Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
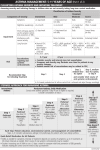
Danielle Gilliam M.D., PGY III University of South Alabama Pediatrics 2011 Most common childhood chronic disorder Increase in incidence by 50 % over the last two decades In 2007, 9% of children 0 to 17 years of age (6.7 million children) had asthma, according to data from the National Health Interview Survey. The cost of illness related to asthma is around $6.2 billion per year in the United States. Each year, an estimated 1.81 million people with asthma require treatment in the emergency department with approximately 500,000 hospitalizations Family Hx of asthma Prematurity Race ( African and Native Americans ) Low socioeconomic settings Urban settings ( pollutants ) Increased indoor irritants ( cigarette smoke, dust mites, pets, recycled air ) History of Atopy ( eczema, allergies and chronic rhinitis / sinusitis ) Cough ( mostly dry and hacking, specially at night ), Wheezing ( mainly expiratory) Shortness of Breath Chest Pain Precipitating factors [(URIs mostly viral occasionally atypical pneumonia. Bacterial causes very rare)], exercise, cold weather, allergens, cigarette smoke) Increased AP diameter of the chest with hyperinflation A silent chest is a medical emergency Detailed history of the symptoms Physical exam Spirometry with reduced FEV1 < 80 % and FEV/FVC < 65 % indicative of airflow obstruction ( children in which spirometry is not possible a trial of asthma meds should be done if indicated by other sxs ) Ancilliary studies ( bronchoprovocative testing, CXR, sweat chloride test, barium swallow and skin testing) Asthma Bronchiolitis (esp in infants), bronchitis, laryngotracheobronchitis, tracheitis Foreign body aspiration Functional abnormalities ( GERD, CF, BPD, immunodeficiency etc ) Structural abnormalities ( laryngotracheomalacia, vascular rings, tracheal stenosis / webs, tumors etc ) Assessment of impairment – Has your asthma awakened you at night or in the early morning? – Have you needed your quick-acting relief medication more than usual? – Have you needed any unscheduled care for your asthma, including calling in, an office visit, or going to the emergency room? – Have you been able to participate in school/work and recreational activities as desired? Assessing asthma control and adjusting therapy in children 0-4 years of age Components of control Classification of asthma control (0-4 years of age) Well-controlled Very poorly controlled Symptoms 2 days/week >2 days/week Throughout the day Nighttime awakenings 1x/month >1x/month >1x/week Some limitation Extremely limited >2 days/week Several times per day 2-3/year >3/year Impairment Interference with normal activity None Short-acting beta2-agonist use for symptom control (not prevention 2 days/week of EIB) Exacerbations requiring oral systemic corticosteroids Risk Not-well controlled 0-1/year Medication side effects can vary in intensity from none to very troublesome and worrisome. The Treatment-related adverse effects level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk. Maintain current treatment. Recommended action for treatment Step up (1 step) and Reevaluate in 2-6 weeks. Regular followups every If no clear benefit in 4-6 weeks, 1-6 months. consider alternative diagnoses or adjusting therapy. Consider step down if well controlled for at For side effects, consider least 3 months. alternative treatment options. Consider short course of oral systemic corticosteroids, Step up (1-2 steps), and Reevaluate in 2 weeks. If no clear benefit in 4-6 weeks, consider alternative diagnoses or adjusting therapy. For side effects, consider alternative treatment options. Classifying asthma severity and initiating treatment in children 5-11 years of age Classification of asthma severity (5-11 years of age) Components of severity Intermittent Persistent Mild Moderate Severe Symptoms 2 days/week >2 days/week but Daily not daily Nighttime awakenings 2x/month 3-4x/month Short-acting beta2-agonist use for symptom control (not prevention of EIB) 2 days/week >2 days/week but Daily not daily Several times per day Minor limitation Some limitation Extremely limited FEV1 = >80 percent predicted FEV1 = 60-80 percent predicted FEV1/FVC >80 percent FEV1/FVC = 75-80 FEV1/FVC <75 percent percent Interference with normal activity None Throughout the day >1x/week but not Often 7x/week nightly Impairment