Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
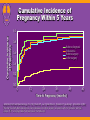
Inflammatory Bowel Disease: Overview IBD: Overview 1CCFA Prevalence: ~250 cases per 100,0001 – More than 1 million cases estimated in United States1 – Ulcerative colitis (UC): 50%1 – Crohn’s disease (CD): 50%1 Incidence: 15 cases per 100,0001 – Onset: 30% between 10 and 19 years of age2 – Young children: <2%2 – Peak age of onset: 20s & 30s, again in 60s3 – Slightly greater risk for women and elderly4 100 80 60 East 40 West 20 North 0 1st Qtr 2nd Qtr 3rd Qtr 4th Qtr Library: Basic Facts. Available at: http://www.ccfa.org. 2Grand RJ, et al. Clin Invest Med. 1996;19:373-380. 3Hanauer SB. Cecil Textbook of Medicine. 20th ed. Philadelphia, Pa: WB Saunders Co; 1996:707. 4Lashner BA. In: Stein SH, Rood RP, eds. Inflammatory Bowel Disease: A Guide for Patients and Their Families. 2nd ed. Philadelphia, Pa: Lippincott-Raven Publishers; 1999:23-29. IBD: Overview (cont’d) Scope of disorder (United States) – 700,000 physician visits per year – 100,000 hospitalizations per year – CD accounts for two thirds Long-term outlook – Chronic, lifelong disease – Acute flare-ups alternating with remission – Complications and increased mortality – Surgery for 50% to 80% of CD patients Calkins BM. Digestive Diseases in the United States: Epidemiology and Impact. Bethesda, Md: National Institutes of Health; 1994. Risk for Developing CD Empiric Risk for Developing Crohn's Disease (%) 60 50 50.0 40 37.0 30 20 16.8 10 0 7.5 Offspr Both Parents MZ Twin Sib Ashk Jew 7.4 7.0 Offspr Ashk Jew Parent 4.6 <4.0 Sib Non-Jew DZ Twin <0.2 0.1 Heterozygote NOD2 Homozygote NOD2 General Population IBD: Systemic Complications Eye inflammation* Lower bone density* Liver and bile duct inflammation Gallstones Skin lesions *Higher incidence in women. Growth failure in children Kidney stones Subfertility* Ovaries Uterus Arthritis and joint pains Influence of Gender on Illness-Related Concerns in IBD Study of 343 men and women – Women report higher levels of symptom severity (P=.04) – Higher levels of rating of IBD patient concerns (P<.001) Maunder R, et al. Can J Gastroenterol. 1999;13:728-732. Patients’ Concerns in IBD Greater in Women Than in Men – Feelings about body – Attractiveness – Feeling alone – Having children – Intimacy (CD) – Sexual performance (CD) Maunder R, et al. Can J Gastroenterol. 1999;13:728-732. Independent of Gender – Energy level – Medication effects – Uncertain nature of IBD – Having surgery – Having ostomy bag – Reaching full potential – Being a burden Gender-Related Considerations in IBD Women Reproductive issues fertility after IPAA or proctocolectomy risk of relapse if disease active at time of conception Disease-related concerns Sexuality concern re: body stigma, loss of bowel control Men fertility with sulfasalazine Sperm count with methotrexate — sexual activity libido and sexual because of dyspareunia, satisfaction after abdominal pain, etc proctocolectomy The Effect of Smoking on Crohn’s Disease in Women There are now two studies that have specifically addressed the gender effect of tobacco Women smokers undergoing surgery are 5 times more likely to have a recurrence than a non-smoker, and recur more quickly1 Women smokers hastened onset of disease and increased the need for immunomodulators2 1Kane SV, Gastroenterol 2002; 124(5):A1169 2 Cosnes J Clin Gastro and Hepatol 2004;2:41-48. Special Considerations for Women With IBD Special Considerations for Women With IBD Cervical Dysplasia Menstruation/contraception Body image/sexuality Conception/pregnancy/breast-feeding Menopause/hormone replacement therapy Risk of osteoporosis Adherence – Physician-patient partnership Overlapping IBS Incidence of Abnormal Pap Smears in IBD Abnormal Pap smears associated with both infection and progression to cancer Incidence study of women with IBD and a history of abnormal Pap smears Adjusted for smoking, OCP use and parity Women with IBD were more likely to have an abnormal Pap Use of azathioprine increased risk 3 fold Kane SV Am J Gastro 2008;103(3):631-6. IBD: Issues With Menstruation and Contraception Menstrual Cycle and Bowel-Pattern Fluctuations Bowel-pattern fluctuation is common during the menstrual cycle IBD symptoms may increase during the menstrual cycle Suppression of menses via hormonal contraceptive methods may be considered in presence of debilitating symptoms Potential IBD-Related Menstrual Symptoms Most frequently reported symptoms – Pelvic pain 52% – Lower back pain 36% – Diarrhea 26% – Irritability 23% – Headache 20% Incidence of any menstrual symptoms significantly higher for IBD patients than for healthy controls (P.01) Kane SV, et al. Am J Gastroenterol. 