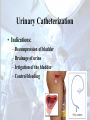
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
General Patient Care and Safety Objectives • Describe preoperative routines. • Identify, describe, and demonstrate the principles of transportation of the surgical patient. • Discuss, demonstrate, and apply the principles of surgical positioning. • Understand the methods of preparation of the operative site for surgery. Objectives • Describe the application of thermoregulatory devices. • Explain the principles and demonstrate the taking and recording vital signs. • Explain the principles of urinary catheterization and demonstrate the procedure. Objectives • Describe how the principles of the surgical skin prep and catheterization are related to patient care and asepsis. • Discuss methods of hemostasis and blood replacement, and demonstrate the use of appropriate agents or devices. • Discuss methods of documentation in the OR. Objectives • Identify developing emergency situations, initiate appropriate action, and assist in treatment of the patient. • Discuss the relationship between patient safety and the surgical environment. Preoperative Patient Routines • Prior to surgery, the patient must have certain information and tests performed. – – – – – – History and Physical Lab tests and results X-rays Preoperative checklist Special needs and allergies Consent • Surgical, Anesthetic, Blood products, Sterilization. Preoperative Education • Preoperative education is intended to: – Alleviate anxiety – Educate the patient about expectations before, during, and after the procedure. – Teach pre-op and post-op behaviors that may promote faster recovery. Admissions Procedure • Patient arrives evening before or morning of surgery. • Required paperwork completed. • Identification bracelet. • Vital signs • Patient changes clothes • IV’s are started • Preoperative medication • Transported to the Operating Room. Informed Consent • Patient must sign before any procedure. • Signing implies that patient has been informed of the procedure and any possible complications. • Patient may refuse or change their mind at any time. Informed Consent • Includes risks of surgery in general and risks for specific procedure. • Usually contains a clause specifying permission to perform further action, if during the operation, conditions arise to modify the procedure. • Anesthesia risks are stated. Informed Consent • Patient must sign before preoperative medication have been given. • If patient is unable to give consent, a spouse, legal parent or guardian, or 2 agreeing physicians. Informed Consent Informed Consent Patient Possessions • Patient is instructed to keep all valuables at home, but any remaining will be collected and given to family members or locked in a secure place. • Religious medals • Dentures, Glasses, Hearing aids • Wedding rings. Preoperative Routines • Pre-Op enemas may be indicated for certain Gastrointestinal or Gynecological procedures. • Nail polish should be removed as it will interfere with the pulse oximeter. • Preoperative showers are performed by the patient before surgery with antimicrobial soap. Preoperative Routines • Pre-Op sedation medications may be administered to help alleviate anxiety 1-2 hours before surgery. – Must have consent signed first. – Patient should not be left alone. – Safety devices such as safety strap and bed rails must be used. Preoperative Routines • Pre-Op shave if indicated will be performed by a nurse or nursing assistant in pre-op hold area. • Clippers (preferred) or razor will be used. • Take care not to nick or cut the skin. • Remove any loose hair so it will not end up on sterile field. Preoperative Routines • To prevent aspirations, patients will be placed NPO (nothing by mouth) at least 4-8 hours before surgery. – Nothing after midnight • May be modified if patient is to have local or spinal anesthesia. • Notify surgeon if patient consumed food or drink, procedure may be rescheduled. Preoperative Routines • Patients are instructed not to wear makeup, as it may contaminate sterile field and interfere with skin coloration. • Patients typically are required to remove all clothing and change into hospital gown. Preoperative Routines • When the operating room is ready, the patient will be asked to void if indicated. – Foley catheter will be placed after anesthesia • Patient ID