Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
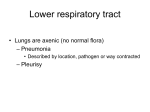
Community-Acquired Pneumonia: A Clinical case scenario Outline Diagnosis of CAP Site of care? Tools for risk assessment? Diagnostic tests needed? Management of severe CAP ? Presentation A 66-year-old man accompanied by his wife, arrived at the Emergency Department complaining of shortness of breath, fever, and cough. Symptoms His symptoms started 8 days ago with mild fever, cough, myalgia, headache & sore throat were he received antipyretic, antihistaminic and cough syrup after consulting his family doctor through a telephone call. Symptoms After initial improvement, he had a worsening of symptoms starting 3 days ago with productive cough, pleuritic chest pain, fever, chills and malaise. Last night he developed dyspnea and high fever, so he decided to come to the Emergency Department today. Medical History X-smoker 2 years (30 pack years). COPD. Type 2 diabetes. Medications include Inhaled salbutamol (100 μg)+ beclomethasone diproprionate (50 μg) 2 puffs x 3. Sustained released theophylline (200mg cap 1x2). Gliclcazide (80mg tab. 1x1). Examination Confused. Temperature: 39.0°C. Blood pressure: 120/70. Pulse rate: 120 bpm. Respiratory rate: 30 per minute. Clinical signs of right upper zone consolidation and bilateral scattered rhonchi. No cyanosis, pedal edema or jugular venous distension is noted. Chest X-ray Diagnosis Dose this patient have Community-Acquired Pneumonia (CAP)? Definition of CAP Infection of the lung parenchyma in a person who is not hospitalized or living in a long-term care facility for ≥ 2 weeks. CAP: Diagnosis Clinical features: Productive cough, dyspnea, fever, clinical signs of consolidation Radiological findings: Consolidation “In addition to a constellation of suggestive clinical features, a demonstrable infiltrate by chest radiograph or other imaging technique, with or without supporting microbiological data, is required for the diagnosis of pneumonia.” CAP – Risk Factors for Pneumonia Elderly Smoking COPD Extreme weather Overcrowding Alcoholism DM Renal insufficiency CHF Chronic liver disease Immunossuppresio n Loss of consciousness Seizures What is the value of CXR in CAP? Establish Dx Evaluation of severity e.g. multilobar or bilateral, pleural effusion. Co-existing conditions e.g. bronchial obstruction, abscess. Pattern Infiltrate Patterns and Pathogens Initial investigations at ER: Hgb 13.4 gm/dl, Hct 40%. WBC 15,800/μl with 88% polymorphonuclear cells, 8% bands. Na+ 137 mEq/L, K+ 3.7 mEq/L. BUN 32 mg/dl, creatinine1.8 mg/dl. RBG 260 mg/dl. Arterial blood gas (room air): pH 7.38, PCO 2 53 mmHg, PO 2 58mmHg, O 2 Sat.% 89% CAP – Management based on PSI Score Would you hospitalize him? Assess the ability to safely and reliably take oral medication & the availability of outpatient support resources CURB 65 score Thorax 2003,58:377 (If study performed) Pneumonia Severity Index (PSI) score <60mmHg / SO 2 <90% Calculation of risk assessment (PSI score) PSI= 146 Class V→ ICU What testing would you do? Diagnostic testing “Recommendations for diagnostic testing remain controversial.” No convincing data that they improve outcomes. Outpatient setting: optional Inpatient setting: Critically ill CAP Specific pathogens (suspected) Diagnostic testing: Critically ill CAP Sputum: Gram staining and culture. Blood cultures. Urinary antigen tests for Legionella & Streptococcus pneumoniae. ± others FOB+BAL / Endotracheal tube aspirate Thoracentesis TNA What testing would you do? Pretreatment: Sputum: Gram staining and culture. Expectorated sputum should be deep cough specimen obtained before antibiotic treatment and it should be rapidly transported and processed within a few hours of collection.* Blood cultures (2 sets) 2 sets of blood cultures should be drawn before initiation of antibiotic therapy during the first 24 hour.* What treatment would you prescribe? General & supportive Therapy Antibiotic Fluid / diet Antipyretics (Paracetamol IV) Sugar blood chart & Insulin accordingly Cough syrup SR theophylline Inhalation ttt → salbutamol + ipratropium bromide O2 therapy → NP 2 L/min Empiric Antibiotic ttt What antibiotics are appropriate? CAP: When to start empiric therapy? As soon as possible in ED CAP: delay-to-AB> 4h after arrival Increased mortality Increased LOS Recommended empirical antibiotics for CAP: Inpatient, ICU ttt b-lactam plus either azithromycin or a respiratory fluoroquinolone (cefotaxime, ceftriaxone) Levofloxacin 750mg/24h + Ceftriaxone 1gm /12h IV 2 hours after ICU admission Sputum (gram stain) →Gram-positive diplococcus Value of Gram stain First, it broadens initial empirical coverage for less common etiologies, such as infection with S. aureus or gram-negative organisms. * Second, it can validate the subsequent sputum culture result. A positive Gram stain was highly predictive of a subsequent positive culture.* Day 3 Sputum culture & Sensitivity: Streptococcus pneumoniae Sensitive→ Cefotaxime, Ceftraixone and Levofloxacin. Susceptibility testing should guide antibiotic choice when results are available. Continue on the same antibiotics Day 3: The patient's condition began to improve, but fever persisted. Day 5: The patient was a febrile for the first time. Normal oral intake started. Cough, dyspnea grade & chest wheezes improved. Pulse 90 bpm, B/P 140/80. WBC 6,800/μl with 3% bands. BUN 18 mg/dl, creatinine1.4 mg/dl, 2 PPBS 170mg/dl. O 2 Sat.% on RA: 93%. Transferred to ward. Switch from intravenous to oral therapy? Afebrile No abnormal GIT absorption Cough & respiratory distress improved WBC returning to normal Levofloxacin 750 mg tab/24hr Day 8: Clinically stable Afebrile for 3days. CXR: partial resolution. Blood culture: No growth up till now. CAP: Duration of Therapy? “A minimum of 5 days… Afebrile for 48-72 h … No more than 1 CAPassociated sign of clinical instability’’ Day 9: Discharged and antibiotic stopped. Recommendations ℜ/ pneumococcal polysaccharide vaccination ℜ/ During next influenza season, influenza vaccination. ℜ/ ttt COPD & DM. FU CXR after 1 week.