1998;93:1867-1872. IBD: Issues With Menstruation There is a trend for patients with CD to be affected by IBD symptoms during menstruation to a greater extent than are patients with UC CD patients experienced diarrhea significantly more often than did controls (P=.004) Kane SV, et al. Am J Gastroenterol. 1998;93:1867-1872. OCs and IBD Risk Controversial data Increased incidence of CD with use of OCs? OCs related to flare of CD activity? Newer OCs with lower estrogen content associated with decreasing incidence of CD in women? CD Flare and OCs Patients With Flare (%) 60 50 40 OC use No OC use 30 20 10 0 0 100 200 300 400 Days After Inclusion Adapted from Cosnes J, et al. Gut. 1999;45:218-222 with permission from BMJ Publishing Group. 500 OCs and IBD Risk F:M Incidence Ratio 2.5 2.0 Baltimore F:M incidence for 20-29-year age group 1.5 Olmstead F:M incidence for 20-29-year age group 1.0 US OC use (5 million) 0.5 0.0 1960 1965 1970 1975 1980 1985 1990 Adapted from Alic M. Gut. 2000;46:140 with permission from BMJ Publishing Group. Contraindications for OCs History of thromboembolic disease Active obstructive liver disease with elevated liver enzymes Breast cancer Smokers over the age of 35 Pregnancy IBD and Contraception: Conclusions OCs should have lower estrogen content (eg, 35 µg) Avoid for women with known hypercoagulability Avoid for women with IBD-associated liver disease Avoid for women with IBD who smoke IBD: Issues With Body Image and Sexuality IBD and Sexuality: Physical Impact Impact of disease – Perianal complications – Draining cutaneous fistulae – Skin lesions – Arthritic deformities – Pain – Fatigue Impact of treatment – Surgical scars – Stoma – Medication side effects IBD and Sexuality: Psychological Impact Affected aspects – Behavior patterns – Communication – Sexual drive – Sensations connected with sexual activity Negative effects – Feeling dirty, unsexy, unattractive – Reduced self-esteem – Loss of former identity – Anxiety over disclosure Maintaining Femininity Following IBD Surgery Body image Sexuality Communication Fertility Pregnancy Sexual Function Following IPAA Usually improved because of improved general well-being Some problems may continue – Dyspareunia – Vaginal drying Sexual function improved 16%-25%1,2 Frequency of intercourse increased 35%2 IPAA = ileal pouch-anal anastomosis. 1Farouk R, et al. Ann Surg. 2000;231:919-926. 2Damgaard B, et al. Dis Colon Rectum. 1995;38:286-289. Women With Restorative Proctocolectomies: Satisfaction With Sexual Relationships 22% improved 51% unchanged 26% less satisfactory Overall 86% moderately to extremely satisfied Bambrick M, et al. Dis Colon Rectum. 1996;39:610-614. Gynecologic Function Before and After IPAA Results of Questionnaire (n=110)1 Before After Dyspareunia* 5% 15% Fecal incontinence during intercourse 3% 7% Menstrual problems 23% 31% *Rates range from 0% to 26%.2-5 1Counihan TC, et al. Dis Colon Rectum. 1994;37:1126-1129. 2Tiainen J, et al. Scand J Gastroenterol. 1999;34:185188. B, Peppen B. Acta Obstet Gynecol Scand. 1995;74:51-55. 4Damgaard B, et al. Dis Colon Rectum. 1995;38:286-289. 5Bambrick M, et al. Dis Colon Rectum. 1996;39:610-614. 3Sjogren Women With Ileostomies: Sexual Function % Patients No change 47% Adversely affected – Mild (22%) – Severe (14%) – Moderate (11%) 47% Improved Awad RW, et al. Br J Surg. 1993;80:252-253. 7% Women With Ileostomies: Sexual Concerns (n=50) Sexual attractiveness decreased 52% – Appliance 72% – Stoma 16% – Odor 4% More women (60%) than men (52%) felt less desirable Sexual intercourse is more difficult – Psychologically 46% – Physically 32% Rolstad BS, et al. Dis Colon Rectum. 1983;26:170-171. Conception and Fertility in Women With IBD Effects of IBD on Fertility Women – UC: normal fertility rate overall (92.2%)1,2 • IPAA reduces fertility – CD: normal fertility, but pelvic inflammation may block fallopian tubes3 – Voluntary childlessness higher for IBD patients4 Men – Reversible sperm abnormalities with sulfasalazine5 – Azathioprine: Semen analysis normal with immunomodulators6 – Methotrexate caused temporary low sperm count in animals7 1Willoughby CP, Truelove SC. Gut. 1980;21:469-474. 2Kane SV. In Kirsner JB, Shorter RG, eds. Inflammatory Bowel Disease. 4th ed. 1995. 3Järnerot G. Scand J Gastroenterol. 1982;17:1-4. 4Baird DD, et al. Gastroenterology. 1990;99:987-994. 5Kornbluth A, Sachar DB. Am J Gastroenterol. 1997;92:204-211. 6Rajapakse RO, et al. Am J Gastroenterol. 2000;95:684-688. 7Johnson FE, et al. J Surg Oncol. 