checks and vital signs are taken just prior to transport. • Accompanied family are moved to waiting room and informed about approximate time and update process. Patient Transportation • Patients are taken to the OR in many ways. – – – – – Gurneys Ward beds Wheelchairs Walking Isolettes or cribs Patient Transportation • Ensure that proper safety devices and body mechanics are used at all times. – Rails, Safety straps, Wheel locks, etc. • Extra personnel available if needed. – Large patients, extra equipment. • Patients transported feet first. – Elevators head first. • Never leave patients unattended. Patient Transfer to OR Bed • Obtain correct number of personnel. – At least 2 for patients able to move themselves. – At least 4 for patients that are not able to move themselves. • Position gurney next to OR bed and lock the wheels. Patient Transfer to OR Bed • Instruct the patient not to move until you give the command. • Position personnel at the sides and ends of the gurney and brace themselves against it. – Take care to protect IV, Catheter, and Oxygen tubing, so they do not become entangled. Patient Transfer to OR Bed • Keep patient covered and assist them in moving over to the OR bed. – May use roller or draw sheet. • Apply the Safety Strap and remove gurney from the room. • Ensure comfort of the patient for induction. Patient Positioning • Goal is to provide best access and visualization of surgical site without causing physical harm to the patients joints, skin, or other body parts. • Must also provide for IV and anesthetic agent administration. Patient Positioning • Factors to consider when positioning: – – – – – Planned surgical procedure Surgical approach Conditions of the patient Age/Size Anesthetic Patient Positioning • Safety considerations when positioning: – – – – – – Ensure adequate personnel Provide for warmth and comfort Bed locks, safety straps. Do not move patient without permission. Arm not extended more than 90* Do not rest mayo stand and other equipment on the patient during the procedure. Patient Positioning • Supine position Supine Position – Patient flat on back with arms at side or on arm boards. – Pad all bony prominences. – Safety strap 2 inches above knees. – Used for procedures of the anterior surface of the body. • • • • Abdomen Chest/Breast Upper and anterior lower extremity Pelvis Patient Positioning • Trendelenburg/Reverse Trendelenburg Trendelenburg/Reverse Trendelenburg • Patient in modified supine. • Uses gravity to assist with procedure. • T-Berg – Pelvis and lower abdomen. • Reverse T-Berg – Upper abdomen and Head/neck. Patient Positioning • Fowler’s position Fowler’s Position • • • • Also known as “beach chair”. Modification to supine position. May be modified further to sitting position. Procedures involving: – – – – Breast Neck Shoulder Cranial Patient Positioning • Lithotomy position Lithotomy Position • Supine position with legs resting in stirrups. – Candy cane – Allen • Procedures involving: – – – – Perineum Anus and Rectum Vagina Urethra Patient Positioning • Prone position Prone Position • Patient is lying on “face down”. • Anesthesia and catheter insertion are performed on the gurney before patient is positioned. • Procedures involving: – – – – Posterior lower extremity Dorsal body surface Spine Posterior cranium Patient Positioning • Kraske/Jackknife position Kraske/Jackknife Position • Modification to prone position. • OR bed if flexed in the middle. • Procedures involving: – Anus – Pilonidal cyst Patient Positioning • Lateral position Lateral Position • Patient is placed on their side with affected side facing up. • Left lateral/Right lateral • Bottom leg flexed/Upper leg straight. • Axillary roll and double or universal arm board. • Procedures involving: – Retroperitoneal space, Hip, or Thorax Patient Positioning • Kidney position Kidney and Sims Position • Modified lateral positions. • Kidney – Used for kidney surgery – Table is flexed slightly • Sim’s – Used during colonoscopies Thermoregulation • Controlling the patients body temperature is important. • Patients lose much of their heat early on. – Moved into cooler OR – Little or no clothing – Wet skin preps • Hypothermia affects 60% of all surgical patients. Thermoregulation • Heat loss occurs from: – Radiation – Convection – Conduction – Evaporation • 80% of heat loss is thru radiation