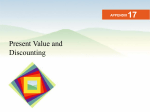
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Nausea and Vomiting of Pregnancy: Cases for Pharmacological Consideration Educational Support & CME • Educational Support – An educational grant to support this program has been provided by Duchesnay USA. • Continuing Medical Education (CME) Credit – An accredited, multimedia presentation is available online at NVPCases.com – Physicians and Nurses can earn 1.0 hours CME credit. Clinical Trial Experiences With NVP Gary D.V. Hankins, MD Garland D. Anderson, MD Distinguished University Chair in Maternal Fetal Medicine Professor and Chairman, Department of Obstetrics & Gynecology University of Texas Medical Branch Galveston, Texas Commercial Interest(s) Duchesnary USA Advisory Board Member Nausea and Vomiting of Pregnancy • Nausea and vomiting of pregnancy (NVP) is a spectrum disorder with varying degrees of symptoms1 • NVP, commonly known as morning sickness, occurs in approximately 75%-80% of pregnant women2 • Symptoms range from mild to severe – Severe NVP (hyperemesis gravidarum [HG]) is seen in approximately 1-3% of pregnancies3 • Self-limiting condition with no impact on long-term health1 1Badell ML, Ramin SM, Smith JA. Pharmacotherapy.2006;26:1273-87. R, Barnie-Adshead AM, Jagger C. Br J Gen Pract. 1993;43:245-8. 3Tsang IS, Katz VL, Wells SD. Int J Gynaecol Obstet. 1996;55:231-5. 2Gadsby Prevalence of NVP Percentage of Women Experiencing Symptoms Nausea 50%-90% Vomiting 0 25%-50% NVP 70%-85% Recurrent NVP in subsequent pregnancy 80%-85% 10 20 30 40 50 60 70 80 90 100 Einarson TR, Navioz Y, Maltepe C et al. J Obstet Gynaecol. 2007;27(4):360-2. Erick M. OBG Management. 2000;25-35. Gadsby R, Barnie-Adshead AM, Jagger C. Br J Gen Pract. 1993;43:245-8. Koren G, Maltepe C. J Obstet Gynaecol. 2004;24(5):530-3. O’Brien B, Zhou Q. Birth. 1995;22:93-100. 40% of Pregnancies Result in Clinically Significant NVP 40% Gadsby R, Barnie-Adshead AM, Jagger C. Br J Gen Pract. 1993;43:245-8. O’Brien B, Zhou Q. Birth. 1995;22:93-100. Vellacott ID, Cooke EJA, James CE. Int J Gynecol Obstet. 1988;27:57-62. Medical, Economic, & Social Impacts • Quality of life (QOL) and work efficiency are adversely affected by NVP.1 • When QOL measures are used in research studies, the scores for women with NVP are worse than the scores of women who report chronic depression.2 • A 2002 study estimated reduced productivity, visits to health care professionals, and the cost of medications and other remedies at $2947 per woman with moderate to severe NVP. 2 • Severe NVP is estimated at approximately $130 million/year from hospital visits alone.3 1O'Brien 2Attard CL, B, Naber S. Birth. 1992;19:138–43. Kohli MA, Coleman S et al. Am J Obstet Gynecol. 2002;186(5 suppl):S220–7. 3Miller F. Am J Obstet Gynecol. 2002;186(5 suppl):S182-3. Impact of NVP Work Affected Required Time Off Work Relationships Affected 1O'Brien 2Miller Caused Depression B, Naber S. Birth. 1992;19:138–43. F. Am J Obstet Gynecol. 2002;186(5 suppl):S182–3. Effectiveness of Delayed-Release Doxylamine + Pyridoxine for NVP: A Randomized Placebo Controlled Trial • Objective – Evaluate the effectiveness of doxylamine succinate 10 mg-pyridoxine hydrochloride 10 mg (delayed-release preparation; Diclectin®), as compared with placebo for nausea and vomiting of pregnancy. • Study design – A randomized, double-blind, multicenter placebo controlled trial studying pregnant women suffering from NVP, analyzed by intention to treat. – Women received active drug (N = 131) or placebo (N = 125) for 14 days – NVP symptoms were evaluated daily using the Pregnancy Unique Quantification of Emesis (PUQE) scale. Koren G, Clark S, Hankins GDV et al. Am J Obstet Gynecol. 