Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
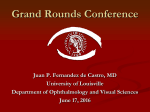
Bullous Pemphigoid: Is prednisone the only option? Wynnie Lau Pharmacy Resident 2010-2011 Medicine Rotation Updated 14 Nov2010 Outline • • • • • Case Background Clinical Question Discussion of evidence Case conclusion/recommendations Case of MK ID 78 yo, 75kg, Caucasian male, NKA living at a care centre CC Large bullae on left arm, thorax, inner thigh and scrotum onset 2wks ago Case of MK HPI 3 August First noticed large brownish bulla in left armpit that was painful and itchy 6 August MD at care centre prescribes hydrocortisone cr applied BID 10 August MD at care centre dx pt with Herpes Zoster and starts Acyclovir 800mg 5x/day X 7days 13 August MD at care centre prescribes diphenhydramine allergy crm applied BID prn 14 August MD at care centre prescribes fucidan 2% cream applied daily 16 August pt admitted to RCH and dx with bullous impetigo and started cephalexin 500mg QID + Probenecid 300mg TID 17 August Pt transferred to VGH CTU blue to be consulted by Derm Case of MK PMHx/ HTN MedsPTA Dyslipidemia Meds at hospital Felodipine 7.5mg daily Atorvastatin 40mg daily Osteoarthritis APAP 325 – 650mg prn T#3 q4-6h prn CVA 2009 resulting in R sided Hemiparesis ASA 81mg daily Ramipril 5mg BID Hypothyroid Levothyroxine 75mcg daily Depression Sertraline 50mg daily Same as @ home but Ramipril held Case of MK Vitals BP 112/72 PE HR88 RR20 O2Sats 96%RA Temp36.7 CNS O x3 HEENT Unremarkable CV S1, S2, no murmur, reg HR, no CP, unremarkable JVP Resp Bilateral air entry, no SOB GI/GU Rash and blisters on abdomen, bullae inner thigh and scrotum Extremities large flacid bullae on left arm and thorax; oozing blood from left arm; rash and blisters on leg and hip Labs WBC 11.4 Na 139 Neut 6.6 Eosino 2.4 K 4.6 SCr 105 HgB 107 INR 1.1 Glucose 6.2 Diagnosis 17Aug 23Aug VGH diagnosis: Bullous Pemphigoid (BP) Pathology finds linear IgG + C3 deposit along basement membrane zone from L upper thigh Bullous Pemphigoid Definition Autoimmune blistering disease Diagnosis Biopsy required for direct immunofluorescence linear deposits of C3 along basement membrane zone found in 100% of pt; IgG found in 65-95% Ref 1, 2, 4 Bullous Pemphigoid Epidemiology Frequently in >65 years old in US 10 per 1 million population Morbidity and mortality Mortality rate ≤ 40% at 1year Pruritus of lesions, pain of ruptured bullae Epidermis loss infections/fluid imbalance Mortality 2o to infection Ref 1, 2, 4 Bullous Pemphigoid Clinical Presentation Urticarial plaques; vescicles and/or bullae Distribution generalized ie. Inner thighs, groin, axillae, flexural Ref 1 Bullous Pemphigoid Causes Precise reason unknown Drug induced BP (Penicillins & furosemide) Goal of therapy Heal existing Reduce new formations Induce remission Ref 3-5 Bullous Pemphigoid Drug induced BP – Reports of 30 medications – Frequently: diuretics and neuroleptics – List include ACEi especially captopril, enalapril – Hypothesis • Drugs change antigenicity to induce synthesis of antibodies against basal membrane zone Ref 5-6 Bullous Pemphigoid Treatment Topical corticosteroids oral corticosteroid (Prednisone 1mg/kg/day) Azathioprine (2-3mg/kg/d) Cyclophosphamide (1-2mg/kg/day) Methotrexate (10-25mg/week) Cyclosporin (6mg/kg/day) Ref 3 MK’s DRPs MK is at risk of adverse events including increased blood pressure and blood glucose secondary to use of systemic corticosteroids and would benefit from a reassessment of his bullous pemphigoid treatment MK’s DRPs • • • • • • • • • MK is at risk for infections secondary to open blisters as a result of his bullous pemphigoid and would benefit from a reassessment of his bullous pemphigoid treatment MK is experiencing continued pruritus secondary to his bullous pemphigoid and would benefit from a reassessment of his bullous pemphigoid treatment MK is experiencing a 14 day history of worsening rash and blisters secondary to his bullous pemphigoid and would benefit from a reassessment of his bullous pemphigoid treatment MK is experiencing continued erythema, blisters and pruritus secondary to improper treatment with cephalexin for his bullous pemphigoid, an autoimmune disorder and would benefit from a reassessment of his bullous pemphigoid treatment MK is experiencing continued erythema, blisters and pruritus secondary to improper treatment with fusidan cream for his bullous pemphigoid, an