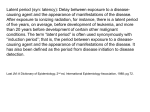
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Epidemiology of metabolic syndrome wikipedia , lookup
Diseases of poverty wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Preventive healthcare wikipedia , lookup
Seven Countries Study wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Race and health wikipedia , lookup
Infection control wikipedia , lookup
Compartmental models in epidemiology wikipedia , lookup
International Epidemiological Association wikipedia , lookup
Public health genomics wikipedia , lookup
Epidemiology Uses of epidemiology • Population or community health assessment • Individual decisions • Completing the clinical picture • Search for causes EPIDEMIOLOGY/ HIKMET QUBEILAT Population or community health assessment – What are the actual and potential health problems in the community? – Where are they? – Who is at risk? – Which problems are declining over time? – Which ones are increasing or have the potential to increase? – How do these patterns relate to the level and distribution of services available? EPIDEMIOLOGY/ HIKMET QUBEILAT Individual decisions – When they decide to stop smoking, – take the stairs instead of the elevator, – order a salad instead of a cheeseburger with French fries, – or choose one method of contraception instead of another – they may be influenced, consciously or unconsciously, by epidemiologists’ assessment of risk. EPIDEMIOLOGY/ HIKMET QUBEILAT Individual decisions (cont) – Since World War II, epidemiologists have provided information related to all those decisions. – In the 1950’s, epidemiologists documented the increased risk of lung cancer among smokers; – in the 1960’s and 1970’s, epidemiologists noted a variety of benefits and risks associated with different methods of birth control; EPIDEMIOLOGY/ HIKMET QUBEILAT Individual decisions – These and hundreds of other epidemiologic findings are directly relevant to the choices that people make every day, choices that affect their health over a lifetime EPIDEMIOLOGY/ HIKMET QUBEILAT Completing the clinical picture – When studying a disease outbreak, epidemiologists depend on clinical physicians and laboratory scientists for the proper diagnosis of individual patients. But epidemiologists also contribute to physicians’ understanding of the clinical picture and natural history of disease EPIDEMIOLOGY/ HIKMET QUBEILAT Completing the clinical picture • For example, in late 1989 three patients in New Mexico were diagnosed as having myalgias (severe muscle pains in chest or abdomen) and unexplained eosinophilia (an increase in the number of one type of white blood cell). Their physician could not identify the cause of their symptoms, or put a name to the disorder. Epidemiologists began looking for other cases with similar symptoms, and within weeks had found enough additional cases of eosinophiliamyalgia syndrome to describe the illness, its complications, and its rate of mortality. EPIDEMIOLOGY/ HIKMET QUBEILAT Search for causes – Much of epidemiologic research is devoted to a search for causes, factors which influence one’s risk of disease. Sometimes this is an academic pursuit, but more often the goal is to identify a cause so that appropriate public health action might be taken – It has been said that epidemiology can never prove a causal relationship between an exposure and a disease. Nevertheless, epidemiology often provides enough information to support effective action EPIDEMIOLOGY/ HIKMET QUBEILAT The Epidemiologic Approach – Like a newspaper reporter, an epidemiologist determines What, When, Where, Who, and Why. – However, the epidemiologist is more likely to describe these concepts in slightly different terms: case definition, time, place, person, and causes. EPIDEMIOLOGY/ HIKMET QUBEILAT Case Definition – is a set of standard criteria for deciding whether a person has a particular disease or other health-related condition. – By using a standard case definition we ensure that every case is diagnosed in the same way, regardless of when or where it occurred, or who identified it. We can then compare the number of cases of the disease that occurred in one time or place with the number that occurred at another time or another place EPIDEMIOLOGY/ HIKMET QUBEILAT – For example, with a standard case definition, we can compare the number of cases of hepatitis A that occurred in New York City in 1991 with the number that occurred there in 1990. – Or we can compare the number of cases that occurred in New York in 1991 with the number that occurred in San Francisco in 1991. – With a standard case definition, when we find a difference in disease occurrence, we know it is likely to be a real difference rather than the result of differences in how cases were diagnosed. EPIDEMIOLOGY/ HIKMET QUBEILAT – A case definition consists of clinical criteria and, sometimes, limitations on time, place, and person. The clinical criteria