2010;203:571.e1-7. Pregnancy Unique-Quantification of Emesis and Global Assessment of Well-being Koren G, Clark S, Hankins GDV et al. Am J Obstet Gynecol. 2010;203:571.e1-7. Subject Enrollment & Final Study Disposition Koren G, Clark S, Hankins GDV et al. Am J Obstet Gynecol. 2010;203:571.e1-7. Score Doxylamine succinate/pyridoxine hydrocholoride (Diclectin®): Phase 3 Efficacy Pregnancy-Unique Quantification of Emesis/Nausea (PUQE) index: Total score is sum of replies to each of the 3 questions. Nausea Score: Mild NVP = ≤6; Moderate NVP = 7 to 12; Severe NVP = ≥ 13. http://clinicaltrials.gov/ct2/show/results/NCT00614445?term=diclectin&rank=1§=X436015#othr. Koren G, Clark S, Hankins GDV et al. Am J Obstet Gynecol. 2010;203:571.e1-7. Primary Endpoint Variable Doxylamine/Pyridoxine (N = 131) Placebo (N = 125) Mean difference in PUQE score baseline to day 15 Mean ± SD Median Mean area under the curve difference in PUQE score baseline (day-by-day) P value 0.006 -4.8 ± 2.7 -3.9 ± 2.6 -5.0 -4.0 61.5 ± 36.9 53.5 ± 37.5 < 0.0001 Koren G, Clark S, Hankins GDV et al. Am J Obstet Gynecol. 2010;203:571.e1-7. Secondary Endpoints Doxylamine/ Pyridoxine (N = 131) Variable Placebo (N = 125) P value Difference in global assessment of well-being from baseline to day 15 Mean ± SD Median Time loss from employment, D Subjects asking compassionate use of drug after day 14, N (%) 2.8 ± 2.8 2.5 0.92 ± 3.86 1.8 ± 2.2 2.0 2.37 ± 10.23 0.005 64 (48.9) 41 (32.8) 0.009 0.06 Women receiving placebo were 50% more likely to report use of alternate therapies and dietary modification. Koren G, Clark S, Hankins GDV et al. Am J Obstet Gynecol. 2010;203:571.e1-7. Adverse Events Profile Diclectin® (N = 133) Placebo (N = 128) 3.01% 3.91% 0 0.78% Intrauterine Death 0.75% 0 Spontaneous Abortion 1.5% 0.78% Abdominal Pain 3.8% 6.3% Fatigue 6.8% 6.3% Somnolence 14.3% 11.7% Dry Mouth 3.0% 0.8% Dizziness 12.8% 15.6% Headache 12.8% 15.6% Variable Total Serious AEs Bile Duct Stone http://clinicaltrials.gov/ct2/show/results/NCT00614445?term=diclectin&rank=1§=X436015#othr. Koren G, Clark S, Hankins GDV et al. Am J Obstet Gynecol. 2010;203:571.e1-7. Adverse Events Profile Variable Diclectin® (N = 131) Placebo (N = 125) P value Somnolence 19 (14.5) 15 (12) 0.54 Dry mouth 4 (3.0) 1 (0.8) 0.37 Hypersensitivity 1 (0.8) 0 (0) > 0.99 Dizziness 8 (6.0) 8 (6.4) 0.94 Headache 17 (13) 20 (16) 0.51 0 (0) 1 (0.8) 0.49 Loss of consciousness Koren G, Clark S, Hankins GDV et al. Am J Obstet Gynecol. 2010;203:571.e1-7. Effectiveness of Delayed-Release Doxylamine + Pyridoxine for NVP: A Randomized Placebo Controlled Trial • Significant improvement over placebo – Change in PUQE baseline to day 15 – Global assessment of well-being baseline to day 15 – Day-to-day changes in PUQE & global assessment of well-being • Significantly superior to placebo – Continue treatment on a compassionate basis • Women receiving placebo • – Reported 50% > use of alternate therapies and dietary modification No increase in adverse effects compared with placebo (somnolence, back pain) Koren G, Clark S, Hankins GDV et al. Am J Obstet Gynecol. 