autoimmune disorder and would benefit from a reassessment of his bullous pemphigoid treatment MK is experiencing continued erythema, blisters and pruritus secondary to improper treatment with acyclovir for his bullous pemphigoid, an autoimmune disorder and would benefit from a reassessment of his bullous pemphigoid treatment MK is at risk of mortality secondary to increased blood pressures due to his held ramipril and requires close monitoring of his blood pressure treatment MK is at risk for deep vein thrombosis clot secondary to being bed bound and immobile and would benefit from a reassessment of his DVT prophylaxis MK is at risk for a cardiovascular event currently taking a statin and would benefit from an assessment of his lipid levels Clinical Question P Elderly patient >65 year old newly diagnosed and active bullous pemphigoid as confirmed by IF studies I Systemic corticosteroid C Other oral and/or topical treatments O Time to resolution of symptoms Adverse effects survival rates Search strategy • Terms: Bullous Pemphigoid, Pemphigoid, Prednisone, methotrexate, azathioprine, cyclophosphamide, cyclosporine • Limits: Humans • Databases: PubMED, Medline, EMBASE, Google – 2 Systematic Review – RCTs – 10 (5 French) – Prospective open label – 5 – Retrospective analysis – 4 Review of Evidence Interventions for bullous pemphigoid (Review) Kirtschig G, Middleton P, Bennett C, Murrell DF, Wojnarowska F, Khumalo NP Cochrane Database Systematic Review 2010; 10. Kirtschig et al. 2010 Studies included 10 RCT, n=1049 Patients Pt of any age treated for BP (confirmed by IF) Interventions Any intervention to treat BP 1o outcome 2o outcome Regression or healing of skin lesions QoL, duration of remission, complications, AE Last search performed 10th August 2010 Heterogeneous data made difficult to pool results Kirtschig et al. • Summary – Starting doses Prednisone >0.75mg/kg/d no added benefit – Prednisone 0.5mg/kg/d may be adequate for disease control – Very potent topical steroids effective however use in extensive disease is limited by practicality and side effects – Additional azathioprine or MMF efficacy unknown – Tetracycline + nicotinamide may be useful – further research Kirtschig et al. Intervention Comparator # of study # of pts Study author Prednisone 1.25mg/kg Prednisone 0.75mg/kg 1 50 Morel Methylprednisolone Prednisone 1 57 Dreno Prednisone + azathioprine Prednisone 2 100 25 Guillaume Burton Nicotinamide + tetracycline Prednisone 1 20 Fivenson Clobetasol propionate cream Prednisone po 1 341 Joly 2002 Mild clobetasol cream standard clobetaosol cream 1 312 Joly 2009 Azathioprine + methylprednisolone MMF + methylprednisolone 1 73 Beissert Controlled trial of azathioprine and plasma exchange in addition to prednisolone in the treatment of Bullous Pemphigoid Guillaume JC, Vaillant L, Bernard P, Pieard C, Prost C, Labeille B, Guillot B et al. Archives of Dermatology 1993; 129:49-53 Guillaume et al 1993 Design Prospective RCT unblinded Oct 1984–Sept 1989, 4 centers Patient N=100, avg 75yo, active pemphigoid, hospitalized, skin biopsy and IF studies to confirm BP Exclusion: localized disease, corticosteroid or immunosuppressive drugs in month, contraindications to study medications Guillaume et al 1993 Comparison Group 1: (n=32) Prednisone 1mg/kg x 4wks ↓ q2wks until 0.5mg/kg @ 3mo ↓ 0.2mg/kg @ 6mo Intervention Group 2: (n=36) Azathioprine 150mg/d (>60kg) or 100mg/d (<60kg) + Prednisone Group 3: (n=32) 4 large volume Plasma exchange in first 2 wks + Prednisone Guillaume et al 1993 Outcomes Follow up – 6months 1) Disease control at 4wks (≤ 1 new blister) & 6months (no new blisters), resolution of erythema and no more than minimal pruritus Guillaume et al. 1993 Prednisone Pred+Aza Controlled N= 31 N = 36 At 1week 39% 44% At 2 week 68% 72% At 3 week 71% 80.5% At 4 week 71% 80.5% At 6 months 42% 39% Relapse 7 10 Death 5 6 Major S/E (including death) 10 15 Pred + Plasma exchange P value NSS Not considered Guillaume et al. 1993 Prednisone Pred + AZA Pred + plasma Total deaths 5 6 3 Severe (incl .death) 10 15 6 4 – cytopenia 3 – hepatitis 1 – MI during procedure Complications 2o to intervention Causes of death • 4 – Pulmonary embolism • 2 – Sepsis • 1 – cerebral stroke • 1 – acute renal failure • 1 – respiratory distress • 1 – wasting syndrome • 3 – unknown reasons Overall death rate 14/98 14.3% at 6months Guillaume et al. 1993 • Summary – “Benefit, if any, of adding azathioprine/plasma exchange to Prednisone 1mg/kg is negligible” – 14/36 Pred vs 13/31 Pred+AZA RR0.93 • Limitations – Trial stopped at interim – Only composite outcome reported A comparison of oral and topical corticosteroids in patients with Bullous Pemphigoid Bullous diseases French Study Group NEJM 2002; 346(5): 321 - 7 Joly et al. 2002 Design P RCT non-blinded 20 centers in France Jan 1996-Dec 1998 Patient N=341, BP confirmed by IF stratified to moderate (<10 new blisters/d) and extensive (>10 new blisters/d) group Exclusion: predominant mucosal involvement, treatment with oral/topical corticosteroids, dapsone or immunosuppressive drugs in previous 6mo Joly et al. 2002 Intervention Moderate n= 153 Extensive n=188 40 g 0.05% clobetasol BID Comparison Prednisone 0.5mg/kg po Outcomes Prednisone 1mg/kg Follow up average 360days 1) Survival 2) Disease control at 3wks (# of new blisters) 3) Complications Joly et al. 2002 Kaplan-Meier estimates of overall survival of pt: p values determined by log rank test Joly et al. 2002 Moderate Topical (n=77) Oral (n=76) Pneumonia 8 Other severe infection (arthritis, cellulitis, peritonitis or septicemia) 3 Diabetes requiring insulin 2 7 MI/ cardiac failure 7 6 Psychosis/delirium 0 Stroke Extensive Topical (n=93) Oral (n=96) P value 11 6 11 NSS 5 2 11 P value P = 0.02 4 13 P =0.04 4 11 NSS 4 0 6 P = 0.03 4 4 7 5 DVT/PE 4 6 5 4 Bone fracture 3 3 2 4 Total 35 29 NSS 27 41 P=0.006 Cumulative hospital stay (day) 11 17 P=0.02 17 25 P=0.002 NSS NSS Joly et al. 2002 Moderate Topical Oral Pt with disease regression at 3 wks 100% Survival rate @ 1yr Extensive P value Topical Oral P value 94% 99% 91% P=0.01 70% 70% 76% 58% P=0.01 Disease Control 21d 100% 95% 99% 91% P=0.01 Complications 38% 32% 29% 54% P=0.006 Disease relapse 35% @ 149d ± 118d 39% @ 178d ± 109d 37% @ 187d ± 118d 46% @ 210d ± 133d NSS Joly et al. 2002 • Conclusions – Prednisone 1mg/kg/d had 1yr mortality rate 41% – In topical treatment – no diff in overall survival – Pt with extensive BP • Topical treatment had 43% RRR in 1 year mortality Joly et al. 2002 • Limitations – – – – Limited AE reported Inconvenient and costly topical regimen Compliance not mentioned Unclear whether new-onset or relapse Back to MK… 18 Aug Started 1mg/kg Prednisone x 5d + clobetasol 0.05% ung BID to affected area 20 Aug no delirium/agitation on dose 22 Aug no new lesions/no pain BG 5-7mmol/L Back to MK… 26 Aug Discharge home Prednisone 55 mg (0.75mg/kg) + clobetasol crm for pruritic or new lesions BID prn Ramipril held to be reassessed (BP~133/71) 27 Aug Decrease to Prednisone 50mg 8 Sept Follow up with dermatology Monitoring Plan Efficacy end points How often? Who? New lesions, bullae, redness Daily Pt, MD, pharmacist, nurse Itchiness Daily Pt, MD, pharmacist, nurse Normalized eosinophilia 2 weeks MD, pharmacist, nurse Disease remission 2 weeks MD, pharmacist, nurse Monitoring Plan Toxicity End points How often? Who? Psychosis/ delirium Daily while at hospital MD, pharmacist, nurse Infection, WBC > 15 with fever Pneumonia Daily while at hospital Daily while at hospital MD, pharmacist Blood pressure control Daily MD, pharmacist Blood Glucose control Daily then weekly MD MD, pharmacist References 1. 2. 3. 4. 5. 6. 7. 8. 9. Goldstein, BG and Goldstein A. Bullous Pemphigoid and other pemphigoid disorders. UptoDate. Last lit review May2010. Lipsker Dan and Borradori Luca. Bullous Pemphigoid: what are you? Urgent need of definitions and diagnostic criteria. Dermatology. 2010. Mutasim, DF. Autoimmune Bullous Dermatoses in the elderly: an update on pathophysiology, diagnosis and management. Drugs Aging. 2010:27(1):1-19. Zhu Yi, Fitzpatrick JE< Kornfeld BW. Lichen planus pemphigoides associated with ramipril. Int J Dermatol. 2006 Dec; 45(12):1453-5. Lee JJ, Downham TF 2nd. Furosemide-induced bullous pemphigoid: case report and review of literature. J Drugs Dermatol. 2006 June; 5(6):562-4. Walsh SR, Hogg D, mydlarski PR. Bullous pemphigoid: from bench to bedside. Drugs. 2005; 65(7):905-26. Rzany Berthold et al. Risk factors for lethal outcome in patients with bullous pemphigoid. Arch Dermatol. 2002; 138: 903-908. Kirtschg et al. Interventions for bullous pemphigoid (review). Cochrane Database of Systematic Reviews 2010; 10. Joly et al. A comparison of oral and topical corticosteroids in patients with bullous pemphigoid. NEJM 2002; 346(5):321-7.