usually include confirmatory laboratory tests, if available, or combinations of symptoms (subjective complaints), signs (objective physical findings), and other findings. – A case definition may have several sets of criteria, depending on how certain the diagnosis is. For example, during an outbreak of measles, we might classify a person with a fever and rash as having a suspect, probable, or confirmed case of measles, depending on what additional evidence of measles was present. EPIDEMIOLOGY/ HIKMET QUBEILAT – . In other situations, we temporarily classify a case as suspect or probable until laboratory results are available. When we receive the laboratory report, we then reclassify the case as either confirmed or “not a case,” depending on the lab results. In the midst of a large outbreak of a disease caused by a known agent, we may permanently classify some cases as suspect or probable, because it is unnecessary and wasteful to run laboratory tests on every patient with a consistent clinical picture and a history of exposure (e.g., chickenpox) ). – Case definitions should not rely on laboratory culture results alone, since organisms are sometimes present without causing disease. EPIDEMIOLOGY/ HIKMET QUBEILAT – Case definitions may also vary according to the purpose for classifying the occurrences of a disease. – For such rare but potentially severe communicable diseases, where it is important to identify every possible case, health officials use a sensitive, or “loose” case definition. On the other hand, investigators of the causes of a disease outbreak want to be certain that any person included in the investigation really had the disease EPIDEMIOLOGY/ HIKMET QUBEILAT – The investigator will prefer a specific or “strict” case definition. For instance, in an outbreak of Salmonella agona, the investigators would be more likely to identify the source of the infection if they included only persons who were confirmed to have been infected with that organism, rather than including anyone with acute diarrhea, because some persons may have had diarrhea from a different cause. In this setting, the only disadvantage of a strict case definition is an underestimate of the total number of cases. EPIDEMIOLOGY/ HIKMET QUBEILAT Numbers and Rates – A basic task of a health department is counting cases in order to measure and describe morbidity. When physicians diagnose a case of a reportable disease they send a report of the case to their local health department. These reports are legally required to contain information on time (when the case occurred), place (where the patient lived), and person (the age, race, and sex of the patient). – The health department combines the reports and summarizes the information by time, place, and person. EPIDEMIOLOGY/ HIKMET QUBEILAT – From these summaries, the health department determines the extent and patterns of disease occurrence in the area, and identifies clusters or outbreaks of disease. A simple count of cases, however, does not provide all the information a health department needs. To compare the occurrence of a disease at different locations or during different times, a health department converts the case counts into rates, which relate the number of cases to the size of the population where they occurred. Rates are useful in many ways. With rates, the health department can identify groups in the community with an elevated risk of disease. EPIDEMIOLOGY/ HIKMET QUBEILAT • These so-called high-risk groups can be further assessed and targeted for special intervention; the groups can be studied to identify risk factors that are related to the occurrence of disease. Individuals can use knowledge of these risk factors to guide their decisions about behaviors that influence health. EPIDEMIOLOGY/ HIKMET QUBEILAT Descriptive Epidemiology – In descriptive epidemiology, we organize and summarize data according to time, place, and person. These three characteristics are sometimes called the epidemiologic variables. Compiling and analyzing data by time, place, and person is desirable for several reasons. – First, the investigator becomes intimately familiar with the data and with the extent of the public health problem being investigated. – Second, this provides a detailed description of the health of a population that is easily communicated. – Third, such analysis identifies the populations that are at greatest risk of acquiring a particular disease. This information provides important clues to the causes of the disease, and these clues can be turned into testable hypotheses. EPIDEMIOLOGY/ HIKMET QUBEILAT Time – Disease rates change over time. Some of these changes occur regularly and can be predicted. For example, the seasonal increase of influenza cases with the onset of cold weather is a pattern that is familiar to everyone. By knowing when flu outbreaks will occur, health departments can time their flu shot campaigns effectively. Other disease