Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
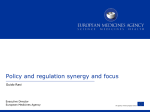
DEVELOPING GLOBAL ROAD MAPS FOR REIMBURSEMENT PROCESSES USED IN HEALTH TECHNOLOGY ASSESSMENT: PHARMACEUTICALS, MEDICAL DEVICES, AND DIAGNOSTICS Noreen J. 1 Sullivan , 2 Szeinbach , 2 Seoane-Vazquez , 3 Matuszewski , Sheryl L. Enrique C. Karl A. 6 7 8 Stefan Holmstrom , Geoffrey Wilson , Annie Chicoye Kevin W. 4, 5 Mayo , 1Resonance Health Analysis Services Pty Ltd, Encinitas, CA, CA, USA, 2Ohio State University, College of Pharmacy, Columbus, OH, USA, 3 Gold Standard/Elsevier, Tampa, FL, USA, 4Bridgehead International, New York, New York, USA, 5University of the Sciences in Philadelphia, PA, USA, 6Astellas Pharma Europe, HEOR, Leiderdrop, Netherlands, 7GE Healthcare, Buckinghamshire, UK, 8IMS Consulting, Puteaux Cedex, France Figure 1. HTA Decision and Reimbursement Process Model Template BACKGROUND Country Health technology assessment (HTA) is used to evaluate health care technologies (e.g., pharmaceuticals, medical devices, and diagnostics) with respect to cost and their projected impact on patient outcomes and society. Currently, there is an ongoing initiative by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) to develop Road Maps that describe the utilization of HTA in health care. The first part of this project described the decision makers and the decision-making process for HTA in several countries. The second part of this project adds the reimbursement process for products and devices approved through the HTA process. *Leading Payer Organization Step 1 Step 2 OBJECTIVE: The purpose of this study was to extend the model for HTA decision-making structures to include reimbursement road maps for several countries. Step 2a METHODS DATA COLLECTION & STRATEGY: Members of the of the ISPOR Special Interest Group (SIG) contacted key individuals in several countries including: Austria, Denmark, France, Hungary, Ireland, Spain, Taiwan, and UK. Pharmaceuticals, medical devices, and diagnostics were used as the framework for our research. The completed decision model template presented in Figure 1 includes the decision maker, the decision-making process, data requirements, and reimbursement processes for each country. The criteria used included: • Decision Maker: Payer (person or organization) who makes final decision for coverage and payment of product. • Evaluator/Advisor: Person or organization who provides input into the decision-making process via HTA development and/or review but does not make final decision for coverage and payment. • Decision-Making Process: HTA evaluation process, as defined in the public domain, for new and emerging technologies. • Reimbursement Process: Describes the strategy for coverage and payment of approved pharmaceuticals, medical devices, and diagnostics. VALIDATION: Once models were completed, they were forwarded to a contact affiliated with each Payer organization to confirm their accuracy. Key Decision Maker (Primary & Secondary) Evaluator/Advisor (Person/Organization) Approved Step 3 Not Approved Formulary or Approved Products Step 4 List Step 5 Reimbursement Additional Evaluators/Advisors *Leading Payer Organization: The top 3 payer groups covering the majority of the population. Table 1. Summary of Reimbursement Processes for HTA in Target Countries Country Austria Denmark France Hungary Ireland Key Decision-Makers Primary Secondary Federal Ministry of Health, Family & Youth (BNFGJ) Danish Medicines Agency (DKMA) Ministry of Health & Union for Health Insurance (UNCAM) National Health Insurance Fund Administration (NHIFA) The Health Services Executive (HSE) Spain Central Government Taiwan Bureau of National Health Insurance (BNHI) National Institute for Health and Clinical Excellence (NICE) UK Evaluator Role Primary Pricing Committee (PK) Main Association of & Independent Drug Austrian Security Commission (UHK) Institutions (HBV) Reimbursment Committee (MTN) Comité Economique des High Health Authority (HTA Produits de Santé public Agency) (CEPS) Technology Appraisal Committee (TAC) Secondary Pharmaceutical 100%: Patient copayment capped at 2% of patient annual income Evaluation Board (HEK) Hospital Committees for medical devices and drugs Office of Health Technology Assessment (OHTA) Corporate Pharmaceutical National Centre for Unit (CPU) Pharmacoeconomics (NCPE) Regional Government European Medicines Ministry of Health Agency (EMEA); Spanish (MSC) Medicine Agency (AEMPS) Center for Drug Evaluation (CDE) National Coordinating Centre for HTA (NCCHTA) Reimbursement Payment Varies with respect to patient accumulated expenditures Most products reimbursed at 65%. Products for chronic/severe disease are reimbursed 100 % . 2007 average was 76.77% for retail pharmacy Drugs classified by category Drugs approved by Community Drug Schemes are100% reimbursed Reimbursed medications are on a national reimbursement list: 100% for hospital pharmaceuticals; 90% for pharmaceuticals used to manage chronic illness; 60% prescription only pharmaceuticals Reimbursement determined by 1) listing 2) restrictions for coverage, and 3) new reimbursement price Patient co-pay is usually less than 18% based on total cost of drug Branded drug price set by Pharmaceutical Price Regulation Scheme (PPRs) drug is reimbursed by NHS according to manufactuer list price RESULTS For the most part, reimbursement and payment processes for new and emerging technologies parallel the overall HTA process. Key decision makers and Evaluators play an important role in the reimbursement process for HTA and ultimately, influence Key Decision Makers in the acceptance of new and emerging technologies (Table 1). While pathways for reimbursement and coverage varied across countries, we were able to define key characteristics that defined the reimbursement process for the review and approval of new and emerging technologies in countries around the world. For these countries, reimbursement and payment decisions were the responsibility of decision makers who were either closely connected to the Key Decision Maker or who served as a primary decision maker for HTA. Reimbursement and payment levels varied across countries, with levels of reimbursement based on annual income, co-payment, drug categories, or a pre-determined percentage. Other Advisory entities consisted of various committees and agencies that provided economic evaluations as part of their responsibilities to the Key Decision Makers or provided input upon request as an independent or contracted entity. In summary, the process for reimbursement and coverage of new and emerging technologies in the countries examined was fairly centralized and organized within the overall HTA process. CONCLUSION This study was designed to characterize and present the reimbursement process for HTA in several countries with respect to Key Decision Makers, Evaluators, Advisors and the decisionmaking process. Although the reimbursement processes for HTA contained features that are common across the countries examined, the coverage and payment mechanisms varied within each country. Future research will focus on the addition of other countries with respect to decision-making and reimbursement processes and how data are used to determine pricing and reimbursement levels for new and emerging technologies. ACKNOWLEDGEMENT We would like to thank the members of the ISPOR Special Interest Group for Global Health Care Reimbursement Systems and Decision Processes with special thanks to Randa F. Eldessouki, Nadia G. Naaman, and Marilyn DixSmith, PhD.