Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
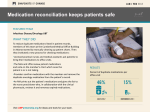
Patient Safety March 5, 2013 Cumberland (GA) ID/Oncology March 5, 2013 Our Team Name Title/Classification Terry Portis, RN Management co-lead Latasha Dixon, MA Labor co-lead, UFCW Local 1996 Angela Peeples, NP Clinician co-lead Sonya Jones LPN Kellye Aschmeyer PharmD Pierson Gladney, Bindu MDs Lingam, Harvey Hamrick Linda Turner, Gwendolyn Brown, Janine Feliciano RNs Darlene Cokley, Julia Siler MAs Bianca Cooper PA Cumberland ID/Oncology Our SMART Goal KP Georgia Cumberland Medical Office Building infectious diseases/oncology department will reduce duplicate medications from a baseline of 46 percent to a goal of 36 percent between August 22, 2011, and November 30, 2011. Our Metrics Measure Data Source Duplicate medications per office visit KP HealthConnect Medications Activity tab Use of discontinue button in HealthConnect Use of reorder button in HealthConnect National Medication Utilization Data Report (weekly) Process Map-BEFORE Start Patient Registers/ Checks In RN/LPN/MA Reviews Medication List with Patient RN/LPN/MA Updates List in KPHC via marking ‘Taking’ or “Not Taking’ MD Reviews List in KPHC with Patient MD Reconciles List in KPHC MD/RN/MA Reviews AVS with Patient Exit Workflow Process Map - AFTER LPN/MA calls patient to bring in Medication Bottles to Office Visit Patient Registers/ Checks In LPN/MA Print out Snapshot of Medications (if needed) RN/LPN/MA Reviews Medication List with Patient in KPHC and notates Snapshot Printout of Duplicates NP/MD Reviews List in KPHC with Patient MD/NP Reconciles List in KPHC and Cleans Up Duplicate Medications & shreds snapshot if applicable RN/LPN/MA Updates List in KPHC via marking ‘Taking’ or “Not Taking’ LPN/MA gives NP/MD List of Duplicate Medications MD/NP Reviews AVS with Patient Exit Workflow Our Successes • Achieved a 67 percent reduction in duplicate medications • The percent of duplicate medications per office visit dropped from 46 percent in July 2011 to 15 percent as of November 2011 • Cost avoidance estimated at $90,000 per three-month period • UBT progressed from a Level 2 to a Level 4 by doing this project Our Challenges • Patients didn’t know/couldn’t accurately describe their medications • Barriers between oncology department and other specialties (such as pharmacy, pain clinic, renal and gastrointestinal) that treat the same patients • Fear of disrupting another specialist’s treatment routine Our Best Practices • Post data in department and analyze in huddles • Build on successful project/workflow from other departments • Encourage patients to use kp.org to monitor their prescription • Involve everyone in the project • Set a goal that stretches your team Our Key Learnings • Increased and improved communication among staff led to more open communication with patients, families • Challenging project strengthened our team Our Rewards & Recognition • Coverage on InsideKP Georgia intranet site • Coverage on LMP website: article, PowerPoint slide, bulletin board poster Questions Questions for the Cumberland ID/oncology team Please use the chat box Send your question to everyone Question #1 Would you like your team to work on a patient safety performance improvement project? Type “yes” or “no” in the chat box Rock Creek (Colorado) GI Team March 5, 2013 Our Team Name Title/Classification/Union Angelina Dale, RN UBT Co-lead, UFCW L7 Jennifer Bias, Endoscopy Technician UBT Co-lead, SEIU L105 Kelly Schuster, RN UBT Co-lead, manager Joseph Cassara, MD UBT Co-lead, physician Our SMART Goal Implement new patient safety protocol within six months to prevent cross contamination between clean and dirty scopes used on patients by March 30, 2012. Background After hearing a news report about how a patient was exposed to dirty scopes, a team member brought the issue to the UBT. They decided to work on the project together to make sure their patients were not exposed to harm. “Although patient to patient exposure is rare, it has devastating effects,” says William Berry, MD. Background Rock Creek GI performs nearly 200 colonoscopies and upper endoscopies a week Equipment is re-used as many as three times per day Tests of change Test of Change Adopt Success Use tags to identify disinfected scopes X The nurse will remove the tag for the doctor Reminder cards on computers to look for blue tags on scopes Adapt Abandon Adjustment Did not work X X Sustaining success Our Best Practices • Collaboration of staff and physician working together as a team to ensure patient safety • Innovativeness to hear something out of the regular environment and consider what could happen in your own department • Spread project to Franklin Medical Office. • The practice is now how we do business Our Challenges • Engagement • Providing the right information • Not having tags in inventory Our Successes Value Compass Award Our Key Learnings • It’s imperative that we explain the “why” of new projects • Involve team members • Let people know ahead of time any changes to processes Questions Questions for Rock Creek GI team Please use the chat box Send your question to everyone Question #2 What will your team’s next step be to improve patient safety? Type your short answer in the chat box. South San Francisco (NCAL) Radiology March 5, 2013 Our Team Insert team picture here From Bob photos Name Title/Classification/Union Tracey Fung 2011 UBT Co-lead, management Derek Granzow 2012 UBT Co-lead, management Donna Haynes UBT Co-lead, labor Our SMART Goal South San Francisco Radiology will reduce “significant” event errors from a baseline of 13 in 2011 to a goal of zero through 2012. “Significant” events are defined as any instance where a patient is unnecessarily irradiated, including incorrect body part, incorrect side, wrong patient, etc. Our Timeline Date Milestone September 2011 Patient safety director approached us to start a Performance Improvement project Invited Radiation Oncology to present their “Stop the Line” project to our UBT October December 2011 UBT did root-cause analysis for all significant events in 2011 Our Timeline Date Milestone Jan. 2012 Determined two key factors leading to significant events: staff feeling rushed and deviation from workflows Feb. – March 2012 Adapted Stop the Line form from the radiation oncology team and created standardized workflow April 2012 Launched Stop the Line at a department “town hall” meeting Workflow Process Map Stop the Line Form Our Best Practices • Review Stop the Line forms at UBT meetings • Track data to identify opportunities for improvement and measure successes • Perform root-cause analysis if similar issues repeat • Collaborate with Risk/Patient Safety department to resolve issues related to other departments impacting radiology Our Challenges • Solving issues outside of radiology that impact our workflows and patient safety. Our Successes • Reduced “significant” events from 13 in 2011 to 5 in 2012 • Since April 2012, 250 Stop the Line forms have been submitted, averting “significant” events before they reached the patient • Empowered staff members to follow the standardized process and stop to do the right thing for a patient’s safety • Improved working relationships with other departments Our Key Learnings • Collaboration with other departments is vital • Data is a powerful tool to: – identify root causes – within and outside the department – communicate and collaborate with other departments that impact patient safety in Radiology • Understand how departments impact each other in the larger system. • Leverage the UBT to do the groundwork for changes in workflows Questions Questions for South San Francisco radiology team Please use the chat box Send your question to everyone Closing Comments Doug Bonacum Vice President of Quality, Safety and Resource Management [email protected] More Resources • Audio and slides from today will be posted on the LMP website • Check out our patient safety videos at http://lmpartnership.org/stories-videos/life-savingteams • Visit the Improvement Advisors – Patient Safety group on IdeaBook for more webinars this week • Thank you to co-sponsors LMP Communications and Department of Care and Service Quality • More virtual UBT fairs coming this year