rates make unpredictable changes. By examining events that precede a disease rate increase or decrease, we may identify causes and appropriate actions to control or prevent further occurrence of the disease. EPIDEMIOLOGY/ HIKMET QUBEILAT – We usually show time data as a graph. We put the number or rate of cases or deaths on the vertical, yaxis; – we put the time periods along the horizontal, x-axis. – We often indicate on a graph when events occurred that we believe are related to the particular health problem described in the graph. – For example, we may indicate the period of exposure or the date control measures were implemented. Such a graph provides a simple visual depiction of the relative size of a problem, its past trend and potential future course, as well as how other events may have affected the problem. Studying such a graph often gives us insights into what may have caused the problem. EPIDEMIOLOGY/ HIKMET QUBEILAT – Depending on what event we are describing, we may be interested in a period of years or decades, or we may limit the period to days, weeks, or months when the number of cases reported is greater than normal (an epidemic period) – For some conditions—for many chronic diseases, for example—we are interested in long-term changes in the number of cases or rate of the condition. For other conditions, we may find it more revealing to look at the occurrence of the condition by season, month, day of the week, or even time of day. EPIDEMIOLOGY/ HIKMET QUBEILAT – For a newly recognized problem, we need to assess the occurrence of the problem over time in a variety of ways until we discover the most appropriate and revealing time period to use. Some of the common types of time-related graphs are further described below. Secular (long-term) trends. Graphing the annual cases or rate of a disease over a period of years shows long-term or secular trends in the occurrence of the disease. We commonly use these trends to suggest or predict the future incidence of a disease. We also use them in some instances to evaluate programs or policy decisions, or to suggest what caused an increase or decrease in the occurrence of a disease, particularly if the graph indicates when related events took place EPIDEMIOLOGY/ HIKMET QUBEILAT – Seasonality. By graphing the occurrence of a disease by week or month over the course of a year or more we can show its seasonal pattern, if any. Some diseases are known to have characteristic seasonal distributions; for example, as mentioned earlier, the number of reported cases of influenza typically increases in winter. Seasonal patterns may suggest hypotheses about how the infection is transmitted, what behavioral factors increase risk, and other possible contributors to the disease or condition. The seasonal pattern of farm tractor fatalities is shown in Figure 1.4.Epi_Course.pdf What factors might contribute to its seasonal pattern? Notice that Figure 1.5 shows the occurrence of a disease event over the course of a year. EPIDEMIOLOGY/ HIKMET QUBEILAT – Day of week and time of day. Displaying data by days of the week or time of day may also be informative. Analysis at these shorter time periods is especially important for conditions that are potentially related to occupational or environmental exposures, which may occur at regularly scheduled intervals. – In Figure 1.6,Epi_Course.pdf farm tractor fatalities are displayed by days of the week. Does this analysis at shorter time periods suggest any hypothesis? – In Figure 1.6 the number of farm tractor fatalities on Sundays is about half the number on the other days. We can only speculate why this is. One reasonable hypothesis is that farmers spend fewer hours on their tractors on Sundays than on the other days. EPIDEMIOLOGY/ HIKMET QUBEILAT Place We describe a health event by place to gain insight into the geographical extent of the problem. For place, we may use place of residence, birthplace, place of employment, school district, hospital unit, etc., depending on which may be related to the occurrence of the health event. Similarly, we may use large or small geographic units: country, state, county, census tract, street address, map coordinates, or some other standard geographical designation. Sometimes, we may find it useful to analyze data according to place categories such as urban or rural, domestic or foreign, and institutional or non institutional. EPIDEMIOLOGY/ HIKMET QUBEILAT – Not all analyses by place will be equally informative. By analyzing data by place, we can also get an idea of where the agent that causes a disease normally lives and multiplies, what may carry or transmit it, and how it spreads. When we find that the occurrence of a disease is associated with a place, we can infer that factors that increase the risk of the disease are present either in the persons living there (host factors) or in the environment, or both. For example, diseases that are passed from