Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
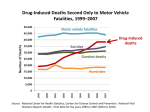
Carbon Monoxide Poisoning Joshua Rocker, MD Pediatric Emergency Medicine Schneider Children’s Hospital The Basics • CO is an odorless, tasteless, colorless, non-irritating gas formed by organic (hydrocarbon) combustion The Basics • CO binds hemoglobin with a much greater affinity then O2 (200-250x) forming carboxyhemoglobin (COHb) Sources • • • • • • Motor Vehicle Exhaust Smoke from fires Gas powered equipment Non-electric heaters (kerosene, gas water) Charcoal or Hibachi grills Spray paint, solvents, methylene chloride, degreasers and paint removers Risks for exposure • • • • • • Riding in back of pickup trucks Swimming behind motor boat Industrial workers where combustion occurs Personnel at fire scenes Using combustion engines indoors Using non-electric heating devices without proper ventilation Epidemiology • 40,000 ER visits per year • 5,000-6,000 deaths per year • Accidental CO poisoning only responsible for approximately 500 deaths annually • Leading cause of accidental poisoning deaths in America Recent Trend Data from the CDC All U.S.A. Deaths from CO Poisoning, 1979 – 1988 • Highest death rates among: males, blacks, the elderly, and residents of northern states • Motor vehicle exhaust caused 57% of unintentional deaths • 83% of deaths associated with stationary automobiles Cobb, N. & R.A. Etzel. (1991) Unintentional carbon monoxide-related deaths in the United States, 1979 through 1988. JAMA, 266, 659-663. Age Distribution of cases • <6 y/o- approximately 14% • 6-19 y/o- approximately 16% • >19 y/o- approximately 70% Data for 1996 and 1997 from the Annual Report of the Am. Assoc. of Poison Control Centers, Toxic Exposure Surveillance System (published in the American J. Emergency Medicine). Symptoms Symptoms • Variable and nonspecific • Cherry red lips or skin • associated with high COHb, but rare (2-3%) and insensitive Symptoms Fatigue Headache Frequency (%) 92 87 Dizziness 69 Sleep Disturbances Cardiac Symptoms Apathy Nausea, vomiting 66 62 54 42 Memory Loss Decreased Libido Loss of Appetite 40 22 12 Symptoms • Older child and adult symptoms are similar • Symptoms of infant or young child may be more vague and difficult to clarify • Irritability, poor feeding Symptoms loosely associated with COHb level Children Specific • In theory children at higher risk of toxicity • higher metabolic rate • higher tissue oxygen demand • Infants with high F-Hgb or other forms of anemias may be at higher risk of deleterious effects • Higher rate of lethargy and syncopy in children at lower levels of COHb than expected (Crocker,William: J Emerg Med, 1985.) Be careful: Misdiagnoses • • • • • • • Flu, viral syndrome AGE Migraine Stroke Alcohol Related Behavior Psychiatric Disorder CAD Delayed Neuropsychiatric Syndrome (DNS) • Seen in up to 40% of those with significant exposure • Onset- 3-240 days after exposure • Variable degrees of cognitive deficits, personality changes, movement disorders or focal neurological deficits • In children may b/w difficulty in school • May persist for years DNS • Cannot be reliably predicted • Increased risk if patient presented with LOC during acute phase Pathophysiology Pathophysiology • Effects • Oxygen delivery • Total oxygen delivery diminished • Oxygen utilization • Asphyxia Pathophysiology • CO rapidly diffuses across pulmonary capillary membrane and binds hemoglobin forming COHb • Once COHb is formed an allosteric change occurs and the hemoglobin protein’s ability to off-load the other 3 O2 is greatly diminished TOTAL OXYGEN CONTENT DIMINSHED Oxyhemoglobin dissociation curve: Left shift Left shift- ↓ P50 ↑ affinity (↑ pH, ↓DPG, ↓temp, CO, met-hgb,F-hgb) Right shift- ↑ P50 ↓ affinity Pathophysiology • CO also interferes with peripheral O2 utilization by impairing oxidative phosphorylation in the mitochondria ASPHYXIA But… • neither the transient hypoxemia nor the transient asphyxia explains the symptoms in full- especially the DNS. Neuropathopysiology • CO binds to cytochrome oxidase which caused oxidative stress • NO is released from platelets and endothelial cells • Form free radical peroxynitrite • Damages the neural vascular endothelium • END RESULT: lipid peroxidation of the brain occurs during recovery Lipid Peroxidation • With perfusion of brain- leukocytes adhesion and subsequent release of destructive enzymes • Excitatory AA exacerbation oxidative injury Neuropathophysiology • CO has predilection for the basal ganglia • Explain movement abnormalities • Autopsy results show involvement of: cerebral cortex, hippocampus, cerebellum and substantia nigra • Explain the diverse neurological abnormalities Laboratory evaluation • VBG/ABG, COHb, CPK, CBC, lytes and EKG • Consider: tox screen, EtOH level and cardiac enzymes COHb • Normal levels • Non-smokers: 0-3 • Smokers: 3-5 (can be up to 10) • Elevation does not always directly translate to more symptoms or worse prognosis Management Management #1- GET OUT!!!!!! Management • 1- Remove oneself from source of CO • 2- Seek medical attention • In ambulance- 100% non-rebreather (NRB) • In hospital- always …ABCs Management • 3. 