Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Infection control wikipedia , lookup
Reproductive health wikipedia , lookup
Birth control wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Dental emergency wikipedia , lookup
Prenatal testing wikipedia , lookup
Menstruation wikipedia , lookup
Menstrual cycle wikipedia , lookup
Maternal physiological changes in pregnancy wikipedia , lookup
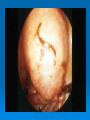
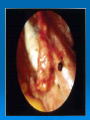
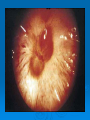
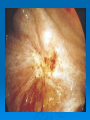
MCCQE Review: Gynecology Dr. Jessica Dy Division of Reproductive Medicine Department of Obstetrics and Gynecology Overview Objectives of MCCQE in Gynecology Selected Topics: Part 1 Sexual Development Menstrual Abnormalities (amenorrhea, PCO, abnormal bleeding patterns) Contraception Intermission Overview Selected Topics: Part 2 Pelvic Pain Pelvic Mass Infertility Pelvic Relaxation/Prolapse Intermission Overview Selected Topics: Part 3 PAP Smears Gynecologic Infections(Graphic) Ectopic Pregnancies Domestic Violence End – Good Luck on your examination MCCQE Objectives: Gynecology: Breast Disorders Infertility/Impotence/Sexual Dysfunction Menstrual Cycle Abnormal/Amenorrhea/Pre-menstrual Syndrome Menopause PAP Smear/Screening/Prevention Pelvic Mass Pelvic Pain Contraception/Pregnancy Prevention/Termination Prolapse/Pelvic Relaxation Vaginal Bleeding,Excessive/Irregular/Painful/Dysmenorrhea Vaginal Discharge/Urinary Symptoms, Vulvar Lesions, STDs Violence, Family (Child,Elderly,Adult,Spouse,Rape,Violence Against Women) Italic = covered under other specialities MCCQE Objectives: Full Clinical Presentation List: Sexual Maturation(normal,abnormal) Part 1 Female Sexual Development “Baby Has Gone Mad!” Breast Development (Thelarche) 10.5 yo Hair Development (Pubarche) 11.0 yo Growth (peak height velocity) 11.4 yo Menstruation (Menarche) 12.8yo Note growth spurt superimposed on pubertal process -begins prior to thelarche Female Sexual Development In General: -low levels of FSH and LH are found in infants and prepubertal girls - prior to onset of pubertal changes, levels of FSH and LH rise (initially at night-LH) - estradiol levels rise and breast development occurs, eventually sufficient estrogen is available to initiates endometrial growth and menses -andrenache(pubarche) biologically unrelated event, but temporally related to other pubertal changes Female Sexual Development: Precocious Puberty (development of secondary sexual characteristics before 8yo) Types: 1) GnRH Dependent(True Precocious Puberty) -early activation of hypothalamic-pituitary-ovarian axis 2) GnRH Independent(Precocious Pseudopuberty) - sexual maturation not related to GnRH secretion (eg.extra pituitary secretion of gonadotropins, or sex steroid secretion) Female Sexual Development: Precocious Puberty Causes: 1) GnRH Dependent Idiopathic CNS problem 74% 7% (tumors, encephalitis, menigitis, hydrocephalus, skull injury/deformity) 2) GnRH Independent Ovarian(cyst or tumor) 11% McCune-Albright syndrome 5% (autonamous early production of E2 by ovaries, cycstic bone lesions-#’s, café au lait) Adrenal 2% Ectopic FSH/LH 0.5% Hypothyroidism ? Female Sexual Development: Precocious Puberty Investigations: initial:- bone age, height and wieght - estradiol levels(precocious breast development) - androgens- DHEAS, Testosterone(precocious andrenarche) - FSH,LH,TSH levels secondary: - imaging of pituitary/sella - ultrasound ovaries, uterus, image adrenals - bone scan(McCune-Albright) Female Sexual Development: Precocious Puberty: Findings Cause 1) GnRH Dependent FSH/LH Estradoil DHAS Gonadal Size Idiopathic CNS problem Increased Increased Increased Increased Normal Normal Increased Increased Decreased Decreased Decreased Increased Increased Increased Increased Increased Normal Normal Increased Normal Uni. Increased Increased Small Increased 2) GnRH Independent Ovarian(cyst or tumor) McCune-Albright syndrome Adrenal Ectopic FSH/LH Bone age is advanced compared to chronological age in all causes, except hypothyroidism.(unknown reason) Female Sexual Development: Precocious Puberty Treatment: Aimed at underlying process Tumor-resect,radiation,chemo Idiopathic- GnRH agonist therapy McCune-Albright- MPA - Testolactone-aromatase inhibitor Delayed Puberty- discussed as primary amenorrhea Suggested sites for more information http://www.utdol.com and search precocious puberty http://www.utdol.com/application/topic.asp?r=/application/topic.asp&file=r_endo_m/9737&type=A&selectedTitle=1~25&app=utdol Amenorrhea Definition: Primary Amenorrhea - no period by age 14 in absence of growth or development of secondary sex characteristics - or no period by age 16 regardless of presence of normal growth and development with the appearance of secondary sex characteristics Amenorrhea Definition: Secondary Amenorrhea - in a woman who has been menstruating, the absence of periods for a length of time equivalent to a total of at least 3 of the previous cycle intervals, or 6 months of amenorrhea Amenorrhea Etiology: Pregnancy Thyroid disease Prolactin disease PCO and its variants Hypothalamic disease Ovarian failure(resistance) Endometrial failure Developmental, genetic disorders Amenorrhea -Hypothalamic Stress induced anorexia nervosa – loss of pulsatile GnRH secretion - 15% below body weight starts to return -exercise induced -critical body fat threshold -centrally acting agents (melatonin, opiods, and CRH increase) Amenorrhea -Hypothalamic Overall: When available energy is excessively diverted or insufficient, reproduction is suspended in order to support essential metabolism for survival. Diagnosis of exclusion Amenorrhea -Pituitary Pituitary Adenomas: non-functioning – most common (30-40% of all pituitary) prolactinoma growth hormone secreting - acromegaly ACTH secreting - Cushing’s Disease Amenorrhea -Pituitary Adenomas Overall: Elevated levels of prolactin cause decrease secretion of GnRH from hypothalamus, therefore decreased