Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
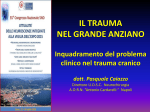
10 yr old F, riding on the shoulders of another child Held onto top of doorframe, then both children fell Pt landed on a wooden floor No LOC, no emesis, no jerking or seizurelike activity, no visible injuries, but parents concerned because patient “just not acting right” No medical conditions No daily medications NKDA No surgeries in the past No history of head injury in the past Pt seen on stretcher, trying to get off of bed, combative with medical personnel, no C-collar in place. A – pt maintaining own airway B – pt breathing without assistance, pulse oximetry > 97% RA, lungs CTA bilaterally without wheezes/rales/rhonchi C – cap refill < 2 seconds, strong distal pulses, nl S1, S2, no murmurs, NSR on monitor D – GCS 14; PERRLA, brisk E – No other signs of trauma Eye Opening › 4 Spontaneously › 3 To voice › 2 To pain › 1 No response Verbal Response › 5 Appropriate words, spontaneous cooing › 4 Inappropriate words › 3 Cries › 2 Incomprehensible sounds, grunts › 1 No response Motor Response › 6 Obeys › 5 Localizes pain › 4 Flexion withdrawal › 3 Flexion abnormal (decorticate posturing) › 2 Extension (decerebrate posturing) › 1 No response Head › Scalp lacerations › Hematomas Cephalohematoma Subgaleal hematoma › Skull fractures Linear Basilar Depressed Nose › CSF rhinorrhea Ears › Battle sign › Hemotypanum › CSF otorrhea Eyes › › › › Pupil size, reactivity EOM Nystagmus Raccoon eyes Patient who has both raccoon eyes and the Battle sign after blunt trauma to the head. Alert, combative, yelling for mother Uncooperative with examination, vital sign measurements Pt fell asleep when not being touched No visible injuries EMV 14 Unable to assess cervical spine tenderness so ccollar placed Decision made to obtain head CT There are more than half a million pediatric head CT scans ordered annually in the United States and rates of neuroimaging for head trauma have doubled over the past decade. However, most children who undergo CT have minor TBI and a negative CT scan. With radiation attributable cancer risk estimated to be as high as 1/2000 in CT exposed children; riskbenefit analyses should be taken into consideration before CT scan of any child with TBI. A great deal of variation in practice exists with respect to neuroimaging after pediatric head trauma. The American Academy of Pediatrics recommends observation of the child with minor closed head injury without LOC and either observation or CT scan for those with LOC A Decision Rule for Identifying Children at Low Risk for Brain Injuries After Blunt Head Trauma, ANNALS OF EMERGENCY MEDICINE 42:4 OCTOBER 2003 Type of Injury No. (% of Children) Cerebral contusion/hemorrhage 50 (51.0) Subdural hematoma 31 (31.6) Subarachnoid hemorrhage 24 (24.5) Cerebral edema 17 (17.3) Epidural hematoma 16 (16.3) *A total of 98 enrolled children had traumatic brain injury identified on CT scan; a combination of injuries was found in 41 of these 98 patients. Note that an isolated skull fracture was not considered a traumatic brain injury. Results: Two thousand forty-three children were enrolled, 1,271 (62%) underwent CT, 98 (7.7%; 95% confidence interval [CI] 6.3% to 9.3%) had traumatic brain injuries on CT scan, and 105 (5.1%; 95% CI 4.2% to 6.2%) had traumatic brain injuries requiring acute intervention. Abnormal mental status, clinical signs of skull fracture, history of vomiting, scalp hematoma (in children ≤2 years of age), or headache identified 97/98 (99%; 95% CI 94% to 100%) of those with traumatic brain injuries on CT scan and 105/105 (100%; 95% CI 97% to 100%) of those with traumatic brain injuries requiring acute intervention. Of the 304 (24%) children undergoing CT who had none of these predictors, only 1 (0.3%; 95% CI 0% to 1.8%) had traumatic brain injury on CT, and that patient was discharged from the ED without complications. Conclusion: Important factors for identifying children at low risk for traumatic brain injuries after blunt head trauma included the absence of: abnormal mental status, clinical signs of skull fracture, a history of vomiting, scalp hematoma (in children ≤2 years of age), and headache. Results similar in 2005 article in Pediatrics. Found significant ICI is unlikely in a child who does not exhibit at least 1 of the highrisk criteria › › › › › › › Evidence of significant skull fx Altered level of alertness Neuro deficit Persistent vomiting Scalp hematoma Abnl behavior coagulopathy Did the child cry immediately after injury? (No crying may indicate loss of consciousness.) Is there a "goose egg" or scalp hematoma present? (Young children who have parietal hematomas are more likely to have an underlying skull fracture.) Was there bleeding or fluid draining from the nose or ears? (A "yes" answer may indicate the presence of a basilar skull fracture.) Was the fall greater than 3 feet? (A "yes" answer indicates increased risk of skull fracture in infants.) How old is the child? (Infants are at increased risk for skull fracture and intracranial injury.) Has the child had a recent head injury? (A second head injury to a now symptomatic child may result in increased morbidity.) Examination of the child is warranted if an answer to any of these questions confirms a risk for significant head injury. If answers to the questions do not indicate a risk for a significant head injury, the parents should be counseled to supervise the child closely up to 24 hours after the time of injury and to contact the physician if there is any change in the child's mental status or any seizures, persistent or increasing headache, or protracted vomiting (more than two to three episodes). Head CT normal Pt still combative when aroused, still refusing food and drink Diagnosed with concussion Decision made to admit to hospital for observation Pathophysiologic process resulting in the self-limited impairment of neurologic function that has an associated set of clinical symptoms Symptoms usually acute in onset, result of functional rather than structural disturbances Estimated that up to 25% of pts with minor head trauma develop a concussion Headache Dizziness Depression Confusion Nausea/vomiting Sensitivity to light or noise Anxiety Poor memory Lethargy Slow response to questions Decreased energy Irritability Blurred or double vision Poor concentration Poor balance Insomnia Severity Symptoms Management Grade 1 (Mild) No LOC, ringing, headache, dizziness, or memory loss Observation May not return to competition until symptom-free upon exertion Grade 2 (Moderate) LOC <5 min or PTA >30 min Grade 3 (Severe) Observation May not return to competition for 1 wk after symptom-free upon exertion LOC >5 min or PTA >24 h Admit Refer for neurocognitive testing prior to resumption of contact sports LOC=loss of consciousness; PTA=posttraumatic amnesia Car seats Proper helmet use Never allowing infants to be unsupervised on tables/beds/etc. Keep side rails up on cribs, lowering mattress when child pulls to stand Gate to stairways Forbid trampolines A Decision Rule for Identifying Children at Low Risk for Brain Injuries After Blunt Head Trauma, ANNALS OF EMERGENCY MEDICINE 42:4 OCTOBER 2003 Pediatric Minor Closed Head Injury, Pediatr Clin N Am 53 (2006) 1 – 26 Prehospital Evaluation and Management of Traumatic Brain Injury in Children, Clin Ped Emerg Med 7:94-104 Pediatric Head Injury, Peds in Review, Pediatr. Rev., Jun 2007; 28: 215 - 224. CLINICAL PRACTICE GUIDELINES PEDIATRICS Vol. 104 No. 6 December 1999, pp. 1407-1415 AMERICAN ACADEMY OF PEDIATRICS: The Management of Minor Closed Head Injury in Children Committee on Quality Improvement, American Academy of Pediatrics Pediatric Advisor 2006 Thanks to Dr. Craig Carter