Normal FEV1 between exacerbations Lung function FEV1 >80 percent predicted FEV1 <60 percent predicted FEV1/FVC >85 percent 0-1/year (see footnote) Risk Exacerbations requiring oral systemic corticosteroids 2/year (see footnote) Consider severity and interval since last exacerbation Frequency and severity may fluctuate over time for patients in any severity category Relative annual risk of exacerbations may be related to FEV1 Step 1 Recommended step for initiating treatment Step 2 Step 3, medium dose ICS option Step 3, medium dose ICS option, or step 4 And consider short course of oral systemic corticosteroids In 2-6 weeks, evaluate level of asthma control that is achieved, and adjust therapy accordingly. Assessing asthma control and adjusting therapy in children 5-11 years of age Components of control Symptoms Nighttime awakenings Interference with normal activity Short-acting beta2-agonist use for symptom control (not Impairment prevention of EIB) Classification of asthma control (5-11 years of age) Well-controlled Not-well controlled Very poorly controlled 2 days/week but not more than >2 days/week or multiple times Throughout the day once on each day on 2 days/week 1x/month None 2 days/week 2x/month 2x/week Some limitation Extremely limited >2 days/week Several times per day Lung function FEV1 or peak flow FEV1/FVC >80 percent predicted/personal 60-80 percent best predicted/personal best >80 percent 75-80 percent <60 percent predicted/personal best <75 percent 2/year (see footnote) Exacerbations requiring oral 0-1/year systemic corticosteroids Consider severity and interval since last exacerbation Risk Reduction in lung growth Evaluation requires long-term followup Treatment-related adverse effects Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk. Maintain current step. Recommended action for treatment Regular followup every 1-6 months. Consider step down if well controlled for at least 3 months. Step up at least 1 step and Reevaluate in 2-6 weeks. For side effects, consider alternative treatment options. Consider short course of oral systemic corticosteroids, Step up 1-2 steps, and Reevaluate in 2 weeks. Classifying asthma severity and initiating treatment in youths greater than or equal to 12 years of age and adults Classification of asthma severity ( 12 years of age) Components of severity Impairment Normal FEV1/FVC: 8-19 yr 85 percent Mild Moderate Severe Throughout the day 2 days/week >2 days/week but not daily Daily Nighttime awakenings 2x/month 3-4x/month Short-acting beta2-agonist use for symptom control (not prevention of EIB) 2 days/week >2 days/week but not daily, and not more than 1x on Daily any day Several times per day Minor limitation Extremely limited Interference with normal activity None Normal FEV1 between exacerbations Lung function 60-80 yr 70 percent FEV1 >80 percent predicted FEV1 80 percent predicted FEV1/FVC normal >1x/week but not Often 7x/week nightly Some limitation FEV1 <60 FEV1 >60 but <80 percent predicted percent predicted FEV1/FVC FEV1/FVC reduced reduced >5 5 percent percent FEV1/FVC normal 0-1/year (see footnote) Risk Persistent Symptoms 20-39 yr 80 percent 40-59 yr 75 percent Intermittent Exacerbations requiring oral systemic corticosteroids 2/year (see footnote) Consider severity and interval since last exacerbation Frequency and severity may fluctuate over time for patients in any severity category Relative annual risk of exacerbations may be related to FEV1 Recommended step for initiating treatment Step 1 Step 2 Step 3 Step 4 or 5 And consider short course of oral In 2-6 weeks, evaluate level of asthma control that is achieved and adjust therapy accordingly. Assessing asthma control and adjusting therapy in youths greater than or equal to 12 years of age and adults Components of control Classification of asthma control ( 12 years of age) Well-controlled Not-well controlled Very poorly controlled Throughout the day Symptoms 2 days/week >2 days/week Nighttime awakenings 2x/month 1-3x/week Interference with normal activity None Some limitation Extremely limited >2 days/week Several times per day >80 percent predicted/personal best 60-80 percent predicted/personal best <60 percent predicted/personal best 0 1-2 3-4 Short-acting beta2-agonist use for symptom control (not Impairment prevention of EIB) FEV1 or peak flow 4x/week 2 days/week Validated questionnaires ATAQ ACQ 0.75* ACT 20 1.5 