FSH/LH and amenorrhea (hypothalamic amenorrhea) Any mass lesion may cause stalk compression (-relieves prolactin from Dopamine suppression therefore can cause hyperprolactinemia) Amenorrhea Rare Pituitary Lesions Sarcoidosis Tuberculosis Teratomas Crayniophyphyrangieoma Lymphocytic hypophysitis Sheehan’s Syndrome Post partum hemorrhage with ischemic necrosis of anterior pituitary (portal system) -failure of lactation Amenorrhea -Ovary Anovulatory – PCO – condition where ovaries contain multiple early stage follicles which do not mature secrete androgens in excess of E2 -related problems with insulin receptor function and lipids, hyperandrogenism and unopposed estrogen Ovarian failure – premature exhaustion of follicles < 40 years -radiation, chemotherapy, genetic, iatrogenic, idiopathic Amenorrhea -Ovarian Abnormal Development Dysgenetic Gonads (Abnormal chromosome complement) - Turner’s Syndrome +/- mosiacisms – 45X - XY Swyer’s syndrome testes develop abnormality or failed to develop no testosterone effect but AMH testis streaks-fibrous bands - Testicular ferminization also a Mullarian abnormality defect is one of a spectrum of androgen insensitivities Amenorrhea -Ovarian Abnormal Development Dygenesis of Gonad XX -accelerated germ cell loss with premature degeneration of ovaries Amenorrhea -Genital Tract Blockage (mullarian abnormalities) - transverse septum - imperforate hymen - non-communicating cavities Endometrial Failure – Asherman’s syndrome - secondary to vigorous D&C – usually postpartum - ++ adhesions/synechia in uterine cavity To Test: give both E2 then P4 and withdrawal if period then outflow tract not obstructed &/- failure Amenorrhea BHCG TSH Prolactin hypothyroid pregnancy hyperprolactinemia Within Normal Limits Progesterone Challenge -Provera 10mg x 10d Bleeding No Bleeding Anovulation Estrogen & Progesterone Bleeding No Bleeding End Organ Problem -obstruction -failure FSH and LH High Ovarian Failure Normal or Low CT Scan of Sella -Sellar lesion -hypothalamic amenorrhea Approach to Amenorrhea If Prolactin elevated- investigate for hyperprolactinemia If pregnant stop investigating Approach to Amenorrhea 2 Approach to Amenorrhea 3 Approach to Amenorrhea 4 Approach to Amenorrhea 5 Approach to Amenorrhea 6 Approach to Amenorrhea 7 Including: Dysgenetic Gonad Gonadal Dysgenesis -therefore do Karyotype Approach to Amenorrhea 8 Abnormal Hypothamic,or pituitary lesion Normal PCOS PCOS – Polycystic Ovarian Syndrome described in 1935 by two gynecologists- Stein and Leventhal large polycystic ovaries with amenorrhea Triad of: amenorrhea obesity hirsutism PCOS -Clinically -biochemistry – LH/FSH ratio >2-3 and elevated androgens (increased testosterone, DHEAS, 17-OH progesterone) -U/S - multiple follicles peripherally arranged (string of pearls appearance) - not specific 8-25% of normally cycling women will have this appearance -~14% of women on the pill will have this appearance -recently appreciated to be a spectrum of disease severity/presentations What is PCOS -a syndrome resulting from chronic anovulation -can be associated with high insulin levels in many patients -diagnosis is made clinically +/- biochemical support -evidence of oligo/anovulation -evidence of androgen excess -+/- evidence of insulin resistance Why is this Important? 1. 2. 3. 4. 5. 6. Infertility Menstrual bleeding problems – amenorrhea – DUB Hirsutism, acne and alopecia Increased risk of endometrial cancer Increased risk of CAD Increased risk of type II diabetes if insulin resistant Insulin Story Defect in insulin receptor - altered phosphorylation at serine (increased) and tyrosine (decreased) residues on insulin receptor - this reduces signal transmission and causes a post receptor problem and glucose transport decreases - this phosphorylation of serine may increase the activity of enzymes that make androgens in both the ovaries and adrenals Insulin Story: Net Result – increased insulin levels secondary to decreased tissue uptake of glucose - increased androgen production from both adrenals and ovaries (LH and insulin act synergistically to increase androgen production by theca cells in ovary). Treatment Treatment depends on patient’s immediate concerns and risk factors -weight loss through diet and exercise -treatment with progesterone to prevent endometrial hyperplasia – cancer -Metformin to decrease insulin levels ? reduce risk of progression to type II diabetes ? improve lipid profiles · ? induce ovulation sensitize to ovulation induction Treatment Ovulation induction Clomiphene SERMS (letrozole/tamoxifen) FSH ovulation induction Ovarian drilling Abnormal Uterine Bleeding (Unrelated to Pregnancy) Menorrhagia: cyclic menstrual bleeding occurring at regular intervals excessive amount and/or duration (>80 ml menstrual fluid/>7 days) Metrorrhagia: uterine bleeding occurring at irregular intervals Menometrorrhagia: uterine bleeding irregular frequency and excessive in amount Abnormal Bleeding Causes of “Organic” Abnormal Uterine Bleeding: uterine -polyps, -fibroids -trauma -infections-PID, endometritis, -IUD -exogenous hormones -endometrial cancer, hyperplasia -cervical cancer, infection other -vulvovaginitis -vaginal,vulvar,ovarian cancer -coagulation disorders -thyroid disease Abnormal Bleeding Dysfunctional Uterine Bleeding(DUB): Uterine bleeding without any evidence of organic disease(ie no polyps, malignancy, pregnancy, etc.) 90% related to anovulation 10% can be ovulatory Anovulatory DUB -no ovulation, therefore no progesterone secretion -endometrium exposed to prolonged and unopposed estrogen resulting in estrogen breakthrough bleeding (fragile, un-uniform growth of endometrium-areas of shedding and re-growth) Abnormal Bleeding Ovulatory DUB(uncommon) - ? Luteal phase progesterone unable to maintain endometrium Abnormal Bleeding Investigations: -Bhcg -CBC -R/O organic diseases -hx & px -endometrial biopsy -+/- ultrasound Treatment dependent on Cause Abnormal Bleeding DUB Treatment: Mild: OCP 1 tab tid then continuous x 4-6 months OR cyclic provera 5-10 mg po od x10d monthly Severe: stabilize patient as required premarin IV 25 mg q4-6h +/- add OCP or provera OR D&C if severely ill or unresponsive to medical Tx Abnormal Bleeding DUB Longterm Treatment: OCP cyclic provera 5-10 mg po od x10d monthly progestin only pill progesterone IUD NSAIDS-menorrhagia anti-fibrinolytic agents- menorrhagia surgical - endometrial ablation, hysterectomy Contraception 27 yo nulligravid medical student was “celebrating” with her male partner (Chiropractic student) after she had successfully passed the MCCQE part 1. Her LMP was 14 days ago and she has regular 28 day cycles with the molimina. Immediately after intercourse she noticed his condom was no longer on his penis and exclaimed “Oh my, your condom must have fallen off and must still be in my vagina !”