2010;203:571.e1-7. Drugs in Pregnancy Gideon Koren MD, FRCPC, FACMT Director, The Motherisk Program The Hospital for Sick Children, Professor of Pediatrics, Pharmacology, Pharmacy and Medical Genetics; Professor of Medicine, Pediatrics and Physiology/Pharmacology; Ivey Chair in Molecular Toxicology The University of Toronto Toronto, Ontario, Canada Commercial Interest(s) Duchesnay Honorarium (Consultant) Research Grants Drugs in Pregnancy: The Issues • Only half of all pregnancies are planned. • Many women need medications for pregnancy induced conditions (e.g. morning sickness), chronic conditions (e.g. epilepsy), and intercurrent conditions (e.g. allergies). • Women work with chemicals, are exposed to radiation, and use illicit drugs. • During embryogenesis, drugs and chemicals may adversely affect development. Situational Analysis • Anxiety of birth defects – Leads women not to take medications during pregnancy and lactation. – Leads pharmaceutical companies not to develop drugs for pregnant and lactating women. • Women are not treated appropriately even after the first trimester, or for life threatening conditions. Perception of Teratogenic Risk • Even when exposed to non teratogenic drugs, women assign a 25% teratogenic risk.1 • Evidence-based counseling can prevent unnecessary pregnancy terminations.2 1Koren G, Bologa M, Long D et al. Am J Obstet Gynecol. 1989;160(5 Pt 1):1190-4. 2Koren G, Pastuszak A. Teratology. 1990;41(6):657-61. Nausea and Vomiting of Pregnancy • NVP affects 80% of pregnant women. • Doxylamine-pyridoxine (Bendectin®) was used by 40% of pregnant American women in 1978. • Due to litigations, drug removed in 1983 despite scientific and FDA support. • Meta-analysis: OR 1.01 (0.66-1.55) • In Canada: Delayed-release doxylamine/pyridoxine (Diclectin®) use is increasing with a temporal decrease in hospitalizations. Einarson TR, Leeder JS, Koren G. Drug Intell Clin Pharm. 1988;22(10):813-24. U.S. Temporal Trends for Limb Reduction Deformities, Bendectin® Sales, and Hospitalizations for NVP 3.5 Hospitalization 3.0 Trend 2.5 2.0 1.5 Limb Reduction Deformities 1.0 0.5 Bendectin® Sales 0.0 74 76 78 80 82 84 86 88 Year Neutel CI, Johansen HL. Can J Public Health. 1995;86(1):66-70. Rate of Hospitalization in Canada 150 Bendectin® Hospitalizations for EVP 18 16 100 14 12 50 10 Diclectin® 8 80 82 84 86 88 90 92 94 96 Prescriptions in 1000s Hospitalizations/1000 Births 20 0 Year EVP = Excessive Vomiting in Pregnancy Neutel CI, Johansen HL. Can J Public Health. 1995;86(1):66-70. Motherisk-NVP Line • The only counseling health line worldwide for women suffering from NVP. • 1-800-436-8477 (Canada & USA) • Evidence-based counseling on drug safety, effectiveness for symptom management • Large prospective database for research Which Drugs Are Safe for NVP? • Diclectin®/Bendectin® based on over 250,000 women f/u • Safe even at doses up to 8 tab/d1 • Other antihistamines2 – Odds ratio: 0.76 (0.6-0.94) • Ondansetron -- possibly safe, based on GlaxoSmithKline • postmarketing, Motherisk controlled study (N = 169) and Danish study (N = 4000) Metoclopramide -- safe based on large numbers3 1Atanackovic G, Navioz Y, Moretti ME, Koren G. J Clin Pharmacol. 2001;41:842-5. 2Seto A, Einarson T, Koren G. Am J Perinatol. 1997;14:119-24. 3Matok I, Gorodischer R, Koren G et al. N Engl J Med. 2009;360:2528-35. Which Drugs Are Safe for NVP? • Phenothiazines -- probably safe based on several series1 • Ginger -- safe2 • Pyridoxine -- safe even at large doses (50-500)3 1Magee LA, Mazzotta P, Koren G. Am J Obst Gynecol. 2002;186:S256-61. G, Chng LA, Karimi-Tabesh L et al. Am J Obst Gynecol. 2003;189:1374-7. 3Shrim A, Boskovic R, Maltepe C et al. J Obstet Gynaecol. 2006;26:749-51. 