100% NRB • Half-life of COHb is 4-5 hours at RA • Half-life is 40-80 minutes with NRB • (Normobaric oxygen therapy- NBO) Management • 4. Hyperbaric Therapy • Delivery 100% O2 at 2.5-3 atms of pressure • Alters the half life of COHb to less than 30 minutes. Hyperbaric Therapy: • Henry’s Law • amount of an ideal gas dissolved in a solution is directly proportional to its partial pressure. • Dissolved Plasma Oxygen Content: • RA @ 1 atm- 0.3 ml/dl • 100% O2 @ 1 atm- 1.5 ml/dl • 100% O2 @ 3 atm- 6 ml/dl • Sufficient to meet resting O2 demands regardless of hgb-O2 supply HBO • Single place vs multi-place chambers • Raise pressure to 2.5-3 atms • Length of tx- 45-300 minutes • Concerns: • Can child tolerate alone- if single • Deterioration in chamber- can’t open immediately HBO • Complications: • 20%- reversible myopia • 3-20%- otic barotrauma • pulmonary barotrauma • pulmonary oxygen toxicity • seizures HBO • Absolute contraindications: • Untreated pneumothorax • Relative contraindications • URI, sinus disease, claustrophobia • Hx of seizure d/o, pneumothorax or chest surgery HBO: how does it work?? • Decreasing the occurrence of DNS does not seem to be solely based on the COHb elimination but rather on the reduction of free radical production and lipid peroxidation. HBO: how does it work • Thom, SR: Antagonism of CO-mediated brain lipid peroxidation by HBO. Toxicol Appl Pharmacol, 1990, 105: 340-344. • Animal study which revealed that HBOT accelerated the elimination of CO from bound cytochrome oxidase, therefore preventing oxidative brain injury. HBO: how about in kids? • Rudge: CO poisoning in infants. South Med J 1993, 86: 334-337 • Complete neurological recovery in 13 of 14 children < 2 y/o receiving HBO • Crocker and Walker: Pediatric CO toxicity. J Emerg Med 1985, 3: 443-448. • No m and m among 16 children who received HBO vs 25% developed DNS in those receiving NBO. • Kim and Coe: Clinical study on CO intoxication in children. Yonsei Med J 1987, 28:266-273. • 29.4% vs 19.4% (NBO vs HBO) with neurological sequelae •BUT… HBO: controversy • Tibbles and Perrotta: Treatment of Carbon Monoxide poisoning: a critical review of human outcome studies comparing NBO with HBO. Ann Emerg Med, 1994. • "no randomized, controlled, blinded clinical trial demonstrated a clear advantage of HBO over NBO in reducing morbidity and mortality in carbon monoxide poisoning." Criteria for HBO: Although controversial, these are general accepted • • • • • • • Syncopy Acutely severe neurological symptoms MI Cardiac Dysrhythmias Persistent neuro symptoms Pregnancy if >COHb15 Severe acidemia Criteria to consider HBO • COHb >20-25% • <6 months with symptoms • Children with underlying disease for whom hypoxia may be deleterious • > 60 y/o Further Management • Treat other issues… • Hypotension- 2º to myocardial damage • Hypoglycemia • Cardiac Ischemia • Smoke inhalation injuries • Burns • Seizures • Rhabdomyolysis Prevention • Careful behavior • Proper ventilation • CO monitors • “To protect against carbon monoxiderelated deaths, New York State implemented a new law requiring carbon monoxide detectors in all one- and twofamily houses, condominiums and co-ops built on or after December 1, 2002.” New York City Department of Health and Mental Hygiene Miscellaneous • Pulse oximetry may read normal or even over-estimate the arterial hemoglobin oxygen saturation Hampson, NB. Pulse oximetry in severe carbon monoxide poisoning. Chest, 1998; 114:1036-1041 Questions A family of 5 presents to the ER. The 5 and 7 years old children present with headaches and abdominal pain. The 6 month old is refusing feeds and is having diarrhea. Their vitals are WNL. The mother passed out at home. What should you do first? • A. Call Jacobi and see if they will receive these patients • B. Call 1-800-POISONS • C. Obtain COHb levels on all the children • D. Put 100% NRB on the older children and give 20cc/kg NS bolus to the youngest • E. Place all the children on 100% NRB • ABCs • 100% NRB to all • Secondary survey may reveal a dehydrated child which can be addressed but it is secondary. • HBO may be necessary but institute first line therapy first. • Yes, draw the levels- after O2. A 9 yr old girl is brought to the ER because she is lethargic. The mother returned home to find her minimally responsive. The mother suffers from chronic lower back pain and has medications in the home. The child is on winter vacation from school. There home is heated with an old coal furnace. On exam she is obtunded. Her vitals are: 36.8 C, HR 100, RR-8, BP- 80/40. O2 sat is- 95%. With 100% NRB her sats increase to 100%. Her skin is normal color. Her lungs are clear. Her pupils are miotic. What is the most likely confirmatory study? • • • • • A. CXR B. Methemoglobin level C. COHb level D. Urine tox E. LP • CXR • no respiratory distress only depression • Methgb • toxin-induced from ingestion or dermal exposure to an oxidizing agent • aniline • dapsone, • local anesthetics • phenazopyridine • nitrates/nitrites • naphthalene • Genetic • dietary (eg, well water nitrates), • idiopathic causes (acidosis). • Patients usually present with cyanosis not responsive to oxygen administration. • COHb • Right season • right risk factors- indoor furnace • right symptom- obtunded, but… miotic, hypotensive and experiencing respiratory depression. Still treat and w/u. • Urine tox • Where the money is. Mom with meds at home and patient with signs of opiate tox. • LP • No fever, respiratory and BP involved. Unlikely, but if else negative encephilitis is possiblity. QUESTIONS???