oil glands at the base of hair follicles Hormone activity Skin cell “plug” pores causing white heads and blackheads. No “cure” Acne Management of Acne Topical medications OTC preparations Prescription - Topical retinoid preparations Prescription - Topical antibiotics Systemic medication Antibiotics Hormonal therapy – birth control pills Accutane * use with extreme caution when all else fails Pediculosis Head lice infestation ranges from 1% to 40% in children. Most common in ages 5 to 12. Less common in African American due to the shape of the hair shaft. Transmission by direct contact with infected person, clothing, grooming articles, bedding, or carpeting. Pediculosis Head lice Pubic lice Body lice Signs and Symptoms Symptoms: itching, whitish colored eggs at shaft of hair, redness at site of itching. Nits Empty nit case Viable nit Interventions Anti-lice shampoo Removal of nits Washing bedding, towels, anything child’s head may have come in contact with in hot soapy water. Vacuum all floors and rugs Do not need to fumigate the house Child can return to school after 1 day of treatment Scabies • • • • A contagious skin condition caused by the human skin mite. Tiny, eight-legged creature burrows within the skin and penetrate the epidermis and lays eggs Allergic reaction occurs Severe itching Assessment Pruritus especially profound at night or nap time. Lesions may be generalized but tend to distribute on the palms, soles and axillae In older children: finger webs, body creases, beltline and genitalia Management Permethrin cream is drug of choice Massage into all skin surfaces – neck to soles of feet - leave on for 8 to 14 hours. Clothing bedding and other contact items need to be washed in hot soapy water. Vacuum upholstered furniture - rugs Scabies Scabies Impetigo • • • The most common skin infection in children. Causative agent is carried in the nasal area. Bacteria invade the superficial skin. Causative agent Group A beta-hemolytic streptococcal (GABHS) Staph aureus Impetigo Spread Highly contagious skin infection. Most common among children. Spread through physical contact. Clothes, bedding, towels and other objects. Interventions •Good general hygiene – wash hands •Wash lesions with soap and water •Topical antibiotic therapy: (Bactroban) • Keflex PO – 2nd generation cephalosporin •New antibacterial: Altabax (2007) Outcomes Self-limiting No scarring or pox marks post infection. Super-infection especially in the neonate. Impetigo / cellulitis Cellulitis A full-thickness skin infection involving dermis and underlying connective tissue. Any part of the body can be affected. Cellulitis around the eyes is usually an extension of a sinus infection or otitis media. Assessment History and physical exam WBC count Blood culture Culturing organism from lesion aspiration. CT scan with peri-orbital cellulitis Clinical Manifestations Characteristic reddened or lilaccolored, swollen skin that pits when pressed with finger. Borders are indistinct. Warm to touch. Superficial blistering. Cellulitis Cellulitis Interventions Hospitalization if large area involved or facial cellulitis. IV antibiotics. Tylenol for pain management. Warm moist packs to area if ordered. Assess for spread If peri-orbital test for ocular movement and vision acuity Poison Oak, Ivy and Sumac Three potent antigens that characteristically produce an intense dermatologic inflammatory reaction when contact is made between the skin and the allergens contained in the plant. Poison Ivy Poison Oak Interventions Prevention: Wear long pants when hiking or playing in the brush. Wash with soap and water to remove sticky sap. Cleanse under finger nails. Sap on fur, clothing or shoes can last up to 1 week if not cleansed properly. Topical cortisone to lesions. Systemic Response Burns in Children Young children who have been severely burned have a higher mortality rate than adults. Shorter exposure to chemicals or temperature can injure child sooner. Increased risk for for fluid and heat loss due to larger body surface area. Burns in Children Burns involving more that 10% of TBSA require fluid resuscitation. Infants and children are at increased risk for protein and calorie deficiency due to decreased muscle mass and poor eating habits. Scarring in more severe. Burns in Children Immature immune system can lead to increased risk of infection. Delay in growth may follow extensive burns. Management of Burns Ascertain adequacy of airway, oxygen, intubation Large bore needle to deliver sufficient fluids at a rapid rate. Remove clothing and jewelry and examine. Alert The most common cause of unconsciousness in the flame burn patient is hypoxia due to smoke inhalation. Look for ash and soot around nares. Management of Burns Admission weight. Nasogastric tube to maintain gastric decompression. Foley catheter for urine specimen and monitor output. Evaluate burn area and determine the extent and depth of injury. Flame Burn Management NG tube in place. Catheter for fluid replacement. Ambulation to prevent problems associated with immobilization Percentage of Areas Affected Depth of Burns First Degree Burn Involves only the epidermis and part of the underlying skin layers. Area is hot, red, and painful, but without swelling or blistering. Sunburn is usually a first-degree burn. Second Degree Burn Involves the epidermis and part of the underlying skin layers. Pain is severe. Area is pink or red or mottled. Area is moist and seeping, swollen, with blisters. Third Degree or