2Portnoi Psychosocial Morbidity in NVP • More severe NVP – More measured depression – Considering termination of pregnancy – Adverse relationships – Adverse effects on partners – Perception of NVP harming the baby – N = 3201 Mazzotta P, Stewart D, Atanackovic G et al. J Psychosom Obstet Gynaecol. 2000;21:129-36. Factors Associated With Pregnancy Termination in NVP • • • • N = 3201 N = 413 considered termination N = 108 terminated “due to NVP” Independent factors with women considering termination – Unplanned pregnancy – More severe vomiting – Feeling of depression – Partner’s daily life – Relationship with partner Mazzotta P, Stewart D, Atanackovic G et al. J Psychosom Obstet Gynaecol. 2000;21:129-36. Pregnancy Termination • Factors independently associated with termination – Unplanned pregnancy – Multiparity – Depression • These factors should be considered when managing these women Mazzotta P, Stewart D, Atanackovic G et al. J Psychosom Obstet Gynaecol. 2000;21:129-36. Preemptive Therapy for NVP • After doxylamine/pyridoxine (Bendectin®) d/c – Three-fold more cases of hospitalization for severe NVP • Suggests that symptom treatment prevents deterioration of cases. • Preemptive study (N = 25) • Women reporting severe NVP in a previous pregnancy are “afraid to conceive again.” • Commenced using antiemetics upon becoming aware of pregnancy. Koren G, Maltepe C. J Obst Gyn. 2004;24:530-3. Preemptive Study • Matched to 35 women counseled regularly when symptoms started • Severe NVP decreased from 18 to 8 cases (P = 0.01) – No such change in the comparison group • In the control group-unchanged severe NVP (80%) when compared to previous pregnancy • Presently, a randomized controlled clinical trial with delayed-release doxylamine/pyridoxine (Diclectin®) is in progress. Koren G, Maltepe C. J Obst Gyn. 2004;24:530-3. Doxylamine/Pyridoxine (Diclectin®) Preemptive Prospective Trial • Women with severe NVP in previous pregnancy • Randomized to receive (Diclectin®) either before NVP started, or at the outset of symptoms • Preemptive group had less severe symptoms in first weeks. • Overall more cases that NVP stopped before labor Maltepe C, Koren G. Obstet Gynecol Int. 2013;2013:809787. Preemptive Prospective • Significant reduction in episodes of severe NVP • Both groups received similar personalized approach of counseling: – Nutritional changes – Acid reflux treatment • All physicians had to be part of the circle of care. Maltepe C, Koren G. Obstet Gynecol Int. 2013;2013:809787. Acid Reflux in NVP • Women with acid reflux during NVP – Significantly more severe symptoms of nausea, vomiting, and retching • Increased in acid reflux in pregnancy – Intra-abdominal pressure, progesterone • Treatment with histamine-2 blockers or proton pump inhibitors significantly reduced symptoms Gill SK, Maltepe C, Mastali K, Koren G. Obstet Gynecol Int. 2009;2009:585269. Conclusions • The return of doxylamine/pyridoxine (Diclegis®), a known and safe drug for NVP, will be welcomed by the obstetric community and pregnant women. • Trivialization of NVP must be replaced by individualized management which includes pharmacotherapy and non-pharmacological means. Patient Case Studies Jennifer R. Niebyl, MD Professor and Vice Chair for Obstetrics Department of Obstetrics and Gynecology The University of Iowa Carver College of Medicine Iowa City, Iowa Commercial Interest(s) Duchesnay USA Honorarium (Consultant) Chateauguay Medical Inc. Honorarium (Consultant) Case #1 • • • • • 32-year old