1994;55:175-178. Effects of CD on Female Fertility: Conflicting Findings 1Fielding In 5 studies, inability of patients to conceive because of CD ranged from 12% to 67%1-5 Risk of inability to conceive was higher in patients with large-bowel disease than in those with small-bowel disease1-4 – Difference sometimes significant1 – No difference5 Chances of conceiving increased after surgery for CD2 JF, Cooke WT. Br Med J. 1970;2:76-77. 2De Dombal FT, et al. Br Med J. 1972;3:550-553. 3Homan WP, Thorbjarnarson B. Arch Surg. 1976;111:545-547. 4Khosla R, et al. Gut. 1984;25:52-56. 5Mayberry JF, Weterman IT. Gut. 1986;27:821-825. Female Fertility After IPAA (n=343) Fecundability Ratio Reference population Patients before diagnosis Patients before colectomy Patients after IPAA P Value 1 Number of Menstrual Periods Observed (time to pregnancy) 914 1.46 98 .002 1.01 84 .92 0.20 149 <.0001 — Adapted from Gastroenterology, Vol 122, Olsen KØ, Juul S, Berndtsson I, Öresland T, Laurberg S, Ulcerative Colitis: Female Fecundity Before Diagnosis, During Disease, and After Surgery Compared with a Population Sample, pages 15-19, Copyright 2002 with permission from Elsevier. Cumulative Incidence of Pregnancy Within 5 Years Cumulative Incidence of Pregnancy 1.0 0.8 Before diagnosis Reference Before surgery After surgery 0.6 0.4 0.2 0.0 0 12 24 36 48 60 Time to Pregnancy (months) Adapted from Gastroenterology, Vol 122, Olsen KØ, Juul S, Berndtsson I, Öresland T, Laurberg S, Ulcerative Colitis: Female Fecundity Before Diagnosis, During Disease, and After Surgery Compared with a Population Sample, pages 15-19, Copyright 2002 with permission from Elsevier. Surgical Approaches to Minimize Infertility Possibly delay pelvic surgery Minimize septic complications Decrease adhesion formation – Ferric hyaluronate adhesion-prevention gel – “Pexing” ovaries Laparoscopic procedures IBD and Conception: Summary Close to normal fertility with UC, decreased after IPAA Conflicting findings regarding influence of CD on ability to conceive Conflicting findings regarding influence of surgery for CD on ability to conceive Some IBD treatments may cause sperm abnormalities in men Pregnancy and Pregnancy Outcomes in Women With IBD Effects of IBD on Pregnancy Outcomes Preterm birth – risk in both UC and CD1,2,5 4 of 5 studies: no major impact on risk of congenital abnormalities1-5 Significant in risk of low birth weight2-5 1Baird risk of maternal/delivery complications5 DD, et al. Gastroenterology. 1990;99:987-994. 2Dominitz JA, et al. Am J Gastroenterol. 2002;97:641-648. RJ, Stirrat GM. Br J Obstet Gynaecol. 1986;93:1124-1131. 4Fonager K, et al. Am J Gastroenterol. 1998;93:2426-2430.4Mahadevan U, et al. Gastroenterol. 2007;133:1106-1112 3Porter Meta-analysis 12 studies – N= 3907 (CD 1952, UC 1113) vs. 320, 531 Prematurity OR = 1.87 (1.52-2.31) p<0.001 LBW OR = 2.10 (1.38-3.19) , p<0.001 C-section OR = 1.50 (1.26-1.79) p <0.001 Congen Abnorm. = 2.37 (1.47-3.82) p <0.001 – 4 studies reported on the incidence IBD vs. controls, no difference – UC vs. controls in two studies (Larzilliere 1998, Dominitz) Cornish Gut 2006;0:1-8. Effect of Pregnancy on UC: Disease Activity at Conception 80 70 n=528 66 n=227 Percent 60 50 45 40 34 30 24 27 20 10 0 No Relapse Relapse Inactive Miller JP. J R Soc Med. 1986;79:221-225. Worsened Continued Decreased Activity Activity Activity Active Effect of Pregnancy on CD: Disease Activity at Conception 80 73 n=186 70 n=93 Percent 60 50 40 27 30 33 32 34 20 10 0 No Relapse Relapse Inactive Miller JP. J R Soc Med. 1986;79:221-225. Worsened Continued Decreased Activity Activity Activity Active Disease activity during pregnancy in women with IBD Percentage of patients Majority of patients have inactive to mild disease during pregnancy 100 80 60 40 20 0 Disease activity in Crohn’s disease Inactive Mild 100 80 60 40 20 0 Disease activity in ulcerative colitis Moderate Severe Concept T1 T2 Mahadevan U, et al. Gastroenterol. 2007;133:1106-1112 T3 PP Trimester Effect of Pregnancy on IBD: Maternal-Fetal HLA Disparity Prepartum disease activity significantly predicts disease activity during pregnancy (P=.008) In single-locus disparity, no significant difference between DR and DQ prepartum, during trimesters 1-3, or postpartum Disparity at both DR and DQ loci significantly predicts disease activity during pregnancy (P=.001) Maternal immune response to paternal HLA antigens may play role in pregnancy-induced remission of IBD Kane S, et al. Gastroenterology. 1998;114:A1006. Abstract G4121. Concerns Regarding Pregnancy and Delivery What is the effect of pregnancy on pouch function before and after delivery? Should the woman deliver vaginally or have cesarean section? Are there unique concerns if cesarean section is performed? Delivery Mode and Perineal Injury Study indicates that more women with IBD have cesarean sections1 Vaginal delivery is usually safe for women with inactive perianal symptoms1 1Ilnyckyji A, et al. Am J Gastroenterol. 