one person to another spread more rapidly in urban areas than in rural ones, mainly because the greater crowding in urban areas provides more opportunities for susceptible people to come into contact with someone who is infected. EPIDEMIOLOGY/ HIKMET QUBEILAT – On the other hand, diseases that are passed from animals to humans often occur in greater numbers in rural and suburban areas because people in those areas are more likely to come into contact with disease-carrying animals, ticks, and the like. For example, perhaps Lyme disease has become more common because people have moved to wooded areas where they come into contact with infected deer ticks. EPIDEMIOLOGY/ HIKMET QUBEILAT – Although we can show data by place in a table—does—it is often better to show it pictorially in a map. – On a map, we can use different shadings, color, or line patterns to indicate how a disease or health event has different numbers or rates of occurrence in different areas, EPIDEMIOLOGY/ HIKMET QUBEILAT PERSON In descriptive epidemiology, when we organize or analyze data by “person” there are several person categories available to us We may use inherent characteristics of people (for example, age, race, sex), their acquired characteristics (immune or marital status), their activities (occupation, leisure activities, use of medications/tobacco/drugs), or the conditions under which they live (socioeconomic status, access to medical care). EPIDEMIOLOGY/ HIKMET QUBEILAT These categories determine to a large degree who is at greatest risk of experiencing some undesirable health condition, such as becoming infected with a particular disease organism. We may show person data in either tables or graphs. In analyzing data by person, we often must try a number of different person categories before we find which are the most useful and enlightening. EPIDEMIOLOGY/ HIKMET QUBEILAT – Age and sex are most critical; we almost always analyze data according to these. – Depending on what health event we are studying, we may or may not break the data down by the other attributes. – Often we analyze data into more than one category simultaneously; for example, we may look at age and sex simultaneously to see if the sexes differ in how they develop a condition that increases with age—as they do for heart disease. EPIDEMIOLOGY/ HIKMET QUBEILAT Age – . Age is probably the single most important “person” attribute, because almost every health-related event or state varies with age. A number of factors that also vary with age are behind this association: susceptibility, opportunity for exposure, latency or incubation period of the disease, and physiologic response (which affects, among other things, disease development). EPIDEMIOLOGY/ HIKMET QUBEILAT – When we analyze data by age, we try to use age groups that are narrow enough to detect any age-related patterns that may be present in the data. – In an initial breakdown by age, we commonly use 5-year age intervals: 0 to 4 years, 5 to 9, 10 to 14, and so on. EPIDEMIOLOGY/ HIKMET QUBEILAT Larger intervals, such as 0 to 19 years, 20 to 39, etc., can conceal variations related to age which we need to know to identify the true population at risk. Sometimes, even the commonly used 5year age groups can hide important differences. EPIDEMIOLOGY/ HIKMET QUBEILAT SEX – In general, males have higher rates of illness and death than females do for a wide range of diseases. For some diseases, this sex-related difference is because of genetic, hormonal, anatomic, or other inherent differences between the sexes. – These inherent differences affect their susceptibility or physiologic responses. EPIDEMIOLOGY/ HIKMET QUBEILAT For example, premenopausal women have a lower risk of heart disease than men of the same age. This difference is attributed to higher estrogen levels in women. On the other hand, the sex-related differences in the occurrence of many diseases reflect differences in opportunity or levels of exposure. EPIDEMIOLOGY/ HIKMET QUBEILAT – You may have attributed the higher level of disorders in females to their higher level of exposure to occupational activities that require repetitive hand/wrist motion such as typing or keyboard entry. – With occupationally-related illness, we usually find that sex differences reflect the number of workers in those occupations. You may also have attributed the higher level of disorders in females to anatomical differences; perhaps women’s wrists are more susceptible to hand/wrist disorders. EPIDEMIOLOGY/ HIKMET QUBEILAT Ethnic and racial groups. • In examining epidemiologic data, we are • interested in any group of people who have lived together long enough to acquire common characteristics, either biologically or socially. Several terms are commonly used to identify such groups: race, nationality, religion, or local reproductive or social groups, such as tribes and other geographically or socially isolated groups. EPIDEMIOLOGY/ HIKMET