Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
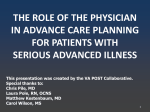
Getting What You Want in End of Life Care Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor and Chair, Department of Geriatrics Florida State University College of Medicine Objectives • Describe the problem of dying in America • Describe common myths about end of life care • Describe steps you can take to control your life – and dying process Remaining Life Expectancy Women Men Walter LC, JAMA, 2001 Causes of Death (>65) • • • • • Heart disease Cancer Stroke Pneumonia Diabetes • • • • • Falls Atherosclerosis Kidney failure COPD Cirrhosis Aging is personally modifiable! Truisms • Everybody’s going to die • Most people don’t want to deal with it • Doctors will always do something, especially when they aren’t sure what to do • The only way to get what you want is to plan for it Common End of Life Medicine • • • • • • Hospitalization No hospice referral Lots of medications Artificial nutrition (“Tube feeding”) Intravenous tubes CPR – cardiopulmonary resuscitation Disease Trajectory Full Function Death 50 80 Artificial Nutrition Myths • • • • Prolong life Reduce suffering Decrease aspiration Ordinary care Prolong Life? • 50%-68% 1 year mortality (Cowen, Callahan) • dementia • stroke • CHF • Survival same as hand fed (Mitchell) • Improvement in nutritional measures does NOT affect survival! (Golden, Kaw, Mitchel) Reduce Suffering? • Complication rate 32% - 70% (Taylor) • Those without hunger or thirst have increased pain with ANH (McCann) • Increased use of restraints • Up to 90% (Peck) • NOT significantly different with G tubes (Ciocon) • 70% had no improvement in function or subjective health status (Callahan) Decrease Aspiration? • NG tube • 67% aspirated • 43% developed pneumonia • 66% pulled out • G tube • 44% aspirated • 56% developed pneumonia • 56% pulled out (Ciocon) Ordinary Care? • Decreased human contact (Slovenka) • Supreme Court ruling in Nancy Cruzan • Religious stands • Catholic - burdens and benefits • Jewish - impediments to dying Loaded Words • Starvation • Dying of thirst • Wasting away Benefits of Dehydration • • • • • • Lack of thirst Decreased phlegm production Decreased urine production Euphoria Analgesia Anaesthetic effect CPR – How Successful? • Television - ? • • • • Majority – trauma 65% children and young adults 75% success rate Rescue 911 - 56% used the term “miracle” • Real life - ? New England Journal of Medicine 334 (24): 1578–1582 CPR in Hospitals • 14% overall survival in hospitals • 3% on general medical wards • 80% of those with restored heart rate are comatose • 50% of survivors do not want CPR again • 50% of survivors develop major depression or functional decline “survival” – leave the hospital CPR in NH • 0%-3% survival rates in NH • 4% of facilities have “No CPR” policies • 23% never initiate - call EMT Definitions • Advance Directives • • • • Living Will Durable Power of Attorney for Health Care Surrogate decision maker Mixed Advanced Directives • 5 Wishes • Advance Care Plan Document – Project Grace • Do Not Resuscitate Order-DNRO (“Yellow Form”) • POLST - an “actionable advance directive” Benefits Of Advance Directives • Discussions between family members • Clarifying preferences • Educating about risks and benefits of different treatments • Dispelling myths • Ensuring desired or preventing undesired treatments? Limitations of Advance Directives • Usually not available in clinical settings • Do not provide clear guidance to emergency personnel • Only 17% - 25% of people have them • Variations in forms • Terms may be unclear to clinicians • Don’t work – SUPPORT study Angela Fagerlin and Carl E. Schneider, “Enough: The Failure of the Living Will,” Hastings Center Report 34, no. 2 (2004): 30-42. Will Better Discussions Work? • SUPPORT Study: • System-level innovation … may offer more powerful opportunities for improvement. • Physician behavior is not altered significantly by addressing poor communication alone. • The fundamental problem may be structural and institutional. Lynn, J. Ineffectiveness of SUPPORT, JAGS, 48: 2000 Murray TH, Improving EOL-Why So Difficult? Hastings Ctr Report, 2005 Why Advance Directives Are Not Followed • Drs (or family) don’t see the patient as hopelessly ill • Contents of the directive are vague • Family member is not available or unable to make the decision • Family