. He then replied “Condom, what condom?”. What would be the appropriate medical management(s) to offer this couple? (You may chose up to three answers) Contraception A) Urgent pregnancy test (serum) B) Menstrual Extraction in office C) Suggest expectant management with possible therapeutic abortion if required D) 2 ovral tablets po q12h x 2 doses E) MTX 50 mg/m2 IM x1 F) Insertion of copper containing IUD G) 0.75 mg Levonorgestrel po q12h x 2doses H) Suggest partner to perform ‘spinal manipulation’ to delay endometrial growth and prevent implantation Contraception Yuzpe Method ‘Morning After Pill’ within 72 hours of intercourse 2 ovral tablets q12 x 2 doses (often combined with Gravol 50mg) 6% chance of pregnancy per single act of intercourse Yuzpe method decreases to 2% Contraception Levonorgestrel within 72 hours of intercourse 0.75mg levonorgestrel q12 x 2 doses (less nausea) slightly improved efficacy to Yuzpe ~1% Contraception Copper IUD Insertion within 5 days of intercourse 0.1% failure rate Ideally used in patients with no contraindications to IUD pregnancy undiagnosed vaginal bleeding pelvic infection suspected gynecologic malignancy copper allergy/Wilson’s disease (previous ectopics, mullerian abnormalities, valvular HD) Contraception OCP Contraindications: pregnancy undiagnosed vaginal bleeding active liver disease (hepatoma) previous or active thromboembolic disease estrogen sensitive cancer age >35 smoker uncontrolled hypertension Contraception Method Typical use (%preg/y) Perfect use (%preg/y) Chance Withdrawal Condom Condom + spermicide Female condom Diaphragm IUD-Copper 85 85% 19 4 12 3 5 (Toronto notes) 21 5 18 6 0.8-2.0 * 0.6-1.5 * different from Toronto Notes(3-5%) Contraception Method Typical use (%preg/y) Perfect use (%preg/y) OCP Depo Provera Norplant ~3 0.3 0.05 0.1 0.3 0.05 Female Sterilization Male Sterilization 0.05 0.15 0.05 0.1 Clinical Gynecologic Endocrinology and Infertility 6th ed. Pg.880 Part 2 Pelvic Pain 26 yo G0P0 woman presents to the office with 8 years of constant pelvic pain. She has had 3 previous diagnostic laparoscopies (2 months, 2 years, and 6 years ago). All demonstrated a normal pelvis. She has recently be seen by specialists in General Surgery, GI, Urology, Orthopedics, and Gynecology. All investigations have been normal and no cause for the pain has been found. Chronic Pelvic Pain: Non-Gynecologic Causes, Childhood Sexual/Physical Abuse Pelvic Pain What other avenues of history or investigation are indicated? (you may chose up to 2) A) history of drug dependency or abuse B) repeat pelvic ultrasound C) history of previous sexual abuse/assualt D) CBC, lytes, BUN, Cr E) exploratory laparotomy Pelvic Pain Approach: 1) History - chronic vs acute 2) Physical Exam Pain History: C Severity O Onset L Location D Duration E Exacerbating/relieving factors R Radiation Pelvic Pain DDx (enormous) Gynecologic: Pregnancy: infectious-PID ectopic endometriosis spontaneous abortion adenomyosis incarcerated uterus fibroids degenerating fibroids ovarian cysts, rupture, torsion ovarian cyst - rupture dysmenorrhea hemorrhage adhesions ovarian torsion prolapse cancer Pelvic Pain DDx continued Non-Gynecologic: -urinary tract(infection, stones, retention, interstitial cystitis) -bowel(IBS, obstruction, IBD, diverticulitis, constipation, appendicitis, mesenteric adenitis, infarction, hernia) -musculoskeletal(nerve entrapment, referred pain, abdominal wall, joint, tumors, MS) -psychological trauma(~20% of chronic pelvic pain patients have a history of sexual abuse/assault) Pelvic Pain Investigations: (Dependent on symptoms and findings at presentation) Gynecology related - BHCG, cultures, U/S - laparoscopy Bowel related - stool cultures - endoscopy - U/S,CT,MRI Urologic - urine cultures, urinanalysis - IVP, U/S, CT Musculoskeletal - X-rays, CT, MRI Endometriosis Definition: Endometrial tissue growing outside of the uterus. Pain History, Endometriosis: Is pain worse with menses ? Do prostaglandin inhibitors help ? Is there pain with deep intercourse ? Is there pain with defecation when on menses ? Do you need to miss work or confine yourself to bed when in pain ? Most Common Endometriosis Sites Endometriosis: Signs & Symptoms Symptoms: Dysmenorrhea Deep Dyspareunia Pelvic Pain Infertility Pain with BM or voiding especially with menses. asymptomatic Signs: pelvic tenderness & nodularity. Retroverted and/or fixed uterus Endometriosis Diagnosis can only be made by visualizing disease by laparoscopy or laparotomy. Endometriosis Typically associated with painful menses and/or deep dyspareunia. Stage of disease does not correlate with the severity of pain symptoms. Suspect bowel involvement if painful BM (dyskesia) with menses. The diagnosis can only be made by laparoscopy of laparotomy. Endometriosis: Pain Relief Medical Therapy Oral Contraceptives Provera (MPA) Danazol GnRH-A Surgical Therapy: % of Patients 30 – 100% 55 – 100% 80 – 100% 80 – 100% 60 – 100% Endometriosis: Recurrent Pain after therapy Medical Therapy Surgical Therapy 30 – 40 % within 12 months of treatment. 