Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
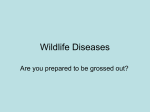
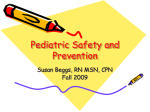
NEUROTOXICOSIS Bodnar R.Ya. PLAN NEUROTOXICOSIS Mercury poisoning Industrial uses. Pathogenesis of Mercury poisoning. Clinical picture. Diagnosis. Treatment. Tetraethyllead poisoning Industrial uses. Pathogenesis of Tetraethyllead poisoning. Clinical picture. Diagnosis. Treatment. Manganese poisoning Industrial uses. Pathogenesis of Manganese poisoning. Clinical picture. Diagnosis. Treatment. MERCURY POISONING MERCURY POISONING Mercury has been used commercially and medically for centuries. In the past it was a common constituent of many medications. It is still used in hospitals in thermometers and blood-pressure cuffs and commercially in batteries, switches, and fluorescent light bulbs. Large quantities of metallic mercury are employed as electrodes in the electrolytic production of chlorine and sodium hydroxide from saline. These uses still give rise to accidental and occupational exposures. MERCURY POISONING Today, however, exposure of the general population comes from three major sources: fish consumption, dental amalgams, and vaccines. Each has its own characteristic form of mercury and distinctive toxicologic profile and clinical symptoms. Dental amalgams emit mercury vapor that is inhaled and absorbed into the bloodstream. Dentists and anyone with an amalgam filling are exposed to this form of mercury. Liquid metallic mercury (quicksilver) still finds its way into homes, causing a risk of poisoning from the vapor and creating major cleanup costs. Humans are also exposed to two distinct but related organic forms, methyl mercury (CH3Hg+) and ethyl mercury (CH3CH2Hg+). MERCURY POISONING Fish are the main if not the only source of methyl mercury, since it is no longer used as a fungicide. In many countries, babies are exposed to ethyl mercury through vaccination, since this form is the active ingredient of the preservative thimerosal used in vaccines. Whereas removal of certain forms of mercury, such as that in blood-pressure cuffs, will not cause increased health risks, removal of each of the three major sources described in this article entails health risks and thus poses a dilemma to the health professional. MERCURY POISONING Exposure to mercury from dental amalgams and fish consumption has been a concern for decades, but the possible risk associated with thimerosal is a much newer concern. These fears have been heightened by a recent recommendation by the Environmental Protection Agency (EPA) that the allowable or safe daily intake of methyl mercury be reduced from 0.5 μg of mercury per kilogram of body weight per day, the threshold established by the World Health Organization in 1978, to 0.1 μg of mercury per kilogram per day. The Global Cycle of Mercury In nature, mercury vapor (Hg0), a stable monatomic gas, evaporates from the earth’s surface (both soil and water) and is emitted by volcanoes Anthropogenic sources include emissions from coal-burning power stations and municipal incinerators. After approximately one year, mercury vapor is converted to a soluble form (Hg2+) and returned to the earth in rainwater. It may be converted back to the vapor form both in soil and in water by microorganisms and reemitted into the atmosphere. Thus, mercury may recirculate for long periods. Mercury attached to aquatic sediments is subject to microbial conversion to methyl mercury (MeHg), whereupon it enters the aquatic food chain. It reaches its highest concentrations in long-lived predatory fish, such as sharks. The Global Cycle of Mercury Panel indicates the routes of transformation to methyl mercury as originally The Global Cycle of Mercury Panel depicts the increase in mercury concentrations in feathers of fish-eating birds in Sweden. The period covered by these data corresponds approximately to the growth of industrialization in Sweden. Acute MERCURY poisoning Acute mercury poisoning occurs rarely. It arises up after