1999;94:3274-3278. Pouch Function During and After Pregnancy 10 vaginal deliveries, 6 cesarean sections – No pouch complications 8.1 bowel movements/day during pregnancy vs 6.5/day postpartum 3 women had incontinence during pregnancy, 1 frequent and 2 mild 1 woman had nighttime incontinence postpartum Scott HJ, et al. Int J Colorectal Dis. 1996;11:84-87. Pregnancy, Delivery, and Pouch Function After IPAA in UC Questionnaires sent to women with IPAA for UC Results – 49 deliveries for 29 women (25 vaginal, 24 c-sections) – 6 pouch-related complications (2 during pregnancy; 4 postpartum) – stool frequency and incontinence during pregnancy – 83% regained prepregnancy function; 17% had some permanent pouch function deterioration not related to delivery method – Delivery method did not affect incontinence, stool frequency Conclusion: Pregnancy is safe for women with IPAA Ravid A, et al. Dis Colon Rectum. 2002;45:1283-1288. IBD in Pregnancy: Summary Pregnancy outcomes best if patient in remission at time of conception, though even patients in remission can have higher rates of adverse outcomes compared to the general population IBD increases the risk of preterm birth and low birth weight and maternal complications No significant increase in risk of congenital abnormalities Women with IBD have a higher rate of cesarean sections Pregnancy may not increase the risk of relapse or significantly increase disease activit Management of IBD in Pregnancy Assessment of Disease Activity in Pregnant IBD Patients Laboratory studies (ESR, Hgb, albumin, CRP) Ultrasound – low risk Low-dose X-rays pose minimal fetal risk1 Endoscopy – low risk if used for appropriate indications2 Flexible sigmoidoscopy – low risk2 Colonoscopy – should only be used for life-threatening colonic disease or when only alternative is laparotomy2 ESR = erythrocyte sedimentation rate; Hgb = hemoglobin; CRP = C-reactive protein. 1Hufton AP. Br J Radiol. 1979;52:735-740. 2Cappell MS, et al. Dig Dis Sci. 1996;41:2353-2361. Drugs in Pregnancy Pharmaceutical companies almost never test products in pregnant women PDR® disclaimer: use in pregnancy is not recommended unless benefits justify risk to fetus FDA classifications (A, B, C, D, X) – Ambiguous – Difficult to interpret and use in counseling PDR® = Physicians’ Desk Reference®; FDA = Food and Drug Administration. Koren G, et al. N Engl J Med. 1998;338:1128-1137. Pregnancy-Risk Categories A: Controlled human studies do not show risk to fetus; chance of risk remote B: No evidence of risk to fetus in human studies; chance of risk remote but possible C: Inadequate studies in humans; risk cannot be ruled out, but benefits may outweigh risks D: Positive evidence of fetal risk; benefits might outweigh risks in life-threatening situations when safer drugs are ineffective X: Contraindicated in pregnancy Briggs GG, et al. Drugs in Pregnancy and Lactation. 5th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 1998. Summary: Safety of IBD Medications During Pregnancy Category B Category C Category D Category X Loperamide Ciprofloxacin Azathioprine† Methotrexate Mesalamine Cyclosporine 6-Mercaptopurine† Thalidomide Balsalazide Diphenoxylate Corticosteroids Olsalazine Sulfasalazine Tacrolimus Anti-TNF agents Natalizumab Metronidazole* *Safe for use after first trimester. †Increasing use in pregnancy. Briggs GG, et al. Drugs in Pregnancy and Lactation. 5th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 1998. Physician’s Desk Reference®. 57th ed. Montvale, NJ: Thompson PDR; 2003. Sulfasalazine in Pregnancy 1Stein Most side effects linked to sulfapyridine moiety1 No increase in fetal malformations Readily crosses placenta, but only minimal amounts in breast milk2 Interferes with folic acid metabolism – Folate important for neural tube development3 – Folic acid supplements (1 mg BID) advised prior to conception and throughout pregnancy RB, Hanauer SB. Gastroenterol Clin North Am. 1999;28:297-321. 2Miller JP. J R Soc Med. 1986;79:221-225. 