13% within 3 years and 19 % within 5 years of surgery. Conclusion: For Further Information For Further Information www.pelvicpain.org www.endometriosisassn.org Courtesy Dr. Paul Claman Pelvic Mass Approach: 1) History- symptoms of bowel/bladder function - wt loss/gain - abdo girth changes - fatigue - fevers/chills - vaginal discharge - pregnancy symptoms(amenorrhea, molimina) - pain Pelvic Mass DDx: Gynecologic a) uterine pregnancy fibroid(s)-leiomyomata, leiomyosarcoma adenomyoisis endometrial carcinoma hematometria b) adnexal ovarian cyst(corp luteum, follicular, theca lutein, endometrioma, benign, malignant) ectopic pregnancy, luteoma of pregnancy tubo-ovarian abscess, pyosalpinx, pelvic abscess hydrosalpinx, fallopian tube cancer c) other pelvic kidney GI masses, abscesses, lymph nodes Pelvic Mass 2) Physical Exam - complete general survey(including nodes) - abdominal exam - pelvic-speculum -bimanual -pelvi-rectal 3) Investigations - U/S (abdominal and endovaginal) - +/- CT or MRI - pre-op investigations - +/- pregnancy test Pelvic Mass Treatment/management dependent of nature of mass Suggested site for more information http://www.utdol.com and search adnexal mass http://www.utdol.com/application/topic.asp?file=genwomen/2368&type=A&selectedTitle=1~15 Infertility Infertility: one year of ‘frequent’ unprotected intercourse without conception (Speroff 6th ed) 10-15% of couples in the reproductive age group Infertility -Epidemiology Time Required for Conception in Couples Who Will Attain Pregnancy Duration of Exposure % Pregnant 3 months 57% 6 months 72% 12 months 85% 24 months 93% Guttmacher 1956 Preliminary Diagnosis Fertility Requirements 1) Oocyte: regular ovulation, good quality oocytes 2) Normal Female Genital Tract: patent tubes, ‘relatively’ normal uterus, cervix and vagina 3) Sperm: sufficient quantity and quality 4) Implantation: appropriate endometrial/embryo interaction e.g. ‘luteal phase deficiency’, ‘septa’,‘polyps’ 5) Immunological Factors: appropriate immunological environment e.g. ‘endometriosis’, ‘antisperm antibodies’ ‘Antiphospholipid Syndrome’, ‘Blocking antibodies’ Preliminary Diagnosis 15% Ovarian Problems (15%) 35% Tubal/Pelvic Pathology (35%) Sperm Problems (35%) Unexplained (10 to 15%) 15% 35% *Pt counseling 40-40-20 Preliminary Diagnosis: Ovary Anovulation Dx - History of regular menses with molimina - mid luteal progesterone (progesterone > 20) - urinary LH surge kits - BBT’s (serial ultrasound, endometrial biopsy, symptothermal) Preliminary Diagnosis: Ovary Decreased Ovarian Reserve Poor Oocyte Quality through; premature follicular exhaustion or advancing female age Day 3 FSH levels (normal upper limit <10) Preliminary Diagnosis: Ovary Hyperprolactinemia: -suppresses GnRH pulsatile secretion (hypogonadotropic) -inhibits progesterone secretion by granulosa cells ”luteal phase defect” Hypothyroidism: -elevation of TRH leads to release of prolactin -possible interaction with autoimmune disease and increased risk of miscarriage Hyperthroidism: -75% of women with hyperthyroidism have normal menses -more of concern re: pregnancy-Graves’ Preliminary Diagnosis: Ovary Overall Primary Investigations: - Day 3 FSH - Day ‘21’ progesterone - TSH - Prolactin - rubella IgG Preliminary Diagnosis: Tubal Tubal Obstruction approximately 40% of female infertility causes; a) infection (GC, Chlamydia, TB) PID first episode 12% risk of tubal infertiity second 23% “ third 54% “ b) appendicitis c) endometriosis d) septic abortion e) tubal/pelvic surgery Preliminary Diagnosis: Tubal Overall Primary Investigations: Dependent on Radiological services available: - HSG or - Hysterosonogram with contrast or - Laparoscopy Preliminary Diagnosis: Tubal Dx -Hysterosalpingogram Preliminary Diagnosis: Tubal Dx -Hysterosonogram with Ultrasonic Contrast (echovist) Preliminary Diagnosis: Tubal Dx -Laparoscopy Preliminary Diagnosis: Sperm Dx - Semenanalysis WHO Criteria: volume concentration motility morphology > 2.0 ml > 20 million sperm/ml > 50% > 30% normal forms *> 14% strict Kruger Total motile count >40 million sperm =volume x concentration x motility Preliminary Diagnosis: Sperm Semen Variability Preliminary Diagnosis: Sperm - variability within individuals requires at least 2 separate semenanalysis separated by several weeks - spermatogenesis requires 69 to 72 days - illness during that time could lead to lower than usual parameters for that individual Note if oligospermia present check- FSH,LH,TSH,Prolactin, Testosterone, +/- Karyotype Preliminary Diagnosis: Sperm Classification: A) Pre testicular Hypothalamic, pituitary (low LH,FSH,T) B) Testicular Testicular failure(sometimes high FHS, low T) Genetic Acquired Insult C) Post testicular(normal FSH,LH,T) obstruction coital disorders Preliminary Diagnosis: Sperm Overall Primary Investigations: -semenanalysis x 2 Treatment Options Approach treatment based on Fertility Requirements 1) Oocytes 2) Normal Female Genital Tract 3) Sperm use these three categories to organize treatment options for each particular couple Treatment Options Oocyte Problems: 1) Annovulation 2) Poor Ovarian Reserve Tx-hypothyroidism -hyperprolactinemia aggressive stimulation IUI/IVF donor oocytes donor embryos adoption PCO - wt loss -clomiphene -metformin -letrozole/tamoxifen -FSH ovulation induction -laparoscopic ovarian drilling Treatment Options: Tubal In General -surgery best suited to mild distal disease -IVF best option for; proximal tubal obstruction bilateral hydrosalpinges severe distal disease Treatment Options: Tubal Surgical Repair -mild distal tubal disease in isolation can result in up to 80% pregnancy rates -with moderate to severe disease pregnancy rates fall to 30 to 15% respectively (Schlaff et al. 1990) Treatment Options: Tubal In Vitro Fertilization Initially used as a treatment for tubal obstruction where tubal surgery is not possible Currently, indications for IVF have expanded to include most forms of infertility Treatment of choice for severe tubal disease, and severe sperm defects ( ICSI +/- TESA, etc.) Treatment Options: Sperm Options dependent on degree sperm defect(s): 