Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
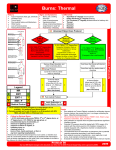
Initial Burn Care Lee D. Faucher, MD FACS Director UW Burn Center Professor of Surgery & Pediatrics Objectives • • • • Burn Care: From where we came Initial Burn Patient Evaluation Pediatric Considerations Burn Center Definition Objectives • • • • Burn Care: From where we came Initial Burn Patient Evaluation Pediatric Considerations Burn Center Definition September 11, 2001 • 8:20am – American Airlines Flight 77 Departed Washington Dulles at 8:20am – 58 passengers, crew of 6 • 9:38am – A 757-200 crashes into the Pentagon Washington Hospital Center • Located in Northwest DC – Areas largest trauma center and regional burn center Code Orange: This is not a drill! • Medical response – 8 trauma surgeons – 6 trauma residents – 7 intensivists and their teams – All others • Anesthesia, lab, blood bank, radiology, RT, security Patients begin to arrive • 3 patients in first 30 minutes – 1 smoke only, 2 burns • Then all air traffic grounded – 4 more by ground Patient Admissions Patient # Gender % TBSA Arrival 1 F 0 <1 hour 2 F 21 <1 hour 3 M 22 <1 hour 4 F 66 <1 hour 5 M 49 <1 hour 6 F 68 <1 hour 7 M 41 7 hours 8 M 42 10 hours 9 M 32 28 hours 10 M 10 31 hours Post-Burn Weeks 35 30 OR Hours # Operations 25 20 15 10 5 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Products consumed IV Fluids 141 Liters Silvadene cream Burn Dressing Gauze 4X4 gauze Kerlix gauze 950 Jars 2006 packs 18,490 3108 rolls Ace Bandages Allograft Synthetic “skin” 2111 26,700 sq cm 30,365 sq cm Autograft PRBCs 22,087 sq cm 269 units Outcomes Patient # Gender % TBSA 1 F 0 2 F 3 Age + TBSA Mortality Risk Outcome 32 N/A Survived 21 74 11 Survived M 22 61 4 Survived 4 F 66 115 62 Survived 5 M 49 100 41 Survived 6 F 68 109 44 Died 7 M 41 80 15 Survived 8 M 42 71 9 Survived 9 M 32 63 1 Survived 10 M 10 82 23 Survived Final numbers • 189 deaths – 125 in Pentagon – 64 on Flight 77 • 106 injured – 50 admitted to 9 area hospitals – 9 serious burns Objectives • • • • Burn Care: From where we came Initial Burn Patient Evaluation Pediatric Considerations Burn Center Definition Medics • Airway • Assess for other injuries • Start IV with LR, in burn OK – < 6 years = 125mL/hr – 6-13 years = 250mL/hr – >13 years = 500mL/hr • 100% O2 if closed space fire • Transport to closest hospital History • Source of burn • Enclosed space – Signs of smoke inhalation • Circumstances surrounding injury • Previous medical problems • First-aid done Reduction of CO 80 Room Air 100% Oxygen 3 ATM % CO 60 40 20 0 0 20 40 Time in Minutes 60 80 Medics - Electrical • Do not become victim – Turn off power • Initiate CPR – If < 1000 volt, ventricular fibrillation – If > 1000 volt, cardiac standstill and respiratory paralysis Medics - Chemical • • • • • Remove involved clothing Flush with water Flush with more water Then flush with more water When you think you are done, flush with more water • NO NEUTRALIZATION Cold • DOES NOT – Reverse temperature – Inhibit destruction – Prevent edema • DOES – Delay edema – Reduce pain Case presentation • EMS responds with Fire to structure fire with reported trapped occupants • On arrival, see two bystanders dragging person out the front door. Medic evaluation • Airway – Moving air, moaning, unresponsive, entire head, face, neck, and chest burned Medic evaluation • Breathing – Equal bilateral breath sounds • Circulation – Palpable distal pulses Medic evaluation • What else should be done at the scene? • Where should this patient be taken? Medic Report to ED • 47 y/o male, extricated from structure fire, burns over head, chest, back, bilateral upper extremities and legs, intubated with one peripheral IV in place running LR at 500mL/hr • Vitals: HR 130, BP 150/90, Sat 100% Emergency room treatment • • • • • • • Assess airway/breathing Ensure source of heat removed Estimate % TBSA Obtain/ensure adequate IV access Initiate/continue resuscitation Closely monitor urine output Keep patient warm Smoke inhalation assessment • Flame burns • Enclosed space • Burns to face, mucosal membranes • Singed eyelashes, nasal hairs • Carbonaceous sputum Emergency room treatment • • • • • • • Assess airway/breathing Ensure source of heat removed Estimate % TBSA Obtain/ensure adequate IV access Initiate/continue resuscitation Closely monitor urine output Keep patient warm Emergency room treatment • • • • • • • Assess airway/breathing Ensure source of heat removed Estimate % TBSA Obtain/ensure adequate IV access Initiate/continue resuscitation Closely monitor urine output Keep patient warm Rule of Nines Lund and Browder Chart Area 0-1 yr. Head 19 Neck 2 Ant. Thorax 13 Post. Thorax 13 R. Buttock 2½ L. Buttock 2½ Genitalia 1 R. U. Arm 4 L. U. Arm 4 R. L. Arm 3 L. L. Arm 3 R. Hand 2½ L. Hand 2½ R. Thigh 5½ L. Thigh 5½ R. Leg 5 L. Leg 5 R. Foot 3½ L. Foot 3½ 1-4 yr. 17 2 13 13 2½ 2½ 1 4 4 3 3 2½ 2½ 6½ 6½ 5 5 3½ 3½ 5-9 10-14 yr. yr. 13 11 2 2 13 13 13 13 2½ 2½ 2½ 2½ 1 1 4 4 4 4 3 3 3 3 2½ 2½ 2½ 2½ 8 8½ 8 8½ 5½ 6 5½ 6 3½ 3½ 3½ 3½ 15 Adult 2 3 Total yr. 9 7 2 2 13 13 13 13 2½ 2½ 2½ 2½ 1 1 4 4 4 4 3 3 3 3 2½ 2½ 2½ 2½ 9 9½ 9 9½ 6½ 