3Czeizel AE, Dudas I. N Engl J Med. 1992;327:1832-1835. Aminosalicylates (B,C) Meta-analysis 7 studies: 642 5ASA, 1158 no med – – – – – Congenital anomalies: OR 1.16 (0.76, 1.77) Stillbirth OR 2.38 (0.65, 8.72) SAB OR 1.14 (0.65, 2.01) Preterm delivery 1.35 (0.85, 2.13) LBW OR 0.93 (0.46, 1.85) Sulfasalazine given w/ folic acid 1 mg BID • Folic acid: neural tube defects, CV, GU, cleft palate • Case reports of congenital malformation Placental and Breast Transfer Occurs • Potential allergic reaction newborn: watery diarrhea • SAS not associated with kernicterus or displacement of bilirubin from albumin Olsalazine: Pregnancy category C. All others, B Rahimi Reprod Toxicol 2008 Safety of Mesalamine in Pregnancy Study Marteau et al1 Diav-Citrin et al2 n 123* 165 Mean Mesalamine Dosage 2.1 ± 0.8 g/d 2.0 ± 1.6 g/d Incidence of Fetal Malformations (%) Patients 3.1 0.8 Controls 1.7-3.4† 3.8 *96 taking mesalamine during first trimester. †General population in France. 1Marteau P, et al. Aliment Pharmacol Ther. 1998;12:1101-1108. 2Diav-Citrin O, et al. Gastroenterology. 1998;114:23-28. Topical 5-ASA in Pregnancy Study of 19 pregnancies – Maintenance 5-ASA topical therapy at time of conception and throughout pregnancy – Successful full-term pregnancies for all patients, with no fetal abnormalities Minimal excretion of 5-ASA and metabolites in breast milk Many years of safe use Bell CM, Habal FM. Am J Gastroenterol. 1997;92:2201-2202. Antibiotics Metronidazole (B) /Ciprofloxacin (C) – Low risk of teratogenicity • Metronidazole: prospective controlled study, 2 metaanalysis – However, 2nd, 3rd T use, 1st T cleft lip, palate • Ciprofloxacin: prospective controlled study low risk of defects – Affinity for bones, arthropathy in children – Breast feeding not advised on MNZL, probably compatible with ciprofloxacin – Minimal benefit in CD and UC with longer use-avoid Rifaximin: Pregnancy C – teratogenicity in animal studies – Safety in humans in pregnancy/breastfeeding unknown Corticosteroids in Pregnancy Increased spontaneous abortions, cleft palate, stillbirths in mice; rare teratogenicity in humans (cleft palate) High doses associated with retardation of fetal growth No fetal adrenocortical insufficiency Safety uncertain with long-term use of high doses while breast-feeding Active-disease risks greater than drug risks to fetus, so use if needed Briggs GG, et al. Drugs in Pregnancy and Lactation. 5th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 1998. AZA/6-MP in Pregnancy Several studies in transplant recipients have reported safe use during pregnancy1 Study of IBD patients showed no in prematurity, spontaneous abortion, congenital abnormalities, or childhood neoplasia2 – Study population included fathers treated with AZA/6-MP In another study, AZA/6-MP did not reduce fertility in men3 Risk of birth defects similar to that in general population4 1Briggs GG, et al. Drugs in Pregnancy and Lactation. 5th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 1998. A, et al. Gastroenterology. 2003;124:9-17. 3Dejaco C, et al. Gastroenterology. 2001;121:1048-1053. 4Library: IBD & Your Family. Available at www.ccfa.org/medcentral/library/family/drugpreg.htm. Accessed March 6, 2003. 2Francella Azathioprine and Teratogenicity Largest Study to date 189 pregnant women on AZA who contacted one of seven teratogen information services were compared to a cohort of 230 pregnant women who took non-teratogenic treatments Rate of major malformations did not differ with six neonates each: – AZA (3.5%) vs control ( 3.0%) (p = .775; OR 1.17; CI: 0.37, 3.69). Mean birth weight and gestational age were lower in AZA group: – 2,995g vs. 3,252g [p = .001] – 37.8 weeks vs. 39.1 weeks [p = .001] The AZA group had more prematurity – 21.4% vs. 5.2% [p < .001] The AZA group had more low birth weight – 23% vs. 6.0% [p < .001] Goldstein Birth Defects Res A Clin Mol Teratol. 2007 Sep 10;79(10):696-701 Thiopurines and Nursing 2 infants breast fed with mothers on 6MP – 6MP levels by HPLC < 0.09% maternal dose1 4 mother-infant pairs 3 months post-partum were tested for 6MP metabolites – All infants were nursing – Maternal levels within therapeutic range – No metabolites found in offspring2 Moretti M. Ann Pharmacother 2006; Dec (40); Gardiner S. Br J Clin Pharmacol 2006; 62:453-56. Cyclosporine in Pregnancy Registry data on transplant recipients1 – No specific congenital abnormalities or birth defects – Prematurity: 56% – Low birth weight: 49.5% Study in 5 women with IBD2 – 4 live births, 1 missed abortion – No congenital abnormalities Should be given at experienced IBD centers3 1Armenti VT, et al. Transplantation. 1994;57;502-506. 2Marion JF, et al. Am J Gastroenterol. 1996;91:1975. 3Kornbluth A, Sachar DB. Am J Gastroenterol. 1997;92:204-211. Infliximab (B) Safety Database in Pregnancy: Outcomes of Women Exposed to Infliximab During Pregnancy Proportion of Patients (%) 80 70 67 67 66 67 60 Live births 50 Miscarriages 40 Therapeutic termination 30 20 17 16 20 19 17 15 13 All infliximab patients (N=96) Infliximab patients with CD (N=82) 11 10 0 General population Crohn’s disease Katz JA, et al. Am J Gastroenterol. 