and convection. Thermoregulation • Hypothermia causes problem intra and post operatively. • Vasoconstriction leading to increased blood pressure. • Shivering increases oxygen demand. • Damage to surgical repairs. • Strain on cardiovascular and respiratory systems. Thermoregulation • Reduce heat loss by: – Raising room temperature initially. – Overhead heater – Warm solutions. – Warm blankets. • Water circulating blankets • Forced air warming blankets Vital Signs • Baseline vital signs are taken before the procedure. • Temperature, pulse, respirations, and blood pressure are monitored during the procedure. Temperature • Hypothalamus controls body temp. • Several factors affect body temp. – Environment, age, health, time of day. • Can be monitored: – Orally – Rectally – Axillary Pulse • 2 phases of the heart. – Systole – Diastole • Measured by health care provider by palpating an artery. • Radial (wrist) –Most common • Apical (Apex of heart) - Stethoscope Pulse Points in the Body Bradycardia <60 BPM / Tachycardia >100 BPM Respirations • Exchange of O2 and CO2. – Internal and External • Rate, rhythm, and depth are monitored by the health care provider. • Normal adult 12-20 per minute. Blood Pressure • Pressure of the blood against the walls of the blood vessels. • Expressed as 2 numbers – Systole – Contraction of heart – Diastole – Relaxation of heart Blood Pressure • Measured by inflating a cuff around the upper arm of the patient and listening to the brachial artery. • 5 Phases • Systolic BP is recorded upon hearing first heartbeat. • Diastolic BP is recorded when the heartbeat sounds disappear. Circulator’s Sterile Tasks • Among the various non sterile duties of a circulator, some tasks require the circulator to don sterile gloves. – Urinary Catheter Insertion – Surgical Skin Prep Open Gloving • Open glove wrapper on suitable surface, touching only the outer edges. • Pinch 1st glove at the cuff and pull onto hand. • Using the 1st gloved hand, scoop the 2nd glove behind the sterile cuff and pull onto other hand. • Make adjustments only touching the sterile area of the glove with other sterile parts of the glove. Open Gloving Open Gloving Open Gloving Urinary Catheterization • Introducing a flexible tube into the bladder via the urethra, to drain the bladder of urine. • Physician’s order in needed. • Performed under sterile conditions. Urinary Catheterization • Indications: – – – – Decompression of bladder Drainage of urine Irrigation of the bladder Control bleeding Urinary Catheterization • Considerations: – Sterile technique – Size, style, and materials • Indwelling • Latex allergy – Balloon filled with sterile water – Drains by gravity – Secure to patients thigh Urinary Catheterization • Surgical techs may be called upon to insert a urinary catheter. • Sizes 8-30 French (14-16 Most common) • Various materials and types • Males in supine, Females should be “frog legged” Urinary Catheterization • Procedure: – – – – – Gather supplies Open sterile catheter kit Don sterile gloves Drape the patient Prepare catheter • Test balloon • Lubricate tip Urinary Catheterization • Procedure: – Clean urethral meatus with antiseptic • Females retract labia • Males retract foreskin if indicated – – – – Keep “contaminated” hand on genitalia Insert catheter until urine is seen flowing Inflate balloon Hang drainage bag Surgical Skin Prep • Performed to remove transient organisms, and reduce resident organisms from the patients skin. • Similar to surgical hand scrub by sterile team members. • Skin cannot be sterilized!! Surgical Skin Prep Solutions • Alcohol – Provides rapid, significant reduction in microbes. Drying effect. • Iodine - Provides rapid, significant reduction in microbes. May irritate skin. • Iodophors – Less irritating to skin. • Chlorhexidine – Reduction effect is not as rapid, but longer lasting. • Hexachlorophene – Must be used several days prior to surgery. Build up effect. Surgical Skin Prep • Considerations: – All necessary procedures are carried out prior to skin prep. – Site must be free of gross contaminates. – Do not let prep solution accumulate under the patient. – Patient allergies – Area to be prepped Surgical Skin Prep • Procedure: – – – – Check patient allergies. Gather supplies. Expose surgical site and place chux pads. Aseptically open prep kit on appropriate surface. • Mayo stand