contact with large quantities of mercury. Acute MERCURY poisoning The main symptoms of the acute poisoning are hypersalivation, inflammation and formation of ulcers of mucous of the mouth, swelling of salivary glands, increase of submandibular lymph nodes, inflammation of gums, nausea, vomiting, diarrhea, tenesmus, intestinal colic. Acute MERCURY poisoning Necrotizing nephrosis with acute renal failure often develops. acute bronchitis, pneumonia. Very often liver, nervous system are affected. In blood: hemolysis, leukocytosis, increase of ESR (to 30-50 mm/h), increase of blood protein, nitrogen. Mercury poisoning Necrotizing nephrosis Acute MERCURY poisoning After the acute poisoning: a chronic diseases of kidneys, chronic colitis, hepatitis astheniс syndrome. After the treatment may be complete recovery. Chronis MERCURY poisoning Occurs after contact with mercury during 8-10 years. Clinical symptoms develop gradually and are characterized by affection of the NERVOUS SYSTEM. According to the degree of expressiveness of pathological process chronic poisoning is divided into 3 stages: INITIAL (FUNCTIONAL), MODERATE AND SEVERE. MERCURY POISONING DIAGNOSIS Early typical symptoms: irritability, weakness, Gingivitis stomatitis. Confirmation of diagnosis is mercury determination in urine and feces. Presence of mercury in urine without proper clinical symptoms indicates a “mercury carriage”. MERCURY POISONING Treatment -To destroy mercury and excrete it from organism antidotes are recommend: Unitiol, Sucsimer, sodium thiosulphate. - Most effective is Unitiol (sodium 2,3dymercaptopropansulfonat) - 5% 5-10 ml (0,05 g or 5% 1 ml per 10 kg of patient’s weight). 1 day - 2-4 injections, next 6-7 days –1 injection/ day. - Its sulfhydryl groups form untoxic complexes with poison and are excreted with urine. MERCURY POISONING Treatment Sodium thiosulphate 30% 5-10 ml i/v slowly. Drugs which improve metabolism and blood supply of brain (Pyracetam, Stugeron). Glucose 40% 20 ml + Vit. C, Vit.B 1, B 12, B 6. Tranquilizers. Symptomatic therapy. TETRAETHYLLEAD POISONING TETRAETHYLLEAD POISONING TEL is an oily transparent liquid which contains a 64,07 % of lead, well dissolves in organic solvents (ether, alcohol, benzol, petrol and other) and in fats. TETRAETHYLLEAD POISONING ТЕL is applied as antidetonate. A dangerous contact with TEL may occur -at its producing, - mixing with a fuel, - at cleaning of petrol cisterns. Tetraethyllead poison. is a strong neurotrop TETRAETHYLLEAD POISONING MODE OF ABSORPTION INHALATION SKIN INGESTION TETRAETHYLLEAD POISONING TYPE of POISONING ACUTE SUBACUTE CHRONIC TETRAETHYLLEAD POISONING Tetraethyllead Poisoning is characterized by neurological symptoms. Toxic affection of cerebral neurocytes ACUTE TETRAETHYLLEAD POISONING in 1-3 hours after a contact with ТЕL the first symptoms of the acute poisoning appear. According to the degree of expressiveness of clinical manifestations there are three STAGES of the acute poisoning by ТЕL: - INITIAL, - PRECULMINATION, - CULMINATION. CHRONIC TETRAETHYLLEAD POISONING is observed in workers who worked in contact with ТЕL during long period. A clinic develops gradually and can be poorly expressed. According to the degree of expressiveness of clinical manifestations there are three STAGES of the chronic poisoning: I-st (initial), II-nd III-rd. ACUTE TEL POISONING Treatment To wash up skin (with warm water and soap), to make gastric washing, to use absorbents. Patients with acute TEL poisoning need complete rest, hypnotic medicines from the group of barbituratus (phenobarbital, barbital sodium or etaminal sodium). At hyperexcitability barbamil (i/m or i/v) or hexenal are prescribed. hypertensive solution of glucose i/v, Vitamine therapy. Warm baths are recommended before sleep. CHRONIC TEL POISONING Treatment Treatment of patients with the chronic form of TEL poisoning is appointed taking into account expressiveness of clinical manifestations. For such patients - drugs which influence on a tissue metabolism (glutamine acid, glucose, vitamins C, B1, B2, ATF, riboxin), - tranquilizers (Diasepam, Tazepam) are recommended. MANGANESE POISONING Manganese poisoning The occupational manganese poisoning occurs among workers who work - on the manganese mines, - in metallurgical industry at steel making , -special alloys producing (ferromanganese – to 80 % of manganese, mirror cast-iron – to 15 % of manganese), - at making of electrodes and gumboils which are used for the electric welding, - in chemical and lacquer-paint industry, - in agriculture (stain of seed for stimulation of plant growth), - in rubber industry. - Most dangerous is ground and sifting of pound ore, because a lot of small disperse dust of manganese appear. VARIANTS OF CLINICAL COURSE Ways of Manganese poisoning Respiratory system Gastrointestinal tract Skin Manganese poisoning - The oxides of manganese are quickly absorbed. - In blood manganese circulates as an unsteady complex with plasma proteins. - Manganese is deposited in bones, cerebrum, parenchyma organs. - It is excreted from the organism with feces and urine. - Manganese may cause bronchial asthma and eczema because of its allergic influence. Manganese poisoning Pathogenesis Manganese, as a microelement, takes part in biological processes of organism. It influences on metabolic processes, depresses cholinesterase activity, affects metabolism of serotonin. At the protracted and systematic getting into the organism it has a direct influence on nervous tissue, and causes vascular violations, increase capillary permeability. It changes activity of enzymes of nervous cells, depresses the biosynthesis of catecholamines, intensifies protein metabolism. Manganese poisoning Pathogenesis The action of manganese is divided into two phases. I phase – cholinergic – is characterized by predominance of cholinergic influence. II phase – phase of areactivity – injury of acetylcholinoreactive structures. A manganese influences on the function of thyroid, cardiovascular system, gastrointestinal tract, liver and other. Acute Manganese poisoning In industry acute manganese poisoning occurs rarely. It arises up at breathing in large quantities of dust which contains manganese. Manganese poisoning causes severe disorders of blood circulation, dyspnea, frequent syncopes. In easy cases of poisoning irritation of the mucous of respiratory headache are observed. tracts, cough, and CHRONIC MANGANESE POISONING Clinical picture of the chronic manganese poisoning is characterized by three stages. !!! The special feature of clinical course of chronic manganese poisoning is inclination to its progress after stopping contact with a metal. MANGANESE POISONING DIAGNOSIS Special attention is paid to early diagnosis of chronic manganese poisoning. It’s necessary to find out a professional route, sanitary description of labor conditions (manganese concentration in the workplace, duration of contact during work day, experience of work, influence of other harmful professional factors), to analyse results of biochemical investigations (level of manganese in blood, urine, saliva, milk). MANGANESE POISONING A decline of patient activity, dormancy of psychical processes, insufficient critical relation to the state of organism predetermine the late appeal of patients for medical help. Handwriting in different stages of manganese poisoning MANGANESE POISONING Treatment Glucose 40 % + Vit.C (300-500 mg) i/v, vitamin B1 (40-50 mg), 0,25 % novocaine 10-15 ml (15-20 injections). At appearance of Parkinsonism signs it is necessary to prescribe antiparkinsonism cholinolytics (Cyklodol, Norakin, Amedin, Tropacin, tab. “Korbella”). Tropacinum – is effective antiparkinsonism cholinolytical drug (10-20 mg 1-2 times per a day after meal). “Karbella” decrease tremor and diminish tonus of muscles (1 tablet before sleep). MANGANESE POISONING Treatment medical gymnastics bath (36-37C, duration - 20 minutes, course of treatment - 10 baths) Application of ozocerite on spine (20-25 minutes 7-10 days)).