2004;99:2385-2392. Ventura et al. National Center for Health Statistics Vital Health Stat 2000;21:1-59 Hudson et al. Int J Gynaecol Obstet 1997;58:229-237. Medications: Biologics Biologics – Category B: Infliximab, adalimumab, certolizumab – Category C: Natalizumab Infliximab: 102 pregnancies, 54 outcomes1 – “Rescue” infliximab successful2 – Infliximab not detected in breast milk (n=5) – Demonstrated to cross the placenta and detectable in cord blood for up to 6 months from birth5 Adalimumab: 2 IBD pregnancies in published literature3,4 – 47 reported in OTIS registry Certolizumab: no published data in humans Natalizumab: IgG4, placental transfer in 1st trimester 1Katz J. Am J Gastroenterol 2004; 99(12):2385-92. 2Mahadevan U. APT 2005; 21(6):733-8. 3Vesga L. Gut 2005; 54(6):890.4Mishkin DS. IBD 2006; 12(8):827-8.5 Mahadevan Gastroenterology 2007;132:A-144 Methotrexate in Pregnancy Contraindicated during pregnancy – Chromosomal damage, teratogenic – Abortifacient Oligospermia noted during treatment of men – Returns to baseline posttreatment – Long-term effects unknown Briggs GG, et al. Drugs in Pregnancy and Lactation. 5th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 1998. Conclusions: IBD Drugs in Pregnancy 5-ASAs and corticosteroids low risk for use during pregnancy and breast-feeding Immunosuppressants – AZA/6-MP appear low risk during pregnancy – Methotrexate contraindicated Antibiotics – Ampicillin and cephalosporins are low risk – Ciprofloxacin and metronidazole should be avoided for longterm use Biologics: – Anti-TNF agents low risk. Infliximab and likely adalimumab cross placenta in third trimester Safety of IBD Medications in Breast-Feeding Low risk to Use When Warranted Oral mesalamine Topical mesalamine Sulfasalazine Limited Data Available Azathioprine 6-Mercaptopurine Infliximab Contraindicated Methotrexate Cyclosporine Metronidazole Corticosteroids Tacrolimus Ciprofloxacin Infliximab Natalizumab Adalimumab Certolizumab Physicians’ Desk Reference®. 57th ed. Montvale, NJ: Thompson PDR; 2003. Management of IBD in Pregnancy: Summary Pregnancy outcomes best if patient in remission at time of conception Many IBD-specific therapies appear to be low risk in pregnancy Monitoring of fetal growth particularly important May need additional nutritional therapy because of malabsorption Menopause in Women With IBD Menopause Natural menopause results from gradual decline in number of estradiol-producing ovarian follicles Surgical menopause may occur at any age as a result of oophorectomy Estradiol decreases; estrone becomes primary circulating hormone Testosterone declines at varying rate No data on effect of menopause on IBD Carr BR, Bradshaw KD. In: Braunwald E, et al, eds. Harrison’s Principles of Internal Medicine. 15th ed. New York, NY: McGraw-Hill; 2002. Menopausal Symptoms Bone loss—may be accelerated in CD and by corticosteroid use Vasomotor symptoms—“hot flashes” (50%–85%) Increases in total and LDL cholesterol Urogenital symptoms (45%) – Dyspareunia – Dysuria – Incontinence – Urinary tract infections U.S. Preventive Services Task Force. Guide to Clinical Preventive Services, 2nd ed. 1996. Available at: http/www.ahcpr.gov/clinic/cpsix.htm. Accessed January 28, 2003. Postmenopausal HRT Replaces estrogen in postmenopausal women Goal: manage symptoms caused by loss of estrogen Unopposed estrogen: only for women who have had hysterectomies Combined estrogen/progestin: recently found to increase risks for breast cancer, heart attacks, stroke HRT Protective Against Disease Activity After Menopause Cohort of post-menopausal women Disease activity pre and post menopause Those taking HRT less likely to have a disease flare in 2 years post menopause Dose response for length of use Form of menopause did not matter Kane SV Am J Gastro 2008; 103(5):1193-96. Potential Benefits vs Risks of HRT Potential Benefits Potential Risks Decrease in vasomotor symptoms Increase in invasive breast cancer Slower changes in body morphology Fewer osteoporotic fractures Side effects: bloating, irritability, weight gain, depression, vaginal bleeding Increased risk of thromboembolic events (blood clots, stroke) Increase in CVD Improvement in lipid balance Reduce IBD flare Clements D, et al. Gut. 1993;34:1543-1546. Stampfer MJ, et al. N Engl J Med. 1991;325:756-762. Women's Health Initiative. JAMA. 2002;288:321-333. HRT Guidelines for IBD Patients As with all therapeutic choices, therapy for menopausal symptoms should be individualized For women with severe osteopenia or osteoporosis, HRT benefits may outweigh risks if alternatives are not feasible For women at increased risk for breast cancer, HRT risks may outweigh benefits CVD risk vs benefit is controversial, but risk may outweigh benefit Osteoporosis in IBD General Risk Factors for Osteoporosis Advancing age Smoking Female gender Physical inactivity Family history Low calcium intake Alcohol use White/Asian race Small and thin body habitus Valentine JF, Sninsky CA. Am J Gastroenterol. 