or Prep stand Surgical Skin Prep • Procedure: – Ask permission from anesthesia to begin prep. – Don sterile gloves using open glove technique. – Check expiration dates on solution and pour onto appropriate sponges. • Scrub solution on scrub sponges • Prep solution on paint brushes sponges Surgical Skin Prep • Procedure: – If abdominal prep, begin with cleansing the umbilicus with cotton tipped applicator. – Take scrub sponge with scrub solution and begin washing at the surgical site moving outward in a circular pattern. • Moving from clean to dirty • Ensure that soiled sponges are not brought back over an area already prepped. Surgical Skin Prep • Procedure: – After all scrub sponges have been used, pat the area dry with sterile towels provided. • Be sure not to contaminate. – Take a paint brush sponge, and begin applying prep solution to the surgical site moving outward in a circular pattern, using the same rules as the scrub sponges. • Continue with all paint brush sponges. Surgical Skin Prep • Procedure: – Without contaminating remove chux pads, and allow the prepped area to air dry. • Tips: – Do not allow prep solution to pool. – If a sponge becomes contaminated, discard and start with a new sponge. Surgical Skin Prep • Abdominal Prep Surgical Skin Prep • Left Chest/Breast Prep Surgical Skin Prep • Lower Extremity Prep – May have a tourniquet applied. Surgical Skin Prep • Upper Extremity Preps – May have a tourniquet applied. Surgical Skin Prep • Perineum/Vaginal Preps – May include internal vaginal prep. Hemostatis • Hemostatis is the arrest of the loss of blood or hemorrhage. • Occurs: – – – – Naturally Mechanical methods Thermal methods Pharmacological methods Natural Hemostatis • Hemostatis is produced naturally by clot formation (Coagulation) and vessel spasm (Vasoconstriction). • Injured blood vessels releases a Prothrombin activator. • Thrombin, calcium, and fibrinogen work together to form a clot. – Platelet plug Factors Affecting Hemostatis • Congenital preexisting disorder – Hemophilia • Acquired disorders – Liver disease – Anticoagulant therapy • Heparin – Aplastic anemia – Aspirin therapy • Discontinue 1 week prior to surgery Mechanical Hemostatis • Clamps – Hemostats – Vascular Clamps • Ligature – Using suture to tie off a blood vessel – Stick tie • Clips – Small stainless steel or titanium used to occlude the vessel Mechanical Hemostatis • Sponges – Laps, Raytex, Cottonoids – Used to absorb blood and apply direct pressure to bleeding areas • Pledgets – Small squares of Teflon felt – Used as suture buttresses exerting pressure on needle holes to promote clotting Mechanical Hemostatis • Bone Wax – Refined and sterilized bee’s wax. – Mechanical barrier to seal off oozing blood from bone. • Suction – Used during surgery to clear the surgical site of blood and body fluids. – Variety of sterile tips for different surgeries. Mechanical Hemostatis • Drains – Used post operatively to remove blood and fluid from wound. • Tourniquets – Often used during extremity surgery to keep the operative site “blood free”. – Careful application is needed. – Must be periodically deflated for longer surgeries. Thermal Hemostatis • Electrosurgery • Monopolar – Active electrode (Sterile) – Dispersive electrode (Grounding Pad) (Unsterile) • Bipolar – Forcep like tip – Does not require placing a grounding pad Thermal Hemostatis • Laser – Intense concentrated beam of light. – Able to cut and coagulate tissue with very little surrounding damage. – Follow all safety protocols when working with a laser. Pharmacological Hemostatis • Absorbable gelatin (Gelfoam) – Composed of collagen in pad or powder form. – Deposits fibrin over bleeding area. • Collagen (Avitene) – Absorbable powdery substance of 100% collagen. – Forms sticky fibrin material. Pharmacological Hemostatis • Oxidized Cellulose (Surgi-Cel) – Creates a rapid forming blood clot applied directly to the bleeding surface. • Silver Nitrate – Used to control cervical or nasal bleeding. • Epinephrine – Vasoconstrictor – Used with local anesthetics and Gelfoam. Pharmacological Hemostatis • Thrombin – Bovine origin blood clotting enzyme – May be used directly onto bleeding area, or used in combination with Gelfoam. Blood Loss • Blood loss intraoperatively is monitored by several methods: – Suction containers • STSR must keep track of amount of irrigation