Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
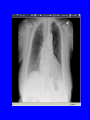
84 yo woman with a cough Mary H. Pak, M.D., FACP Primary Care Conference February 22, 2006 Disclosure Received honorarium for being on an advisory panel for Pfizer related to linezolid. Case presentation • EG is an 84 yo woman who presented to the ER with a cough of 1-2 weeks in duration. – She notes some shortness of breath, mostly related to the coughing fits as well as intermittent chest pains. – There is no sputum production. – She has had difficulty sleeping because of the coughing. – She has some nausea related to the cough but no emesis. Case presentation (con’t) • PMH: Metastatic renal cell CA (treated in eastern Europe, s/p nephrectomy 6 years ago) Hypertension Arthritis Depression Case presentation (con’t) Medications: captopril 50 mg po b.i.d. Ambien prn Robitussin (OTC) Tylenol prn Allergies: Morphine nausea SH/FH: widowed, lives with daughter in Madison. Denies any tobacco or alcohol use. FH heart disease, no other cancers. No information about her immunization history. Case presentation (con’t) ROS: No fevers, chills or sore throat No sputum production or hemoptysis No known sick contacts Irritated and itchy eyes occasionally Diffuse arthralgias Case presentation (con’t) Physical Examination – T 98.9, BP 145/64, pulse 70, resp 16, 95% RA – Lungs were clear to auscultation B/L – Heart was regular in rhythm with no appreciable gallops, murmurs or rubs – Extremities were noted to have trace ankle edema with negative Homan’s sign Case presentation (con’t) Laboratory data: • WBC 8.1 (normal diff), H/H 11.5/33, plt 285 • Normal electrolytes, creatinine 1.7, BUN 40 • BNP 175 • Troponin 0.1 • D-dimer 0.6 Case presentation (con’t) • Differential diagnosis: viral URI (including RSV, adenovirus) or URI symptoms related to Influenza type virus atypical respiratory infections including Mycoplasma pneumoniae, Chlamydia pnueumoniae, Bordetella pertussis, Bordetella parapertussis Cough secondary to post nasal drip GERD Case presentation (con’t) • We sent off a nasopharyngeal swab for Bordetella pertussis DNA PCR and culture • Placed the patient in respiratory droplet isolation • Started azithromycin 500 mg Objectives • Case presentation • Differential diagnosis of prolonged cough • Discussion regarding epidemiology, diagnosis and treatment of pertussis • Role of adult vaccination Bordetella pertussis: epidemiology • 25,827 cases reported in the U.S in 2004 60% cases in adolescents (11-18) and adults (>20) • Transmitted from person-to-person through aerosolized respiratory droplets from cough or sneeze or direct contact with secretions from infected persons. • Incubation period 5 – 21 d (typical 7 – 10d) • Endemic in U.S., epidemic every 3 - 4 years. Tiwari T, MMWR 2005 MMWR 54 (50), 1284 MMWR 54 (50), 1285 Bordetella pertussis: economics • Pertussis in adults has been shown to generate medical and nonmedical costs of $773 per case-patient. • Often leads to 10 days of missed work. Lee GM, Clin Inf Dis 2004 Bordetella pertussis • Uniquely human pathogen • Only disease for which universal childhood vaccination is recommended that has an increasing trend in reported cases in U.S. In early vaccine years (1920 – 40), average annual rate 150 per 100,000 population After universal vaccination during 1940’s, declined to 1 case per 100,000. In 2004, 8.4 cases per 100,000 Robbins JB, Clin Inf Dis 1999 Tiwari T, MMWR 2005 Bordetella pertussis: clinical manifestations • Catarrhal period (1 – 2 weeks) Coryza, mild fever, non productive cough Infants can have apnea and respiratory distress • Paroxysmal period (2 – 6 weeks) Paroxysmal cough, inspiratory “whoop”, posttussive vomiting • Convalescent period (> 2 weeks) Tiwari T, MMWR 2005 Bordetella pertussis: clinical manifestations • Potential complications: – Weight loss (due to coughing) – Sleep disturbance – Effects generated by increased pressure due to severe coughing including pneumothorax, epistaxis, subconjunctival hemorrhage, subdural hematoma, rib fracture, urinary incontinence. – Secondary bacterial pneumonia including aspiration pneumonia related to posttussive vomiting Dworkin MS, Ann Intern Med 2005 Tiwari T, MMWR 2005 Bordetella pertussis: testing • Culture of the nasopharyngeal mucus is the “gold standard” Prefer aspiration samples via hand-trap If swabs are to be used, Dacron is recommended since alginate may inhibit PCRbased assays and cotton may be toxic to the bacteria. • Send for B. pertussis PCR and culture. Dworkin MS, Ann Intern Med 2005 Bordetella pertussis: diagnostic barriers • Reluctance to cause patient discomfort • Need for special transport medium (BordetGengou medium) • Tendency for the organism to die before culture confirmation • Low yield of PCR and culture in the setting of partial immunity • Chronicity of cough delays diagnosis to a time when diagnostic yield is poorest. • Lack of reliable serologic markers Dworkin MS, Ann Intern Med 2005 Testing for pertussis is not sufficiently sensitive for treatment decision to be guided by test results alone. Bordetella pertussis: treatment Tiwari T, MMWR 2005 Bordetella pertussis: vaccination • In May, 2005, Boostrix (GlaxoSmithKline) was licensed for vaccination in persons between the ages of 10 – 18. • In June, 2005, Adacel (Sanofi-Aventis) was licensed for use in person between 11 – 64 years. • Both vaccines are Tdap vaccines which contains tetanus, diphtheria and acellular pertussis. MMWR 2005; 54 (50) Bordetella pertussis: vaccination • On June 30, 2005, the Advisory Committee on Immunization Practices (ACIP) recommended a single dose of Tdap for all persons aged 11 – 18 years. • In October, 2005, ACIP recommended a single dose of Tdap for adults aged 19 –64. • No adoption into immunization guidelines as yet. Conclusion • Pertussis is not solely a childhood disease. Pertussis is a “community-acquired disease of all ages” • Reported cases of pertussis has been rising significantly particularly in the adolescents and adults. • Diagnostic testing is not always reliable. Presumptive treatment with a macrolide is recommended. • Additional vaccinations in adulthood might help to decrease the reservoir of pertussis. References 1) 2) 3) 4) 5) 6) 7) Dworkin MS. Adults are Whooping, but Are Internists Listening? Ann Intern Med 2005; 142: 832-835. Tiwari T, Murphy TV, Moran J. Recommended Antimicrobial Agents for the Treatment and Postexposure Prophylaxis of Pertussis: 2005 CDC Guidelines. MMWR 2005; 54 (RR-14): 1- 15. Pertussis – United States, 2001 – 2003. MMWR 2005; 54 (50): 1283-1286. Cherry JD. Epidemiological, Clinical and Laboratory Aspects of Pertussis in Adults. Clin Inf Dis 1999; 28 (Suppl 2): S112-S117. Keitel WA. Cellular and Acellular Pertussis Vaccines in Adults. Clin Inf Dis 1999; 28 (Suppl 2): S118-S123. Gardner P. Indications for Acellular Pertussis Vaccines in Adults: The Case for Selective Rather than Universal Recommendations. Clin Inf Dis 1999; 28 ( Suppl 2): S131-S135. Orestein WA. Pertussis in Adults: Epidemiology, Signs, Symptoms and Implications for Vaccination. Clin Inf Dis 1999; 28 (Suppl 2) S147-S150. References (con’t) 8) 9) 10) Ward JI, et al. Efficacy of an Acellular Pertussis Vaccine among Adolescents and Adults. N Eng J Med 2005; 353: 1555-1563. Robbins JB. Pertussis in Adults: Introduction. Clin Inf Dis 1999; 28 (Suppl 2): S91-93. Hewlett EL. A Commentary on the Pathogenesis of Pertussis. Clin Inf Dis 1999; 28 (Suppl 2): S94-S98.