Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
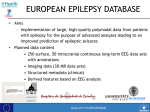
Comprehensive Video EEG monitoring JWM Neurology Kate Kobza, MD August 2006 Why do we need it? Limitations of routine EEG: Limited sampling An EEG is a sampling of brain activity occurring at the time of the recording Seizures and spells are paroxysmal and may be missed on a short study No video to correlate patient behavior with suspicious EEG changes Limitations of routine EEG: Yield of a single routine scalp EEG is 50% Certain artifacts and normal variants can be confused with epileptiform discharges Some EEG abnormalities do not have a close correlation with clinical seizures Limitations of routine EEG: Pathophysiologically – epileptic seizures are characterized by an excessive, disorderly, neuronal discharge An EEG study may disclose epileptiform abnormalities which have a high correlation with occurrence of epileptic seizures The only way to definitively prove epilepsy is to record a seizure What does a video EEG study consist of? Methodology EEG electrodes are attached to the scalp with glue ECG electrodes are placed Patient is moved to a room with video monitoring Patient and family are given an alarm to push with any spell Trained nurses and staff respond to alarms to observe patient and treat if necessary Methodology Miscellaneous options: Antiepileptic medications may be discontinued or decreased Known inducers of events may be performed • Sleep deprivation • Suggestion (important in nonepileptic events) Extra electrodes may be added • Sphenoidal • Foramen ovale Methodology Multi-channel long term EEG recording with split screen video recording Digital storage of EEG and video data that can be reviewed later Performed under close monitoring of trained technologists and nurses Study is reviewed by a trained neurologist or epileptologist Outpatient settings Represents a partially controlled environment Useful for: Minor or non-convulsive seizures Diagnostic purposes only Benefits: Less costly Drawbacks: Invasive electrodes not possible No medication withdrawal possible Inpatient settings Completely controlled environment Useful for: Benefits: Major or convulsive seizures Medication withdrawal possible Other tests: Blood sugars, SPECT possible Inducers can be used, if present Invasive electrode monitoring possible Intracranial EEG possible Drawbacks: Expensive Who orders a study? What patients might be candidates? Primarily neurologists order video EEG studies Video EEG can be ordered on infants, children, and adults Indications for video EEG monitoring Common indications: Follow up of borderline or nonconclusive routine EEGs Diagnosis of recurrent spells Classification of seizure type Quantification of interictal epileptiform activity Preoperative evaluation of surgical candidates Evaluation of patient in coma as treatments for status epilepticus Follow-up borderline EEG Allows for prolonged collection of digital EEG Areas of uncertainty (i.e. artifact vs. abnormality) can be correlated with video material for clarification Aids in diagnosis of spells: Causes other than epileptic seizures: Syncope Sleep apnea Periodic movements of sleep Non-epileptic seizures Breath-holding spells Migraine Other uses: Characterization or any repetitive or stereotyped behavior autonomic changes in infants repetitive behaviors in the ICU setting unexplained nocturnal events Characterization of seizures Accurate diagnosis and classification of seizures is essential for proper therapeutic intervention Medication choices are driven by seizure classification Classification of seizure types Generalized Absence Generalized tonic, clonic, or atonic Myoclonic Partial onset Simple or complex Secondary generalization Non epileptic Examples of seizure types Complex partial Generalized tonic-clonic Nonepileptic Complex partial Generalized tonic-clonic Nonepileptic Diagnosis of non-epileptic events: Pseudoseizures Studies1 have shown that 22% of patients with medically intractable seizures studied by video EEG monitoring had nonepileptic events Approximately 1/3 of patients studied at video monitoring centers have nonepileptic events The majority of patients with nonepileptic events have been inappropriately treated with antiepileptic medications for years 1 Matson et al. Nonepileptic events Video EEG monitoring provides evidence to support medication choices • Allows safe discontinuation of antiepileptic drugs Information can be used when discussing a diagnosis of pseudoseizure with patients • Many patients are relieved by diagnosis • Many others are doubtful as they have been told for many years that they have epilepsy This is used to as a treatment modality Nonepileptic events Majority of patients with nonepileptic events also experience epileptic seizures Video EEG can quantitate frequency of each type Aids in education of family members about clinical differences • Avoid abuse of resources • Limit health provider calls • Avoid abuse (overuse) of antiepileptic drugs Quantification of interictal epileptiform activity Quantify the number of seizures per day Helpful for: Absence seizures • Helpful in decision to stop medications Nonconvulsive seizures Document efficacy of suppressive medications Things we don’t like to hear as a passenger. Localization of epileptogenic focus Useful in patients with intractable epilepsy as part of a presurgical evaluation Focus of study is to correlate EEG findings with lesion on MRI Preoperative evaluation of surgical candidates Usually for intractable temporal or extra-temporal epilepsy Can be performed with sphenoidal or foramen ovale electrodes Subdural grid placements can be used in conjunction with a neurosurgeon Evaluation of patient in coma as treatments for status epilepticus Status epilepticus Patients often demonstate continued subclinical seizure discharges after the clinical behaviors have cease EEG monitoring is necessary in all patients in drug induced coma as a treatment for status epilepticus • Need to document burst suppression pattern induced by meds Long term EEG monitoring: Other uses Intraoperatively: Functional stimulation during resections Intraoperative surface EEG monitoring • carotid endarterectomy Other monitoring modalities: Digital ambulatory monitoring Patient wears a digital EEG recorder home Records 24 hours of digital EEG Patient records symptoms in a diary In Summary: Video EEG monitoring Captured 50-96% of epileptic and nonepileptic events (Legatt AD and Ebersole JS, 1998). Established a diagnosis in 88-95% (Legatt AD and Ebersole JS, 1998). Improved outcome in 30-74% of patients (Legatt AD and Ebersole JS, 1998). St. Vincent Hospital EEG – outpatient or inpatient Ambulatory EEG – 24 hour outpatient study Video EEG monitoring Routine 3 adult rooms (hardwired) 1 portable unit (adult or pediatric) 1 ICU monitoring room A neurologist