1999;94:878-883. Christchilles EA, et al. Arch Intern Med. 1991;151:2026-2032. Risk of Osteoporosis in IBD Low bone mass in 31% to 59% of IBD patients1-3 IBD-related risk factors4 – Onset of IBD before reaching age of peak bone mass – Inflammatory cytokines – Calcium malabsorption – Vitamin D deficiency (CD patients) – Drugs (corticosteroids, methotrexate, cyclosporine) 1Compston JE. Aliment Pharmacol Ther. 1995;9:237-250. 2Roux C, et al. Osteoporos Int. 1995;5:185-190. H, et al. Scand J Gastroenterol. 1997;32:1247-1255. 4Valentine JF, Sninsky CA. Am J Gastroenterol. 1999;94:878-883. 3Andreassen Prevention and Treatment of Osteoporosis in IBD Prevention – Baseline and follow-up measurements of bone density (DEXA) – Lifestyle and nutritional measures (eg, weight-bearing exercise, smoking cessation, calcium supplementation) – Possible HRT for high-risk postmenopausal women Treatment – Calcitonin – Bisphosphonates – PTH – IV therapies Valentine JF, Sninsky CA. Am J Gastroenterol. 1999;94:878-883. Corticosteroid-Induced Bone Loss Bone loss occurs early (weeks to months after initiation of therapy) Cumulative dose, dosage, and duration of corticosteroids may play a role Calcium and small doses of vitamin D may confer limited prophylactic benefit Valentine JF, Sninsky CA. Am J Gastroenterol. 1999;94:878-883. Van Staa TP, et al. J Bone Mineral Res. 2000;15:993-1000. Corticosteroid-Induced Loss of Bone Mass Enhanced bone resorption – Reduced intestinal calcium absorption and calcitonin synthesis – Increased renal calcium excretion, osteoclastic activity, and parathyroid hormone secretion – Enhanced binding of macrophages to bone Reduced bone formation – Reduced synthesis of osteoblasts and proliferation of osteoblasts – Impaired gonadal hormone production – Prednisone associated with increased rate of bone loss – Conflicting data regarding budesonide Reducing the Risk of Osteoporosis History and physical lab (25-hydroxy vitamin D, albumin, calcium, PTH) Bone density (DEXA) Minimize corticosteroids Normal T Score Monitor regularly Low BMD: T Score <–1 SD Osteoporosis: T Score <–2.5 SD Hormone (if appropriate) Hormone (if appropriate) Raloxifene (if appropriate) Raloxifene (if appropriate) Calcium Calcium Vitamin D Vitamin D General guidelines Bisphosphonates Repeat DEXA General guidelines Repeat DEXA Bisphosphonates in the Prevention and Treatment of Osteoporosis Lumbar Spine BMD 12 month diff. = 3.8% 12 month diff. = 2.7% % Change from Baseline 2 4 *† 1 † † †P<.05 0 control -1 0 3 * † *† Placebo * -3 vs 3 2 * -2 -4 *P<.05 vs baseline 6 * 9 12 Ris 5.0 mg * 1 0 0 6 Months Months Prevention Study Treatment Study Cohen S, Levy RM, Keller M, Boling E, et al. Risedronate therapy prevents corticosteroid-induced bone loss: a twelve-month, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum. 1999;42:2309-2318. Copyright© American College of Rheumatology. Reproduced with permission of John Wiley & Sons, Inc. 12 Reproduced from J Bone Miner Res. 2000:15;1006-1013 with permission of the American Society for Bone and Mineral Research. Infliximab in Patients With CD and Osteoporosis Prospective, 4-week trial with patients taking corticosteroids Significant decrease in CDAI with infliximab (P=.0001) Increase in surrogate markers for bone turnover Conclusion: increased bone synthesis with no increase in bone resorption CDAI = Crohn’s disease activity index. Abreu MT, et al. Am J Gastroenterol. 2002;97:S269. Abstract 819. Summary: Osteoporosis and IBD Bone density is unusually low in patients with active IBD who are taking steroids IBD causes other risk factors, eg, poor calcium absorption and disease-related inflammatory processes, that increase risk of bone loss Monitoring BMD is important Selection of treatment should be considered Clinical Management and Adherence Issues in IBD Illness-Related Factors Affecting Adherence in IBD Severity, extent, duration of disease Frequency, duration, intensity of flare-ups Type and severity of complications Patients with well-controlled disease and few flares are most likely to discontinue maintenance therapy Treatment-Related Factors Affecting Adherence in IBD Convenience – Dosage/dosing regimen – Formulation – Method of administration – Pill size Cost/reimbursement Choice of medication – Sulfasalazine, corticosteroids • Need to balance efficacy vs safety • Start with low doses, titrate slowly upward – Mesalamine • Dose-related efficacy but not toxicity • Initiate and maintain treatment with high doses • Induction dose = maintenance dose Patient-Related Factors Affecting Adherence 1Martin Inadequate education1; inadequate skills/knowledge to follow regimen2 Patients’ main concerns – Uncertain nature of IBD – Effects of medications3 Patients’ belief systems (treatment will not help, side effects outweigh benefits)2 Psychiatric disorders4 Male, unmarried, younger age5,6 Patterns of nonadherence7 A, et al. Ital J Gastroenterol. 