QUBEILAT Differences that we observe in racial, ethnic, or other groups may reflect differences in their susceptibility or in their exposure, or they may reflect differences in other factors that bear more directly on the risk of disease, such as socioeconomic status and access to health care. EPIDEMIOLOGY/ HIKMET QUBEILAT Socioeconomic status. • Socioeconomic status is difficult to quantify. It is • made up of many variables such as occupation, family income, educational achievement, living conditions, and social standing. The variables that are easiest to measure may not reflect the overall concept. Nevertheless, we commonly use occupation, family income, and educational achievement, while recognizing that these do not measure socioeconomic status precisely. The frequency of many adverse health conditions increases with decreasing socioeconomic status. EPIDEMIOLOGY/ HIKMET QUBEILAT For example, tuberculosis is more common among persons in lower socioeconomic strata. Infant mortality and time lost from work due to disability are both associated with lower income. These patterns may reflect more harmful exposures, lower resistance, and less access to health care. EPIDEMIOLOGY/ HIKMET QUBEILAT – Or they may in part reflect an interdependent relationship which is impossible to untangle— does low socioeconomic status contribute to disability or does disability contribute to lower socioeconomic status? – Some adverse health conditions are more frequent among persons of higher socioeconomic status. These conditions include breast cancer, Kawasaki syndrome, and tennis elbow. Again, differences in exposure account for at least some of the differences in the frequency of these conditions. EPIDEMIOLOGY/ HIKMET QUBEILAT Analytic Epidemiology • As you have seen, with descriptive epidemiology • we can identify several characteristics of persons with disease, and we may question whether these features are really unusual, but descriptive epidemiology does not answer that question. Analytic epidemiology provides a way to find the answer: the comparison group. Comparison groups, which provide baseline data, are a key feature of analytic epidemiology. EPIDEMIOLOGY/ HIKMET QUBEILAT – For example, in one outbreak of hepatitis A, it was found that almost all of those infected ate pastries from a particular bakery and drank city water . However, without knowing the habits of persons without hepatitis, it was not possible to conclude that pastries, city water, or both were risk factors for hepatitis. Therefore, a comparison group of healthy persons from the same population were questioned. Among the comparison group without hepatitis, almost all drank city water but few were exposed to the pastries. This finding indicated that pastries from the particular bakery were a risk factor for hepatitis A. EPIDEMIOLOGY/ HIKMET QUBEILAT – When—as in the example above—we find that persons with a particular characteristic are more likely than those without the characteristic to develop a certain disease, then the characteristic is said to be associated with the disease. – Identifying factors that are associated with disease helps us identify populations at increased risk of disease; we can then target public health prevention and control activities. Identifying risk factors also provides clues to direct research activities into the causes of a disease. EPIDEMIOLOGY/ HIKMET QUBEILAT – Thus, analytic epidemiology is concerned with the search for causes and effects, or the why and the how. – We use analytic epidemiology to quantify the association between exposures and outcomes and to test hypotheses about causal relationships. It is sometimes said that epidemiology can never prove that a particular exposure caused a particular outcome. Epidemiology may, however, provide sufficient evidence for us to take appropriate control and prevention measures EPIDEMIOLOGY/ HIKMET QUBEILAT Epidemiologic studies fall into two categories: experimental and observational. In an experimental study, we determine the exposure status for each individual (clinical trial) or community (community trial); we then follow the individuals or communities to detect the effects of the exposure. In an observational study, which is more common, we simply observe the exposure and outcome status of each study participant. The study of hepatitis A cases described above was an observational study. EPIDEMIOLOGY/ HIKMET QUBEILAT – Two types of observational studies are the cohort study and the case-control study. A cohort study is similar in concept to the experimental study. We categorize subjects on the basis of their exposure and then observe them to see if they develop the health conditions we are studying. This differs from an experimental study in that, in a cohort study, we observe the exposure status rather than determine it. After a period of time, we compare the disease rate in the exposed group with the disease rate in the