fluid used. – Weigh soiled sponges • If blood loss is determined to be significant, a transfusion may be ordered. Blood Transfusions • Blood typing and cross matching are needed to ensure proper match. • 4 types – A, B, AB, and O – RH + or RH – • Careful checks are completed before blood is given to patient to avoid hemolytic reaction. Blood Transfusions • Whole blood or blood products may be indicated. – Plasma – Packed Red Blood Cells – Platelets • Homologous (Donated) • Autologous (Stored patient blood) – Cell Saver machine Emergency Situations • The STSR must be able to anticipate emergency situations and prepare in advance. • This skill comes with time, but entry level techs must be able to recognize basic signs. • The STSR must be able to react in a quick and calm fashion. Emergency Situations • Indicators of emergency situations: – – – – – – Rapidly dropping blood pressure Cardiac dysrhythmia Changes in vital signs Chest pain/difficulty in breathing Changes in skin color/temperature Confusion/Disorientation Emergency Situations • Treatment includes – Ensure a patent airway and restore breathing. – Maintain or restore cardiovascular status. – Treat injuries: • Chest • Shock • Wound closure • Fractures • Vital sign monitoring • Reassurance and comfort for patient Emergency Situations • CPR – All healthcare providers must be familiar with this lifesaving technique. – Certification by AHA or Red Cross • Recert every 2 years – – – – A = Airway open B = Breathing C = Circulation D = Definitive treatment Emergency Situations • CPR in the O.R. – Primary responsibility of the STSR is to remain sterile and protect the sterile field. – Keep track of instruments and needles. – May be asked to do open chest massage. – Sterility may become secondary. Emergency Situations • Malignant Hyperthermia – Life-threatening, acute pharmagogenetic disorder, triggered by an anesthetic agent. – Rapid increase in body temperature – Unexplained tachycardia – Unstable BP – Muscle rigidity – May lead to renal failure, heart failure, or death. Emergency Situations • Malignant Hyperthermia Prevention – When patients have a predisposition to MH, nontriggering anesthetic agents are used. • Propofol • Vecuronium – Vaporizer, filter, circuit hoses are changed and/or flushed with oxygen to ensure removal. – Careful monitoring by anesthesia provider. Emergency Situations • Malignant Hyperthermia Treatment – Stop the triggering agent immediately – Surgery may be stopped ASAP • STSR must be ready for quick closure – Various cooling methods may be used. • Chilled peritoneal lavage • Packing patient in ice • Dantrolene is administered. Emergency Situations • Syncope – Sudden loss of consciousness – Caused by several factors: • Disorders of arterioventricular conduction • Ventricular asystole or fibrillation • Bradycardia – Notify physician – Protect from aspiration – Treat injuries Emergency Situations • Seizures – Grand Mal (Most common) • • • • • Loss of consciousness Convulsions Incontinence Pre seizure warning signs May have no memory afterwards – Petit Mal • Shorter in duration Emergency Situations • Seizures – Focal • Arise from motor and sensory nerves in brain. • Occur in patients with brain tumors and arteriovenous malformations. • Following all seizures patients may feel fatigued and may have no memory of the event. Emergency Situations • Seizure management – Primary duty of STSR is to protect the patient. – Maintain an airway • Aspiration risk • Mouth clenching – After seizure calm and reassure the patient. – Document Emergency Situations • Anaphylactic reaction – Exaggerated allergic reaction to a substance. • Local anesthetics • Contrast media • Latex – First signs are usually mild itching and swelling. – Leads to difficulty breathing due to bronchospasm and laryngeal edema. Emergency Situations • Anaphylactic treatment – Maintain airway and provide oxygen. – Myocardial infarction is possible. – Treat for possible shock. – Give epinephrine to reduce spasm and raise blood pressure. – Levophed to increase blood pressure • Key is to act quickly and be sure to check for any allergies before giving medications, etc. Review and Summary • • • • • • • • Preoperative routines / Consent Patient transportation and positioning Vital signs Open gloving Urinary catheterization Surgical skin prep Hemostatis Emergency situations