1) Intrauterine insemination of washed sperm - Ideal to inseminate >10 x 106 motile sperm 2) Donor sperm - safe, easy to use, much less expensive - non-genetic male parentage Treatment Options: Sperm 3) Intracytoplasmic Sperm Injection (ICSI) - require very few moving sperm - can combine with testicular sperm retrieval - requires IVF (female risks & discomfort) Treatment Options: Sperm 4) Varicocelle repair 5) Hormonal replacement (hypothalamic, pituitary) 6) Surgical repair of obstruction Conclusions 1. Preliminary Diagnosis of Infertility based on investigations of requirements of fertility a) Oocytes b) Tubes c) Sperm 2. If possible treatment is directed at specific requirements of fertility. Pelvic Relaxation/Prolapse Cystocele - downward displacement of bladder Uterine Prolapse - descent of the uterus and cervix down the vaginal canal toward the vaginal introitus Rectocele - protrusion of the rectum into the posterior vagina lumen Enterocele - herniation of small bowel into the vaginal lumen Vaginal Vault Prolapse - descent of the vaginal apex down the vaginal canal towards the introitus Cystocele / Rectocele/ Enterocele Cystocele Rectocele Descent of anterior vaginal wall and overlying bladder base herniation of bulging of posterior vaginal wall and underlying rectum into vaginal lumen Enterocele herniation of peritoneum (+/intraperitoneal contents) in areas of pelvic floor Pelvic Relaxation/Prolapse Predisposing Factors: -aging -vaginal childbirth -menopause(decreased estrogen) -changes in pelvic anatomy(surgery) -obesity -chronic cough -chronic constipation Pelvic Relaxation/Prolapse Symptoms: -Pelvic pressure, heaviness -dragging sensation -low back ache -possibly relief with lying down -voiding difficulty, incomplete emptying, UTIs -constipation(pt’s may report having to reduce the rectocele to have a bowel movement) Pelvic Relaxation/Prolapse Treatment - Conservative -Pessary, Kegels, wieght loss, stool softeners, HRT smoking cessation (wide range of pessaries exist for most forms of prolapse -not useful for rectocele) - Surgical Anterior Repair (Cystocele) Posterior Repair (Rectocele) Vault suspension(Vault Prolapse following hyst) Enterocele Repair abdominal approach(Enterocele) Vaginal Hysterectomy(Uterine Prolapse) Part 3 PAP Smear Management Screening Test - sampling of transformation zone - detection of early pre-malignant squamous lesions - yearly examination once sexually active -multiple classification systems Bethesda System widely practiced PAP Smear Management 1996 Ontario Cervical Screening Guidelines Women of all ages who are, or ever have been, sexually active should be screened. After three normal "Pap" tests (reported as satisfactory for evaluation) at one-year intervals, screening should be continued every two years. If there have been four normal "Pap" tests in the previous ten years, screening may be discontinued after the age of seventy. Note: These recommendations do not apply to those women who have had previous abnormal "Pap" tests. http://www.cancercare.on.ca/prevention_cervicalScreening.htm PAP Smear Management Possible Results(Squamous) Within Normal Limits Atypical Squamous Cells of Undetermined Significance (ASCUS) may favour reactive or premalignant/malignant process Low Grade Squamous Intraepithelial Lesion (LSIL) High Grade Squamous Intraepithelial Lesion (HSIL) Squamous Cell Carcinoma PAP Smear Management PAP Smear Management PAP Smear Management Possible Results(Adeno) Within Normal Limits Atypical Glandular Cells of Undetermined Significance (AGUS) may favour reactive or premalignant/malignant process Adenocarcinoma(endocervical, endometrial, extra-uterine, NOS) PAP Smear Management Management -AGUS referral for colposcopy & ECC, endometrial bx may need cone bx -Adenocarcinoma endometrial bx, search for primary PAP Smear Management Ontario Modified Bethesda System 1997 Ontario Modified Bethesda System 2001 Interpretation/Result Within Normal Limits Negative for Intraepithelial Lesion or Malignancy Benign cellular changes: Endometrial cells, cytologically benign in a post-menopausal woman Endometrial cells in woman >40 years of age Atypical squamous cells of undetermined significance (ASCUS) Atypical Squamous Cells Favour reactive Undetermined Significance (ASC-US) Favour SIL Cannot exclude HSIL (ASC-H) Low Grade Squamous Intraepithelial Lesion (LSIL) Low Grade Squamous Intraepithelial Lesion (LSIL) High Grade Squamous Intraepithelial Lesion (HSIL) High Grade Squamous Intraepithelial Lesion (HSIL) Squamous Cell Carcinoma Squamous Cell Carcinoma PAP Smear Management Ontario Modified Bethesda System 1997 Ontario Modified Bethesda System 2001 Atypical glandular cells of undermined significance (AGUS) Atypical Endocervical cells Favour reactive endocervical Favour neoplastic endocervical Favour endometrial Not otherwise specified Not otherwise specified Favour neoplastic Atypical Endometrial cells Not otherwise specified Favour neoplastic Atypical Glandularl cells Not otherwise specified Favour neoplastic Atypical glandular cells, consistent with adenocarcinoma in situ Malignant cells present consistent with adenocarcinoma Endocervical Adenocarcinoma in situ Adenocarcinoma Endocervical Enometrial Extra-uterine Not otherwise specified PAP Smear Management Statement of Adequacy Recommendation Within normal limits: Satisfactory for evaluation Continue with normal screening interval (see Screening Interval Guidelines) Within normal limits: Satisfactory for evaluation but limited by: state reason If previous Pap tests have been normal, and satisfactory for evaluation, continue normal screening interval. If there is no previous Pap test or no test satisfactory for evaluation, the test should be repeated earlier than one year. Unsatisfactory for evaluation Repeat in three months PAP Smear Management Diagnostic Category Recommendation Benign cellular changes: Inflammation Culture and treatment, if appropriate Continue with normal screening interval Benign cellular changes: Non-Specific If previous tests have been normal and satisfactory for evaluation, continue with normal screening interval. PAP Smear Management Diagnostic Category Atypical squamous cells of undetermined significance (ASCUS) Low-grade intraepithelial lesion (LSIL) * See ASCUS subclassification Recommendation The minimum recommendation is to repeat at six-month intervals for up to two years. If a second diagnosis of ASCUS or LSIL occurs in a two-year period, colposcopy could be considered. If there is no evidence of cytological progression on repeat Pap tests, it is acceptable to follow the patient for up to two years, at which point all patients with persistent abnormalities should be referred for colposcopy. It is noted that there will be clinical situations (e.g., poor compliance, previous abnormal Pap test) in which immediate colposcopy and biopsy are the recommended forms of investigation PAP Smear Management Diagnostic Category Recommendation High-grade intraepithelial lesion (HSIL) Colposcopy Squamous cell carcinoma Colposcopy Endometrial cells, cytologically benign in a postmenopausal woman These findings should be interpreted in light of the clinical scenario. PAP Smear Management Diagnostic Category Atypical glandular cells of undetermined significance (AGUS): Favor endometrial origin AGUS: Favor reactive endocervical cells Recommendation Suggest endometrial sampling Repeat test in six months PAP Smear Management Diagnostic Category AGUS: Favor neoplastic endocervical cells AGUS: Not otherwise specified Recommendation Colposcopy. It is recognized that follow-up of Pap tests diagnosed as AGUS may include sampling of the endocervical canal, in addition to colposcopy PAP Smear Management Diagnostic Category Atypical glandular cells consistent with adenocarcinoma in situ Recommendation Colposcopy. With cytological evidence of adenocarcinoma in situ, a diagnostic cone biopsy should be performed (i.e. knife excision, not loop electrodiathermy excision procedure - LEEP). PAP Smear Management Diagnostic Category Recommendation Malignant cells present consistent with adenocarcinoma Suggest further investigation Malignant cells present NOS Suggest further investigation NOTE: These are minimum guidelines only. There may be clinical situations which require earlier follow-up referral for colposcopy. Any repeat Pap test should not be performed earlier than three months. The Pap test should not be used in the assessment of a visible cervical lesion. These patients require biopsy for accurate diagnosis. Revised Ontario Cervical Screening Guidelines consistent with Bethesda 2001 will be released in 2005. The Ontario Cervical Screening Program will release additional information at that time. http://www.cancercare.on.ca/prevention_3550.htm Case 19 year old G0 woman presents to the ER with lower abdo/pelvic pain for 2 days. She had developed a fever today and a vaginal discharge. She has recently become sexually active, and is not using contraception. A pregnancy test is negative. Case What is the most likely diagnosis? A) early appendicitis B) chlamydial cervicitis C) disseminated herpes D) PID E) trichomonas vaginitis Gynecologic Infections Acute Pelvic Inflammatory Disease (PID) - clinical diagnosis implying patient has upper genital tract infection and inflammation -ascending infection to endometrium, tubes, peritonium -most often an STD-chlamydia, gonorrhea -rarely endogenous vaginal bacteria, TB Gynecologic Infections Presentation - spectrum of severity - fever - pain, and tenderness - RUQ pain (Fitz-Hugh-Curtis) - vaginal discharge or bleeding - nausea, vomiting, - dysuria- rare Gynecologic Infections Diagnosis: pelvic pain cervical motion tenderness adnexal tenderness with fever or- high WBC - cervical discharge - positive cultures for chlamydia, gonorrhea - high risk partner - pelvic abscess clinically, or U/S Dx Patients suspected of having PID should have U/S to r/o abscess Partner should be evaluated and treated for STD’s Gynecologic Infections Reasons to Admit for PID -abscess -moderately, severely ill -unable to tolerate oral meds -immunocompromised -pregnant -atypical infection -previous instrumentation -failed outpatient management -unreliable for follow up or compliance -uncertain diagnosis Gynecologic Infections Treatment: Outpatient - ceftriaxone 250mg IM x1 and doxycycline 100mg BID x 14 days OR Ofloxacin 400mg PO QID x 14 days and Clindamycin 450mg PO QID x 14 days (metronidazole 500mg PO BID x 14 days) Gynecologic Infections Inpatient: Cefoxitin 2g or Cefotetan 2g IV q6h (at least 48 h) and Doxycycline 100mg BID x 14 days OR Clindamycin 900mg IV q8h (at least 48 h) and Gentamicin 2mg/kg + 1.5mg/kg q8h (at least 48 h) If no improvement within 48 h may need to drain abscess -precutaneously, laparoscopically, laparotomy Pelvic Inflammatory Disease Parenteral Regimen A Cefotetan 2 g IV q 12 hours or Cefoxitin 2 g IV q 6 hours PLUS Doxycycline 100 mg orally/IV q 12 hrs Pelvic Inflammatory Disease Parenteral Regimen B Clindamycin 900 mg IV q 8 hours PLUS Gentamicin loading dose IV/IM (2 mg/kg) followed by maintenance dose (1.5 mg/kg) q 8 hours. Single daily dosing may be substituted. Pelvic Inflammatory Disease Alternative Parenteral Regimens Ofloxacin 400 mg IV q 12 hours or Levofloxacin 500 mg IV once daily WITH OR WITHOUT Metronidazole 500 mg IV q 8 hours or Ampicillin/Sulbactam 3 g IV q 6 hrs PLUS Doxycycline 100 mg orally/IV q 12 hrs Pelvic Inflammatory Disease Oral Regimen A Ofloxacin 400 mg twice daily for 14 days or Levofloxacin 500 mg once daily for 14 days WITH OR WITHOUT Metronidazole 500 mg twice daily for 14 days Pelvic Inflammatory Disease Oral Regimen B Ceftriaxone 250 mg IM in a single dose or Cefoxitin 2 g IM in a single dose and Probenecid 1 g administered concurrently PLUS Doxycycline 100 mg twice daily for 14 days WITH or WITHOUT Metronidazole 500 mg twice daily for 14 days Pelvic Inflammatory Disease Management of Sex Partners Male sex partners of women with PID should be examined and