unexposed group. EPIDEMIOLOGY/ HIKMET QUBEILAT The length of follow-up varies, ranging from a few days for acute diseases to several decades for cancer, cardiovascular disease, and other chronic diseases. The Framingham study is a well-known cohort study which has followed over 5,000 residents of Framingham, Massachusetts, since the early 1950’s to establish the rates and risk factors for heart disease EPIDEMIOLOGY/ HIKMET QUBEILAT – The case-control study—the other type of observational study—is more common than the cohort study. In a case-control study, we enroll a group of people with disease (“cases”) and a group without disease (“controls”) and compare their patterns of previous exposures. The study of hepatitis A described above is an example of a case-control study. The key in a case-control study is to identify an appropriate control, or comparison, group, because it provides our measure of the expected amount of exposure. EPIDEMIOLOGY/ HIKMET QUBEILAT – In summary, the purpose of an epidemiologic study is to quantify the relationship between an exposure and a health outcome. – The hallmark of an epidemiologic study is the presence of at least two groups, one of which serves as a comparison group. – In an experimental study, the investigator determines the exposure for the study subjects; in an observational study, the subjects determine their own exposure. EPIDEMIOLOGY/ HIKMET QUBEILAT In an observational cohort study, subjects first are enrolled on the basis of their exposure, then are followed to document occurrence of disease. In an observational case-control study, subjects first are enrolled according to whether they have the disease or not, then are questioned or tested to determine their prior exposure. EPIDEMIOLOGY/ HIKMET QUBEILAT Causation – we will define a cause of disease as a factor (characteristic, behavior, event, etc.) that influences the occurrence of disease. An increase in the factor leads to an increase in disease. Reduction in the factor leads to a reduction in disease. – If disease does not develop without the factor being present, then we term the causative factor “necessary.” – If the disease always results from the factor, then we term the causative factor “sufficient.” – below. EPIDEMIOLOGY/ HIKMET QUBEILAT Exposure to Mycobacterium tuberculosis is necessary for tuberculosis to develop, but it is not sufficient, because not everyone infected develops disease. On the other hand, exposure to a large inoculum of rabies virus is a sufficient cause in a susceptible person, since clinical rabies and death will almost inevitably occur. A variety of models of disease causation have been proposed. Models are purposely simplified representations. In this instance, the purpose of the model is to facilitate the understanding of nature, which is complex. Two of these models are discussed EPIDEMIOLOGY/ HIKMET QUBEILAT The Epidemiologic Triad: Agent, Host, and Environment – The epidemiologic triangle or triad is the traditional model of infectious disease causation. It has three components: an external agent, a susceptible host, and an environment that brings the host and agent together. In this model, the environment influences the agent, the host, and the route of transmission of the agent from a source to the host. shows two versions of this model in diagram form. EPIDEMIOLOGY/ HIKMET QUBEILAT Agent factors • Agent originally referred to an infectious microorganism—virus, bacterium, parasite, or other microbe. Generally, these agents must be present for disease to occur. That is, they are necessary but not always sufficient to cause disease. As epidemiology has been applied to noninfectious conditions, the concept of agent in this model has been broadened to include chemical and physical causes of disease. EPIDEMIOLOGY/ HIKMET QUBEILAT These include chemical contaminants, such as the l-tryptophan contaminant responsible for eosinophiliamyalgia syndrome, and physical forces, such as repetitive mechanical forces associated with carpal tunnel syndrome. This model does not work well for some noninfectious diseases, because it is not always clear whether a particular factor should be classified as an agent or as an environmental factor. EPIDEMIOLOGY/ HIKMET QUBEILAT Host factors • Host factors are intrinsic factors that influence an individual’s exposure, susceptibility, or response to a causative agent. Age, race, sex, socioeconomic status, and behaviors (smoking, drug abuse, lifestyle, sexual practices and contraception, eating habits) are just some of the many host factors which affect a person’s likelihood of exposure. Age, genetic composition, nutritional and immunologic status, anatomic structure, presence of disease or medications, and psychological makeup are some of the host factors which affect a person’s susceptibility and response to an agent. EPIDEMIOLOGY/ HIKMET QUBEILAT Environmental factors – Environmental factors are extrinsic factors