1992;24:477-480. 2Levy RL, Field AD. Am J Gastroenterol. 1999;94:1733-1742. 3Drossman DA, et al. Psychosom Med. 1991;53:701-712. 4Nigro G, et al. J Clin Gastroenterol. 2001;32:66-68. 5Kane S. Am J Gastroenterol. 2001;96:2929-2932. 6Kane S. Am J Gastroenterol. 2001;96(suppl):S296. 7Kane S. In: Bayless TM, Hanauer SB, eds. Advanced Therapy of Inflammatory Bowel Disease. Hamilton, Ontario: BC Decker, 2001:9-11. Prevalence of Nonadherence to IBD Maintenance Therapy 1Blackwell Failure to take medication by patients with other illnesses: 25%–50%1 41% of patients on maintenance sulfasalazine do not take prescribed dosages2 Clinical research protocols overestimate drug adherence B. Clin Pharmacol Ther. 1972;13:841-848. 2van Hees PAM, van Tongeren JHM. J Clin Gastroenterol. 1982;4:333-336. Impact of Nonadherence on Outcomes in IBD % of Patients With Quiescent UC Remaining in Remission 100 90 Adherent to 5-ASA therapy (Asacol®) 80 70 60 Nonadherent to 5-ASA therapy* (Asacol®) 50 40 30 20 10 0 0 5 10 15 20 25 30 Time (months) *P=.001. Adapted with permission from Am J Med., Vol 114, Kane S, Huo D, Aikens J, Hanauer S. Medication nonadherence and the outcomes of patients with quiescent ulcerative colitis, pages 39-43, Copyright 2003 with permission from Excerpta Medica. Strategies for Optimizing Patient Adherence IBD is a chronic, lifelong illness Induce then maintain remission Reciprocal patient:clinician relationship Educate patient and family Individualize therapy/simplify regimen Promote emotional/psychological support Obtain patient’s commitment to therapeutic objectives Guided Self-Management in UC Intervention Group n=101 Personalized, guided self-management regimen Single 15-30-minute session – Relapse recognition – Treatment protocols Patients given written protocols Copy to primary MDs Robinson A, et al. Lancet. 2001;358:976-981. Control Group n=102 Routine treatment and follow-up Relapses Are Treated Earlier in Self-Managed Patients Proportion Untreated (%) 100 90 80 70 60 Control group 50 40 30 20 Intervention group 10 0 0 2 4 6 Time (days) Reprinted with permission from Elsevier (The Lancet. 2001;358:976-981). 8 10 12 Patient Self-Management Trends in self-management group (vs controls) – Fewer relapses (1.53 vs 1.93; P=NS) – Shorter duration of relapse if treated in first 24 h (17.7±17.1 d vs 25.5±37.4 d; P=.16) – 82% preferred self-management – 95% of controls said they were adopting self-management Robinson A, et al. Lancet. 2001;358:976-981. General Conclusions: Special Considerations for Women With IBD Women have more severe symptoms, more disease concerns than men Menstrual symptoms may be more severe OCs may be related to disease-activity flares IPAA improvement may be accompanied by feelings of decreased attractiveness Most women experience postoperative improvement in sexual activity General Conclusions: Special Considerations for Women With IBD (cont’d) Fertility – Normal or near normal in UC – May be affected in CD – IPAA reduces fertility – Voluntary childlessness makes data difficult to interpret Pregnancy – IBD has minimal effect on pregnancy outcomes – Conception during remission preferable – Some IBD drugs safe in pregnancy and breastfeeding – Disease activity is greater threat to pregnancy than treatment General Conclusions: Special Considerations for Women With IBD (cont’d) Menopause – Bone loss, especially in CD, is greatest risk, leads to osteoporosis – Cardiovascular risk increases, equal to risk in men by age 75 – Benefits of HRT are increasingly questioned as risks are observed Osteoporosis – Common in postmenopausal women, aggravated by CD and steroid therapy – Active plan to prevent bone loss and osteoporosis is vital – Nonsteroidal IBD drugs – Treatment options to preserve bone mass General Conclusions: Special Considerations for Women With IBD (cont’d) Adherence improves outcomes; nonadherence leads to relapse Patient must understand nature of disease, goals of treatment Treatment plan tailored to patient’s life and needs Adherence improved by good physician-patient communication