16-19 N/A 15 2/year (see footnote) Exacerbations requiring oral 0-1/year systemic corticosteroids Consider severity and interval since last exacerbation Risk Progressive loss of lung function Evaluation requires long-term followup care Treatment-related adverse effects Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk. Maintain current step. Recommended action for treatment Regular followups every 1-6 months to maintain control. Consider step down if well controlled for at least 3 months. Step up 1 step and Reevaluate in 2-6 weeks. For side effects, consider alternative treatment Avoidance of risk factors Exercise induced bronchospasm : short acting beta agonists ( albuterol ) 10-15 min prior to activity Intermittent : Rescue albuterol treatments as needed, systemic corticosteroids reserved for severe exacerbation Mild Persistent : Low dose inhaled corticosteroids (ICS) (e.g. Pulmicort, Asmanex, Flovent, QVAR) Moderate persistent : Low to medium dose ICS and either a long acting beta agonists ( Foradil, Serevent ) or a leukotriene modifier ( Singulair ) Severe Persistent : High dose ICS and a long acting beta agonist . Advair ( Fluticasone + Salmeterol ) Controller medications: ◦ ◦ ◦ ◦ Inhaled corticosteroids, Inhaled cromolyn or nedocromil, Long-acting bronchodilators (Salmeterol), Leukotriene antagonists (Montelukast) Rescue medications: Short-acting bronchodilators, Systemic corticosteroids Inhaled ipratropium or atrovent Drugs Beclomethasone Product Availability 40 mcg to 80mcg/ inh MDI (QVAR) Fluticasone HFA MDI 44 mcg, 110 mcg, 220 mcg/inh (Flovent) 50 mcg, 100 mcg, 250 mcg/inh Mometasone DPI 110 mcg, 220 mcg/inh (Ventolin) COMBOS Fluticasone + Salmeterol (Advair) Diskus (all have 50 mcg salmet) 100/50, 250/50, 500/50 mcg/inh 45/21, 115/21, 230/21 HFA (all have 21 mcg salmet) Budesonide + Formoterol 80/4.5 mcg, 160/4.5 mcg (Symbicort) HFA and MDI Side Effects: Common= couph, dysphonia, oral candidiasis, upper RTI, throat irritation Serious= decreased growth velocity in children, HPA suppresion, reduced bone mineral density, cataracts (dose and duration dependent) Combo meds= above +Headache, dizziness, palpitations, tremor Evaluate treatments every 2-3 months and step down as appropriate or go up on the dose of ICS for recurrent exacerbations ICS and long acting beta agonists have proven better efficacy compared to alternative treatments ( leukotriene modifiers, cromolyn. theophylline ) Studies have shown MDIs with spacers to be more efficacious and practical than nebulizers in routine application Asthma exacerbation is a medical emergency. Don’t delay evaluation and treatment. 1) Early/Immediate Phase : characterized by bronchoconstriction. 2) Late Phase (6-8 hours) : airway inflammation and hyper-responsiveness Management should emphasize ◦ 1) Initial stabilization ◦ 2) progressive monitoring and treatment ◦ 3)eventually discharge planning O2 to keep sats >92% Bronchodilators : Beta Agonist (Albuterol) : via nebulizer Q 15-20 minutes times three then Q2 twice if needed and then Q4-6 hrs ATC/PRN If needed more frequently PICU admisision Ipratropium ( Atrovent ) via nebulizer may be given with the first three albuterol treatments then Q4-8 ATC/PRN Levalbuterol ( Xopenex ) : selective beta 2 agonist. Not routinely used. Good alternative for continuous therapy if side effects from albuterol experienced Start Corticosteroids if; ◦ ◦ ◦ ◦ No response after one nebulised t/t Patient is steroid dependent Has had a recent ER visit for asthma Previous admission to ICU Steroid PO (Prednisolone 2mg/k/d) or Steroid IV (Solumedrol 2mg/k IV/IM bolus then 1-2mg/k/d divided Q6) x 3-10 days If greater than 5 day course, will need to wean Continuous Albuterol Magnesium Sulfate (IV) IV Terbutaline or Epinephrine Ketamine Intubation for respiratory failure Heliox Solumedrol IV Use of ketamine in acute severe asthma V. J. Sarma 30 DEC 2008 Randomized, Double-Blind, Placebo-Controlled Trial of Intravenous Ketamine in Acute Asthma, Joseph C Howton MD, John Rose MD, Scott Duffy MD, Tom Zoltanski and M.Andrew Levitt DO Wean oxygen as tolerated Advance diet as tolerated and wean IVF accordingly Social services consult : home nebulizer, supplies, insurance issues Respiratory Consult : teaching nebulizer / MDI treatments Prescribe controller meds according to classification Finish course of antibiotics and steroids F/U with pediatrician: two to three days