which affect the agent and the opportunity for exposure. Generally, environmental factors include physical factors such as geology, climate, and physical surroundings (e.g., a nursing home, hospital); biologic factors such as insects that transmit the agent; and socioeconomic factors such as crowding, sanitation, and the availability of health services. EPIDEMIOLOGY/ HIKMET QUBEILAT Agent, host, and environmental factors interrelate in a variety of complex ways to produce disease in humans. Their balance and interactions are different for different diseases. When we search for causal relationships, we must look at all three components and analyze their interactions to find practical and effective prevention and control measures. EPIDEMIOLOGY/ HIKMET QUBEILAT Component Causes and Causal Pies – One of the newer models is based on the multi factorial nature of causation in many diseases. It illustrates the factors that act to cause disease as pieces of a pie, the whole pie making up the sufficient cause for a disease. Notice that it shows that a disease may have more than one sufficient cause, with each sufficient cause being composed of several factors. What is the letter of the necessary cause shown for the hypothetical disease illustrated by this model? The factors represented by the pieces of the pie in this model are called component causes. EPIDEMIOLOGY/ HIKMET QUBEILAT They include intrinsic host factors, as well as the agent and the environmental factors of the agenthost-environment model. A single component cause is rarely a sufficient cause by itself. For example, even exposure to a highly infectious agent such as measles virus does not invariably result in measles disease—the host must be susceptible; other host factors may also play a role. EPIDEMIOLOGY/ HIKMET QUBEILAT – At the other extreme, an agent which rarely causes disease in healthy persons may be pathogenic when other conditions are right. Pneumocystis carinii is one such organism, harmlessly colonizing some healthy persons but causing potentially lethal pneumonia in persons whose immune systems have been weakened by human immunodeficiency virus (HIV). Presence of Pneumocystis carinii organisms is therefore a necessary but not sufficient cause of pneumocystis pneumonia. In Figure 1.15 it would be represented by component A in each “pie.” EPIDEMIOLOGY/ HIKMET QUBEILAT If the three pies in the model represented all the sufficient causes for a particular disease, component A would be considered a necessary cause for the disease, as P. carinii is for pneumocystis pneumonia. Because component A is included in all sufficient causes for the disease, it would have to be present, usually with various combinations of other factors, for disease to occur. Infectious agents are likely to be represented by component A As the model indicates, a particular disease may result from a variety of different sufficient causes. They are different pathways leading to the same end. EPIDEMIOLOGY/ HIKMET QUBEILAT – For example, lung cancer may result from a sufficient cause which includes smoking as a component cause. Smoking is not a sufficient cause by itself, however, since not all smokers develop lung cancer. Neither is smoking a necessary cause, because lung cancer may occur in persons who never smoked. Thus smoking may be represented by component B, which is present in sufficient causes I and II but not in III. – Asbestos exposure may be represented by component C, present in causes I and III but not in II. Indeed, since lung cancer may develop in persons with neither smoking or asbestos exposure, there would have to be at least one other sufficient cause pie that did not include components B and C. EPIDEMIOLOGY/ HIKMET QUBEILAT – To apply this model, we do not have to identify every component of a sufficient cause before we can take preventive action. We can prevent disease by blocking any single component of a sufficient cause, at least through that pathway. For example, eliminating smoking (component B) would prevent lung cancer from sufficient causes I and II, although some lung cancer would still occur through sufficient cause III. EPIDEMIOLOGY/ HIKMET QUBEILAT – In summary, the purpose of an epidemiologic study is to quantify the relationship between an exposure and a health outcome. The hallmark of an epidemiologic study is the presence of at least two groups, one of which serves as a comparison group. In an experimental study, the investigator determines the exposure for the study subjects; in an observational study, the subjects determine their own exposure. In an observational cohort study, subjects first are enrolled on the basis of their exposure, then are followed to document occurrence of disease. In an observational casecontrol study, subjects first are enrolled according to whether they have the disease or not, then are questioned or tested to determine their prior exposure. EPIDEMIOLOGY/ HIKMET QUBEILAT