Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
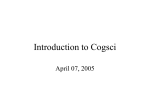
A woman with a bifrontal headache and confusion 2013 July-August Featured Case DR M Haghighi MD History of Present Illness • A woman in her thirties developed a progressive bifrontal headache associated with a temperature to 100.0°F (37.8°C). She went to sleep in the late afternoon. • Approximately 24 hours later, her husband found her difficult to arouse, nonverbal and non-interactive. She was unable to arise from bed, answer questions or follow commands, and appeared confused. Past Medical History • She had previously been well. Medications • None. Epidemiological History • She lived with her husband and young daughter, and worked as a housekeeper. She did not drink alcohol, smoke tobacco, or use illicit drugs. Physical Examination • The patient appeared somnolent, arousable to painful stimuli, and unable to follow commands consistently. The blood pressure was 143/60 mm Hg, pulse 59 beats per minute, temperature 38.3°C (101.0°F), respirations 20 beats per minute, and oxygenation 98% while breathing room air. • On neurological examination, the pupils were symmetric and sluggishly reactive from 4mm to 3mm; extra-ocular movements were grossly intact. She was able to open her eyes and moved all four extremities spontaneously. Deep tendon reflexes were 2+ and symmetric bilaterally. The remainder of the examination was otherwise normal. Studies • Her white blood cell count was 17,900 per cubic millimeter (reference range 4,500-11,000) with an absolute neutrophil count of 14,770 cells per cubic millimeter (ref. 18007700). The hemoglobin and platelet counts were normal. Other routine laboratory tests including blood levels of electrolytes, and tests of coagulation, renal function and liver function were normal. Serum toxicology panel was negative. • Urinalysis revealed a specific gravity of 1.030, trace ketones, trace urobilinogen, 2+ protein, and 10-20 red blood cells and 3-5 white blood cells per high power field. Culture of the urine and blood were obtained, and were sterile. WHAT IS YOUR RECOMMENDATION? • A chest radiograph was normal. Computed tomography (CT) of the head, performed without the administration of contrast revealed enlargement of the lateral and third ventricles consistent with hydrocephalus. CT of the brain, sagittal view, without contrast WHAT IS YOUR PLAN? Clinical Course • The patient was intubated and bilateral external ventricular devices were placed emergently, with improvement in the severity of hydrocephalus on follow-up CT imaging. • Analysis of cerebral spinal fluid (CSF) obtained from the external ventricular drains revealed a glucose level of 79 mg/dl (reference range 50-75), a normal total protein level; 1150 red blood cells per cubic millimeter, and 2 white blood cells per cubic millimeter. WHAT IS YOUR NEXT STEP? • Dexamethasone (4mg every 6 hours), levetiracetam, ceftriaxone, vancomycin, and acyclovir were administered. • MRI of the cervical, thoracic, and lumbar spine were negative. An ophthalmologic examination revealed no evidence of ocular involvement. • Testing for serum HIV antibodies, interferongamma release assay, and mycobacterial DNA from the cerebrospinal fluid were negative. Cultures of the cerebrospinal fluid for bacteria, fungi, and mycobacteria were sterile. WHAT IS YOUR RECOMMENDATION? CT of the brain, sagittal view, without contrast • (CT) of the head, performed without the administration of contrast revealed enlargement of the lateral and third ventricles consistent with hydrocephalus , and • a fluid-filled vesicular structure in the frontal horn of the left lateral ventricle near the foramen of Monroe with a soft-tissue density inside the cyst, and calcified densities scattered throughout the supratentorial brain. • On the second hospital day, magnetic resonance imaging (MRI) of the brain was performed with the administration of contrast . DIFERENTIAL DIAGNOSIS DIFFERENTIAL DIAGNOSIS • Tuberculous meningitis caused by Mycobacterium tuberculosis • Echinococcus spp. • Aspergillus spp. • Sarcoidosis • Malignancy • Cryptococcal meningitis • Vasculitis • Coenurosis • Brain Abscess • Toxoplasmosis • MRI of the brain revealed a nonenhancing multilobed cystic mass (28.4mm in its greatest dimension) within the left lateral ventricle and numerous calcified foci throughout the cerebral hemispheres, as were seen on CT. FINAL DIAGNOSIS • The soft-tissue density seen within the cyst on CT of the head was consistent with a scolex, and the innumerable calcified densities scattered throughout the supratentorial brain were suggestive of neurocysticercosis. • On the seventh hospital day, a left-sided mini-craniectomy with left frontal endoscopic removal of the intraventricular cyst was performed. The left-sided external ventricular drain was also removed. • Histopathological examination of the resected tissue with hematoxylin and eosin staining revealed a cysticercus celluosac with the encysted larva . The scolex with suckers and hooklets were visible within the sac. Testing for cysticercus IgG antibodies was positive in the serum and negative in the cerebrospinal fluid. Gross pathology of resected intraventricular cystic lesion. H and E stain of resected cystic mass showing suckers and hooklets. H and E stain of T. solium with suckers and hooklets. Final Diagnosis • Intraventricular and intraparenchymal neurocysticercosis, caused by Taenia solium infection.