7 6½ 7 3½ 3½ 3½ 3½ Total Emergency room treatment • • • • • • • Assess airway/breathing Ensure source of heat removed Estimate % TBSA Obtain/ensure adequate IV access Initiate/continue resuscitation Closely monitor urine output Keep patient warm IV access • • • • • < 15% TBSA – oral resuscitation 15 – 40% TBSA – one large bore IV > 40% -- two large bore IV’s IV’s should be in the upper extremities Suture IV’s started through burns Emergency room treatment • • • • • • • Assess airway/breathing Ensure source of heat removed Estimate % TBSA Obtain/ensure adequate IV access Initiate/continue resuscitation Closely monitor urine output Keep patient warm Crystalloid solution • Ringer’s Lactate – [Na+] 130 mEq (serum 140 mEq) – Osmolality 272 mOsm (serum 300mOsm) • Advantages of crystalloid – Effective in maintaining perfusion – Costs less than colloids – Can be mobilized with a diuretic Resuscitation first 24 hours • Baxter formula – 4 mL/kg/% TBSA burned • Give ½ the volume in first 8 hours and other ½ over next 16 hours. If < 20kg • Same Baxter formula for LR • Add 4mL/kg of D5 ¼ NS – Infuse at constant rate, increase LR if needed for adequate urine output Emergency room treatment • • • • • • • Assess airway/breathing Ensure source of heat removed Estimate % TBSA Obtain/ensure adequate IV access Initiate/continue resuscitation Closely monitor urine output Keep patient warm Monitor urine output • Place foley if > 20% TBSA • Urine output goal – 2 mL/kg/hr very young – 1 mL/kg/hr child – 0.5 mL/kg/hr adult • Diuretics are NEVER used to increase urine output • Increase urine output to > 100mL/hr if pigment present Emergency room treatment • • • • • • • Assess airway/breathing Ensure source of heat removed Estimate % TBSA Obtain/ensure adequate IV access Initiate/continue resuscitation Closely monitor urine output KEEP PATIENT WARM!!!!! Next priorities • • • • Insert NG tube Escharotomies Medications Wound care Next priorities • • • • Insert NG tube Escharotomies Medications Wound care Escharotomies • Only for leathery, circumferential, full-thickness burns • Rarely needed in transport < 12 hours • Almost always done at the Burn Center • Emergent indications: – Unable to ventilate – Pulseless, painful extremity Escharotomy pic Next priorities • • • • Insert NG tube Escharotomies Medications Wound care Medications • • • • • Pain control Pain control More pain control Tetanus immunization NEVER need antibiotics Next priorities • • • • Insert NG tube Escharotomies Medications Wound care Wound care • Debridement and topical application is usually done after transfer • Can cover with plastic wrap • Transport patient in DRY sheet and blanket • If transport delayed > 12 hours, – Debride loose tissue and clean with mild soap and water – Apply Silver Sulfadiazine and wrap loosely Resuscitation 24 - 48 hours • Continue maintenance fluids, watch serum Na+ • May use albumin or plasma for volume – Infuse 5 – 10mL/kg as needed • Maintain adequate urine output Objectives • • • • Burn Care: From where we came Initial Burn Patient Evaluation Pediatric consideration Burn Center Definition Burn Etiology ABA National Burn Repository, 2012 Report UWHC Admissions <18 years Admissions to Burn Centers ABA National Burn Repository, 2012 Report Percent Overall Burns and Mortality 40 35 30 25 20 15 10 5 0 0 to 2 5 to 16 2 to 5 Age Lived ABA National Burn Repository, 2012 Report Died 16-20 Overall Mortality and TBSA 100 Percent 80 60 40 20 0 0 to 10 10 to 20 20 to 30 30 to 40 40 to 50 50 to 60 60 to 70 70 to 80 80 to 90 TBSA 0 to 2 ABA National Burn Repository, 2012 Report 2 to 5 5 to 16 16 - 20 > 90 Where Childhood Burns Occur 10 2 8 Home Auto Recreation Other 80 ABA National Burn Repository, 2012 Report A kid with a small burn Why we do this • An acute burn may not be completely blistered • Can’t do wound care in clinic • Sedation easier when adequate pain control Appropriate wound care • Silicone • Foam • Silver What is Mepilex Ag Then what do we do • Dressing changed every 3 to 5 days • Our length of stay drastically reduced • Still same number of surgical procedures Objectives • • • • Burn Care: From where we came Initial Burn Patient Evaluation Pediatric Considerations Burn Center Definition Burn Center Referral • • • • • • All children Any burn > 10% TBSA Any full-thickness burn Burns to hands, face, feet or perineum Any Electrical or Chemical burns Other associated injuries, medical problems, or inhalation injury • Systemic disease Excerpted from Guidelines for the Operations of Burn Units (pp. 55-62), Resources for Optimal Care of the Injured Patient: 1999, Committee on Trauma, American College of Surgeons Outpatients Do Not include • • • • • Special locations Extremes of age Associated injuries Previous medical problems Unusual etiologies – Some chemical, some electrical • Unstable social situations Nurses Residents Physiatrists Pediatricians Burn Surgeons Nurse Practitioner Physical therapists Physician Assistant Child Life therapists Health psychologists Respiratory therapists Recreational therapists Occupational therapists Social Worker Pharmacists Nutritionists Administrators