treated for sexual contact 60 days preceding pt’s onset of symptoms Sex partners should be treated empirically with regimens effective against CT and GC Gynecologic Infections Complications of PID - chronic pain, chronic PID - infertility - increased risk for ectopic pregnancy - pelvic adhesions - bacteremia with disseminated infections Gynecologic Infections Chlamydial Cervicitis: - intracelluar parasite - STD reportable disease Presentation - asymptomatic - endocervical discharge - pelvic pain discomfort to PID - dysuria, with no bacturia - post coital spotting (ALWAYS R/O CERCIAL CANCER) Gynecologic Infections Treatment Doxycylcine 100mg PO BID x 7 days OR Azthiromycin 1g PO x1 if pregnant Erythromycin, Amoxicillin Screen and treat partners Chlamydia trachomatis Azithromycin 1 gm single dose or Doxycycline 100 mg bid x 7d Chlamydia trachomatis Alternative regimens Erythromycin base 500 mg qid for 7 days or Erythromycin ethylsuccinate 800 mg qid for 7 days or Ofloxacin 300 mg twice daily for 7 days or Levofloxacin 500 mg for 7 days Chlamydia trachomatis Treatment in Pregnancy Recommended regimens Erythromycin base 500 mg qid for 7 days or Amoxicillin 500 mg three times daily for 7 days Alternative regimens Erythromycin base 250 mg qid for 14 days or Erythromycin ethylsuccinate 800 mg qid for 14 days or Erythromycin ethylsuccinate 400 mg qid for 14 days or Azithromycin 1 gm in a single dose Gynecologic Infections Gonorrhea Cervicitis: - gram negative intracellular diplococci - STD reportable disease Presentation -same as chlamydia Treatment ceftriaxone 125mg IM x1 OR cefixime 400mg PO x 1 OR ciprofloxacin 500mg PO x 1 AND Treatment for Chlamydia Gynecologic Infections Gonorrhea-male Neisseria gonorrhoeae Cervix, Urethra, Rectum Cefixime 400 mg or Ceftriaxone 125 IM or Ciprofloxacin 500 mg or Ofloxacin 400 mg/Levofloxacin 250 mg PLUS Chlamydial therapy if infection not ruled out Neisseria gonorrhoeae Cervix, Urethra, Rectum Alternative regimens Spectinomycin 2 grams IM in a single dose or Single dose cephalosporin (cefotaxime 500 mg) or Single dose quinolone (gatifloxacin 400 mg, lomefloxacin 400 mg, norfloxacin 800 mg) PLUS Chlamydial therapy if infection not ruled out Gynecologic Infections Gonorrhea - intracellular Gram negative diplococci Gynecologic Infections Vulvovaginitis Organism Candida(Yeast) Discharge White thick Symptoms Wet Mount -itching KOH -satellite lesions -hyphae -edematous -red Ph <5 Bacterial Vaginosis (anaerobes, Gardnerella etc.) grey, thin, diffuse fishy odour -worse after intercourse -no irritation/ inflammation 5-5.5 clue cells KOH +whiff test Gynecologic Infections Candida Vulvitis Gynecologic Infections Candida-KOH prep Hyphea Gynecologic Infections Clue cell- epithelial cell with bacteria clustered peripherally Gynecologic Infections Vulvovaginitis Organism Trichomonasis (Trichomonas Vaginalis) Physiologic ( high E2 states) Discharge Symptoms yellow/green -strawberry spots clear/white Wet Mount Ph -fagellated 5-6.5 protozoa - no irritation/ -normal <4.5 inflammation epithelial cells Gynecologic Infections Trichomonas- strawberry spots Gynecologic Infections Trichomonas- fixed and stained Gynecologic Infections Treatment Candida(Yeast) -clotrimazole, miconazole, terconazole -Diflucan 150 mg PO x 1(resistant cases) -lactobacillus acidophilus Bacterial Vaginosis Metronidazole 500mg PO BID x 7 days (or 2g PO x1) OR Clindamycin 300mg PO BID x 7 days OR topical above creams QHS x 7 days Trichomonas Metronidazole 500mg PO bid x 7days or 2g PO x 1 Gynecologic Infections Vulvar Lesions Condylomata Acuminata - human papilloma virus (HPV) - strongly associated with cervical/vulvar intraepithelia neoplasia and cancer - acetowhite lesions, wartlike progections Treatment - podofilox - imiquimod - liquid N - TCA - laser, electro, excision - intralesional interferon Gynecologic Infections Condylomata Acuminata Gynecologic Infections Condylomata Acuminata Gynecologic Infections Condylomata Acuminata Gynecologic Infections Condylomata Acuminata-male Gynecologic Infections Condylomata Acuminata-perianal Papillomavirus Patient-applied Podofilox 0.5% solution or gel or Imiquimod 5% cream Provider-administered Cryotherapy or Podophyllin resin 10-25% or Trichloroacetic or Bichloroacetic acid 80-90% or Surgical removal Papillomavirus Vaginal warts Cryotherapy or TCA/BCA 80-90% Urethral meatal warts Cryotherapy or podophyllin 1025% Anal warts Cryotherapy or TCA/BCA 80-90% Papillomavirus Treatment in Pregnancy Imiquimod, podophyllin, podofilox should not be used in pregnancy Many specialists advocate wart removal due to possible proliferation and friability HPV types 6 and 11 can cause respiratory papillomatosis in infants and children Preventative value of cesarean section is unknown; may be indicated for pelvic outlet obstruction Gynecologic Infections Vulvar Lesions Molluscum Contagiosum - molluscipoxvirus - mildy contagious - nodule with umbilicated centre Treatment - curette - TCA, silver nitrate, carbonic acid Gynecologic Infections Molluscum Contagiosum Gynecologic Infections Molluscum Contagiosum Gynecologic Infections Molluscum Contagiosum Gynecologic Infections Genital Ulcers Description Diagnosis Herpes (HSVII, I(10%)) -prodromal viral culture -small vessicle progresses to shallow, painful, inflamed Syphilis (Treponema pallidum) -smooth, raised border painless, smooth base Chancroid (Hemophilus ducreyi) -irregular border, deepculture Gram stain undermined edges, painful -GNB in rows +/- buboe(tender lymphadenopath dark field micro -spirochetes -VDRL etc. Gynecologic Infections Genital Herpes Gynecologic Infections Genital Herpes Gynecologic Infections Genital Herpes Genital Herpes First Clinical Episode Acyclovir 400 mg tid or Famciclovir 250 mg tid or Valacyclovir 1000 mg bid Duration of Therapy 7-10 days Genital Herpes Episodic Therapy Acyclovir 400 mg three times daily x 5 days or Acyclovir 800 mg twice daily x 5 days or Famciclovir 125 mg twice daily x 5 days or Valacyclovir 500 mg twice