Full-thickness Involves injury to all layers of skin. Destroys the nerve and blood vessels No pain at first Area may be white, yellow, black or cherry red. Skin may appear dry and leathery. Wound Management Dead skin and debris are Carefully trimmed. Gauze with ointment is applied to burn wound. Wound Management Bowden, Dickey, Greenberg text Children and Their Families Wound Management Hydrotherapy is used to cleanse the wound. Gauze pads are used To debride the wound by removing exudates and previous applied Medication. Skin Grafts Removal of split-thickness Skin graft with dermatone. Healed donor site Compartment Syndrome Escharotomy / fasciotomy in a severely burned arm. Burn Wound Covering Therapy to Prevent Complications Elasticized garment and “air-plane” splints. Physical therapy to prevent contracture deformity. Burns Ball & Bender Flash burn from gasoline. Electrical burn caused by biting of electrical cord. Keep Kids Safe Infants Immune System No active immune response at birth Passive immunity from mother Potential for immune response is present / active response is lacking Immune Response IgG is received from mother transplacental and in breast milk 6 to 9 months infants start to produce IgG Immune system starts to assume defensive role Active immunity begins after exposure to antigens Neonatal Sepsis Can be caused by bacterial, fugal, parasitic or viral pathogens. Etiology: complex interaction of maternal-fetal colonization, transplacental immunity and physical and cellular defenses of the fetus and mother. Sepsis Laboratory confirmed blood stream infection Neonatal sepsis Mortality rate 50% 1 to 8 cases per 1000 live births Meningitis occurs in 1/3 Major Risk Factors Maternal prolonged rupture of membranes > 24 hours Intra-partum maternal fever > 38C Prematurity Sustained fetal tachycardia > 160 Minor Risk Factors Twin gestation Premature infant Low APGAR Maternal Group B Streptococcus Foul lochia Etiology Group B beta-hemolytic Streptococcus Escherichia coli Haemophilus Influenza Diagnostic Tests C-Reactive Protein * earliest indicator of infectious / inflammatory process CBC with differential WBC Blood Culture – rule out blood borne bacteria – sepsis (take 3 days for final culture results) Lumbar Puncture – rule out meningitis Urine Culture – rule out UTI Clinical Manifestations Respiratory distress Temperature instability > 99.6 (37 C) or < 97 (36 C) Gastrointestinal symptoms Tachypnea / apnea / hypoxia Vomiting, diarrhea, poor feeding Decreased activity: lethargic / not eating Blood Test C-Reactive Protein Protein appears within 6 hours or exposure Blood culture to identify causative agent Medical Management Ampicillin Gentamicin Cefotaxime Acyclovir: herpes Nursing Interventions Administer IV antibiotics Monitor therapeutic levels Monitor VS, temperature, O2 saturation Activity level Sucking Infant parent bonding Outcomes Newborn will achieve normalization of body function Parents will participate in care Newborn will demonstrate no signs of CV, neurological or respiratory compromise Newborn will experience no hearing loss as a result of antibiotic therapy SCIDS Severe Combined Immunodeficiency Disease Hereditary disease Absence of both humoral and cell mediated immunity Clinical Manifestations Susceptibility to infection Frequent infection Failure of infection to respond to antibiotic treatment Treatment Manage infection Bone marrow transplant Acquired Immunodeficiency Syndrome / AIDS Human immunodeficiency virus type 1 is a retro virus that attacks the immune system by destroying T lymphocytes. AIDS T lymphocytes are critical to fighting infection and developing immunity. HIV renders the immune system useless and the child is unable to fight infection. Killer T-cells Blood Testing in Infants Babies born to HIV-positive mothers initially test positive for HIV antibodies. Only 13 to 39% of these infants are actually infected. Infants who are not infected with HIV may remain positive until they are about 18- months-old. Treating Infants in Utero Routinely offer HIV testing to all pregnant women. Administration of zidovudine (AZT) can decrease the likelihood of perinatal transmission from 25% to 8%. Modes of Transmission Three chief modes of transmission: Sexual contact (both homosexual and heterosexual). Exposure to needles or other sharp instruments contaminated with blood or bloody body fluids. Mother-to-infant transmission before or around the time of birth. Symptoms in Children An infant who is HIV positive will generally exhibit symptoms between 9 months to 3 years. Failure to thrive Pneumonia, chronic diarrhea, opportunistic infections Encephalopathy: leading to developmental delay, or loss of previously obtained milestones. Interdisciplinary Interventions Maternal treatment during pregnancy. Newborn receives zidovudine for 6 weeks after birth. Prophylaxis with Septra or Bactrim when CD4 level starts to drop. Interventions Age-appropriate immunizations except those containing live attenuated viruses. Can be given when T-Cell count is adequate Chicken pox - Varicella MMR – measles, mumps, rubella Community Interventions Education and prevention are the best ways to manage AIDS. Safe sexual practices Monogamous relationship Avoidance of substances such as alcohol and drugs that can cloud judgment. Changes in HIV Number of infected newborns has dropped due to treatment of HIV infected mothers. HIV has become a chronic disease in children Team approach Emphasis on community teaching