members disagree with the person’s choice Teno, J Gen Intern Med, 1998;13:439 Florida Case #1 • Madeline Neuman – 89 y/o Fl nursing home resident completed an AD • Found unresponsive – resuscitated, intubated - 3 granddaughters persuaded Drs to cease treatment – she died after 1 week in Intensive Care Unit • GDs successfully sued Joseph Morse Geriatric Center in West Palm Beach Florida Case #2 • Hanford Pinnette – 73 y/o man in ORMC in Orlando with end-stage heart failure, kidney failure and on a ventilator • Had executed an AD and named his wife as surrogate • Drs recommended ending life-sustaining Tx in accordance with his living will • Wife refused and said she could communicate with him • Hospital went to court and won – LST was stopped and he died FL Living Will - Myths • Only way to limit interventions • Have to fit one of the 3 categories • End stage disease, terminal condition, persistent vegetative state • Must have 2 physicians “decide” • Have to be incapacitated Better Option • Physician Orders for Life-Sustaining Treatment •“POLST” form Purpose of POLST • To ensure that patient preferences are followed • To provide a mechanism to communicate patient preferences for end of life treatment across treatment settings • Home Hospital Nursing home National Use of POLST What is POLST? • A physician order • Can be completed by any provider but must be signed by MD • Complements, but does not replace, other advance directives • Voluntary use, but provides a consistent, easily recognized document Basis of POLST • Discussion regarding advance care preferences • With patient • With surrogate decision maker (or proxy) if patient does not have capacity to make decision • The POLST can be changed by the surrogate, based on proper ethical principles 1 Percentage of Participants Who Received Less, Same, or More Care than Requested . Amount of Care Received Less Than Requested Percent Same as Requested More Than Requested 100% 94% 91% 90% 86% 84% 80% 70% 60% 50% 46% 40% 33% 30% 20% 20% 14% 10% 4% 13% 6% 3% 3% 3% 0% CPR (N=54) 1 Medical Intervention (N=54) Antibiotics (N=28) IV Fluids (N=38) Feeding Tubes (N=34) Areas of Care and Valid Reponses Percentages exclude participants for whom care was not applicab le. Lee, Brummel-Smith, Meyer, Drew, London. J Am Geriatr Soc, 2000; 48:1219 Newest Study • Compared NH residents with POLST to those without one • 1711 residents • Three states – Oregon, West Virginia, Wisconsin Hickman SE, et al. J Amer Geriatrics Soc, 2010 Results – Orders in Chart % 100 90 80 70 60 50 40 30 20 10 0 POLST No POLST Hosp AB ANH CPR Section A: Resuscitation • Resuscitate • Do Not Resuscitate (DNR) • Order only apply if a person is pulseless and not breathing • Some have suggested changing this term to “AND” – Allow Natural Death Section B – Three Levels • Comfort Measures Only • Transfer to hospital only if comfort needs cannot be met • Limited Additional Interventions • Do not use intubation or artificial ventilation, avoid ICU • Full Treatment • Use intubation & ventilation, cardioversion, pacemaker insertion, ICU Sections C and D • Antibiotics • No antibiotics • Evaluate whether limits exist • Use antibiotics • IV and Artificial Nutrition • No nutrition by tube or IV fluids • Use for a defined trial period • Use long term Section E • Basis for Orders • Who was it discussed with? • A summary of the medical condition(s) • Signatures Comfort Measures Always Provided! • Each level of care starts with comfort • Each successive level includes the previous level • Even those receiving “full treatment” need comfort • SUPPORT study – majority of dying patients had untreated, but controllable symptoms Where to Keep the POLST • The front of the chart if admitted • In a red envelop on the fridge (makes it hard to read when in envelope) • Goes with resident (patient) on transfer to another facility • Comes back with resident • Photocopies stay in medical chart (or EHR) after discharge or in physician’s office FL POLST Initiative • Center for Innovative Collaboration of Medicine & Law • Marshall Kapp, J.D., MPH – Director • http://med.fsu.edu/medicinelaw/ • Alyson Odom Program Associate 850-645-9473 • Donations appreciated! References • My Mother, Your Mother: Embracing "Slow Medicine," the Compassionate Approach to Caring for Your Aging Loved Ones • Dennis McCullough • Sick to Death and Not Going to Take It Anymore • Joanne Lynn