daily x 3-5 days or Valacyclovir 1 gm orally daily x 5 days Genital Herpes Daily Suppression Acyclovir 400 mg bid or Famciclovir 250 mg bid or Valacyclovir 500-1000 mg daily Gynecologic Infections Syphilis-male Gynecologic Infections Syphilis-female Gynecologic Infections Syphilis- Treponema pallidum Gynecologic Infections Darkfield Microscopy - Treponema pallidum Syphilis Primary, Secondary, Early Latent Recommended regimen Benzathine Penicillin G, 2.4 million units IM Penicillin Allergy* Doxycycline 100 mg twice daily x 14 days or Ceftriaxone 1 gm IM/IV daily x 8-10 days (limited studies) or Azithromycin 2 gm single oral dose (preliminary data) *Use in HIV-infection has not been studied Gynecologic Infections Chancroid-male Gynecologic Infections Chancroid-male with regional adenopathy Gynecologic Infections Chancroid-male with regional adenopathy node ruptured Gynecologic Infections Hemophilus ducreyi(Chancroid GNB in row-school of fish) Chancroid Azithromycin 1 gm orally or Ceftriaxone 250 mg IM in a single dose or Ciprofloxacin 500 mg twice daily x 3 days or Erythromycin base 500 mg tid x 7 days Gynecologic Infections Genital Ulcers Treatment Herpes (HSVII, I(10%)) 10 acyclovir 400mg PO TID x 7-10d 20 acyclovir 400mg PO TID x 5d Syphilis (Treponema pallidum) benzathine penicillin G 2.4 million units IM -treat partners -reportable illness Chancroid (Hemophilus ducreyi) -erythromycin 500mg QID x 7 days OR ceftriaxone 250mg IM x 1 OR azithromycin 1g PO x1 -treat partners Case 31 yo woman complains of sudden onset of LLQ pain. The pain is constant and worse with movements. She is late for her menses by 3 weeks and has been actively trying to get pregnant. Past medical history is positive for PID requiring hospitalization for IV antibiotics for 4 days. Her vitals are stable, and afebrile. She is having mild vaginal bleeding(<1pad) that started today. Case What investigations would be appropriate? (chose up to 3) A) CBC B) pelvic ultrasound (endovaginal and transabdominal) C) flat plate(x-ray) of abdomen D) Bhcg- quantitative if positive E) sigmoidoscopy with possible colonscopy F) IVP with delayed films Ectopic Pregnancy 1-2% of all pregnancies ~14% if previous ectopic pregnancy ~ 1/30,000 pregnancies will be heterotopic(1 IUP + 1 ectopic) Ectopic Pregnancy Types: Tubal -Ampullary -Isthmic -Fimbrial -Cornual 80% 12% 5% 2% Abdominal Ovarian Cervical 1.4% 0.2% 0.2% Ectopic Pregnancy Risk Factors: Tubal surgery Previous ectopic Previous salpingitis Assisted Reproduction Age < 25 previous pelvic infection Infertility Cigarettes Vaginal douching Relative Risk 20 10 4 4 3 3 2.5 2.5 2.5 Ectopic Pregnancy Risk Factors: -IUD use does not increase risk of ectopic over women using no contraception -however, if pregnant with IUD 3-4% will be ectopic -uterine anomalies -?progestins? Ectopic Pregnancy Diagnosis: -amenorrhea -pain -spotting (vaginal bleeding not from direct blood loss from tubal bleeding- hormonal event from estrogen breakthrough bleeding) -hypovolemic shock Ectopic Pregnancy Investigations: -Hx & Px -Bhcg Quantitative, CBC, G&S, -pelvic ultrasound Endovaginal Bhcg> 1200-1500 gestational sac of a normal pregnancy should be visible in uterus -serial Bhcg’s normal doubling time of Bhcg is about 2 days inadequate doubling is concerning for ectopic or abnormal intrauterine -laparoscopy -culdocentesis(of non clotted blood)-more historical note only Ectopic Pregnancy Treatment Surgical(laparotomy,laparoscopy) -salpingectomy, salpingostomy Medical - methotrexate 50mg/m2 IM x 1 serial Bhcg weekly f/u - 10-15% failure rate Ectopic Pregnancy Ectopic Pregnancy Ectopic Pregnancy Salpingostomy with electrocaughtery Ectopic Pregnancy Ectopic Pregnancy Electrocaughtery for hemostatsis Ectopic Pregnancy In this case salpingectomy needed for hemostasis Ectopic Pregnancy Criteria Methotrexate Tx: -stable patient - < 3.5 - 4 cm of ectopic pregnancy -Bhcg<5000 iu (Dr. Claman of U of O) -no fetal cardiac activity -compliant to follow up -no renal/hepatic/hematologic impairment Violence Against women - ~ 1 in 2 women (aged 16 onwards) will experience some form of physical or sexual violence -prevalence of domestic violence in Canadian women is 29% - acts of violence against women are ‘significantly under reported’ - estimated that only 3% of violent acts against women are identified by primary physicians Violence Against women - abuse is often increased during pregnancy - first episode of abuse may occur in pregnancy (14% of abused women) - estimated that only 3% of abused pregnant women reported the abuse Violence Against women Role of Physician: 1) be aware 2) be approachable 3) identify problems 4) provide support and medical care Violence Against women When to suspect physical abuse: - multiple visits to office with vague complaints - shyness, fear, crying, accompanied by male partner who is reluctant to leave - substance abuse, depression, attempts a self harm - injuries inconsistent with explanation of mechanism Violence Against women Support and Medical Care: - not physicians role to contact authorities - Inappropriate interventions can cause situation to escalate at home, endangering woman or children more - clear documentation - provide information on community supports, and resources and information on an exit plan - support woman’s decisions (refer for additional support if needed) Violence Against women Exit Plan: 1- Prepare a change of clothing for herself and children with medications, keys (house and car) and keep with a friend or neighbour. 2- cash, cheque book, and savings account book with clothing 3- Important papers, birth certificates, SIN card, drivers licence, automobile title, mortgage papers should be taken if possible 4- Have a plan detailing exactly where to go regardless of time of day(family, friend, shelter etc.) Violence Against women Regardless of status of plan patient should leave immediately if she feels there is a danger to the life, health, or safety of herself or her child(ren) Good Luck