Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
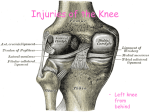
MCL Injuries Dr. David Vasconcellos Sports Fellow University of Iowa Sports Medicine Center The Latest and Greatest Evidence Based Case 17 y/o male tackled at his left knee from the outside while playing intramural football. Knee buckled inward. Felt a pop in his knee, limped off the playing field. Case PE Stiff Knee Gait Mild Effusion No Joint Line TTP +TTP over femoral insertion of the MCL Negative Lachman, Negative Anterior and Posterior Drawer. Negative McMurrays Varus and Valgus stable in extension. Moderate laxity in 30 degrees of flexion with valgus stress with firm endpoint. Case XR: Negative Case Diagnosis? Case Grade II MCL Tear Case Treatment Conservative Treatment. Crutches Anti-inflammatories ROM Brace Rehab Outcome RTP in 4 weeks, weaned as tolerated from brace. Anatomy Layer I Layer II Deep fascia, Sartorius Superficial MCL Layer III Deep MCL Posteromedial Capsule Medial Knee Anatomy MCL Function Primary stabilizer to valgus force. Secondary stabilizer to Anterior translation. Resist external rotation. MCL and ACL have a codependent relationship. Diagnosis History Classic Mechanism: Isolated Valgus moment to knee. PE Complete Knee Exam Examine MCL with the knee both in full extension and at 30 degrees of flexion. Valgus Stress with knee at 30 degrees of flexion causes pain or instability of medial knee. MCL Injury Model MCL Grading System I - Stretching of fibers. Localized TTP. No instability. II - Disruption of Fibers. Mild to moderate instability. III - Complete disruption of ligament. Gross instability. Imaging XR May demonstrate avulsions. MRI Confirms Diagnosis Evals other ligaments, cartilage. Treatment The injured MCL heals predictably without repair regardless of its grade. Non-op management of all MCL tears is considered standard practice. Treatment of Isolated MCL Injury Grade I and II Injuries Non-Surgical Treatment Crutches until symptoms improve, WBAT, ROM. Edema Control - Ice, Compression, Massage. NSAIDS Hinged knee brace Speeding Recovery Good control of swelling can decrease the amount of time for full recovery of motion and strength. Treatment of Isolated MCL Injury Grade III MCL Non-Surgical Rehab Brief period of immobilization Start ROM when initial swelling subsides. May need a longer period of protected weight bearing. Persistant valgus instability May consider for early surgical reconstruction. Tibial Sided vs. Femoral Sided MCL injury Proximal MCL tears at the femoral insertion more common than at the distal tibial insertion. In general, femoral side injuries tend to heal better than tibial side or midsubstance injuries. QuickTime™ and a TIFF (Uncompressed) decompressor are needed to see this picture. ACL + MCL Usually do not require MCL reconstruction Rehab the medial side and achieve full ROM then do ACL reconstruction. However, if valgus instability persists after rehab then reconstruction of ACL and MCL should be considered. PCL + MCL If significant posterior subluxation is present following injury, both ligaments should be reconstructed acutely. If the Joint is well reduced, can treat MCL nonsurgically with bracing. PCL can be reconstructed when full ROM is achieved and valgus stability is restored. If valgus instability persists, reconstruct PCL and MCL. Chronic MCL Injury Chronic injury results when the MCL complex loses its potential for spontaneous healing. Usually occurs 3 to 4 months following the initial injury. Can develop secondary ligamentous instabilities or secondary limb malalignment. Chronic MCL Injury Valgus deformity of limb secondary to chronic MCL Osteotomy may be required at time of MCL reconstruction. Surgical Options POL Advancement Proximal Capsular Advancement Distal Capsular Advancement Semimembranosis advancement Allograft Child with Medial Knee Injury Don’t forget to rule out physeal injury! Prevention Prophylactic and Functional Bracing for MCL Protection Controversial Latest Research Animal Studies suggest that AntiInflammatory medications do not impede ligament healing in early and intermediate healing phases Sports Med. 1999; 27; 738. Claude T. Moorman, III, Udita Kukreti, David C. Fenton and Stephen M. Belkoff. The Early Effect of Ibuprofen on the Mechanical Properties of Healing Medial Collateral Ligament ACL + MCL Operative and Nonoperative Treatments of Medial Collateral Ligament Rupture Were Not Different in Combined Medial Collateral and Anterior Cruciate Ligament Rupture. Review ACL + Grade 3 MCL Surgery at 4 - 23 days after injury. No difference in results at 2 years. Surgery took place before MCL healing. Low Demand Patients Treated with continuous hinged knee brace Conclusion: Patients with combined ACL + MCL injuries who undergo early surgery after injury may do well without surgical treatment of the MCL, but they should be treated in a hinged knee brace. Caution should be used in a different patient population such as high demand athletes. Halinen J, Lindahl J, Hirvensalo E, Santavirta S. Operative and Nonoperative Treatments of Medial Collateral Ligament Rupture with Early Anterior Cruciate Ligament Reconstruction: A Prospective Randomized Study. Am J Sports Med. 2006 Jul;34:1134-40. Questions?