female in 1st trimester of pregnancy Frequency of nausea is generally throughout the day Frequency of vomiting is 1-2 times daily in the morning Doesn’t feel good enough to go to work Steady weight loss over the last couple of weeks Case #1 • Phones physician’s office because of NV • Patient wants to know what she can do to get rid of her NV • Patient does not want to come into the office • Can she be managed clinically over the phone? • What additional information do we need from the patient? Any headache, abdominal pain, fever? • What are the first steps in treating her? Clinical Management of NVP • Avoid odors, triggers • Avoid fatty, spicy foods • Omit iron tablets • Frequent small feedings, fluids between meals • Bland and dry, high-protein foods • Crackers at bedside in AM • Avoid empty stomach Clinical Management of NVP • Large ketones – Intermittent IV hydration (with multivitamins) – LFTs, amylase, urinalysis, electrolytes • Follow urinary ketones, weight, electrolytes • Ultrasound – Multiple gestation – Hydatidiform mole • Antiemetics • Prevent parenteral nutrition Case #1 • Follow-up with patient reveals NV not subsided • Patient declines medication • Alternative therapies are offered – Pyridoxine (vitamin B6), PrimaBella®, ginger Treatment of NVP: Pyridoxine (Vitamin B6) • Sahakian et al. – 25 mg (1/2 tab) PO Q8hrs or placebo (N = 59) – ~ 50% of patients stopped vomiting – Severe nausea decreased to mild or moderate – No effect on mild nausea • Vutyavanich et al. – 30 mg/d PO versus placebo x 5 d (N = 342) – Significant decrease in nausea (P < 0.008) – No. of vomiting episodes reduced (P = 0.0552) Sahakian V, Rouse D, Sipes S et al. Obstet Gynecol. 1991;78:33-6. Vutyavanich T, Wongtra-ngan S, Ruangsri R. Am J Obstet Gynecol. 1995;173:881-4. Treatment of NVP • Pyridoxine + doxylamine (not delayed release like Bendectin®, Diclectin®, Diclegis®) • Pyridoxine (vitamin B6) 50-mg tablets – 1/2 tablet TID • Doxylamine (Unisom SleepTabs®) 25 mg – 1 tablet QHS; 1/2 tablet in AM and PM PRN • Lack of teratogenicity McMahon MJ in Yankowitz J & Niebyl JR: Drug Therapy in Pregnancy. Lippincott, Williams & Wilkins, Philadelphia, 2001:p. 81. Delayed-Release Pyridoxine/Doxylamine • FDA approved Diclegis® on April 8, 2013 • Delayed-release pyridoxine 10 mg + doxylamine 10 mg • FDA category A for pregnancy – 2 tablets QHS, 1 tablet QAM PRN – +1 tablet QPM PRN • Only FDA-approved treatment for NVP Acupuncture in NVP • Two randomized trials – N = 33, Sweden, versus placebo acupuncture1 • Different site and superficial • Helped hyperemesis gravidarum (HG) – N = 55, England, traditional acupuncture versus sham2 • Blunt cocktail stick over different area and dressing • Nausea vomiting, outpatients, no difference 1Knight 2Carlsson B, Mudge C, Openshaw S et al. Obstet Gynecol. 2001;97:184-8. CP, Axemo P, Bodin A et al. J Pain Symptom Man. 2000;20:273-9. Alternative Therapies: Acupressure Neiguan point or pericardium 6 (PC6) Acupressure in NVP • Sea-Band®, Bioband® • 7 randomized controlled trials of PC6 stimulation – Conflicting results – Absence of blinded testing – Both groups improved with time – Largest study -- no effect O'Brien B, Relyea MJ, Taerum T. Am J Obstet Gynecol. 1996;174:708-15. Dundee JW, Sourial FB, Ghaly RG, Bell PF. J R Soc Med. 1988;81:456-7. Features and Components ELASTIC WRISTBAND LOW BATTERY INDICATOR II POWER LEVELS (I - V) POWER BUTTON III I IV V Press to turn ON Press again to increase to the next level Press and hold for 3 to 5 seconds to turn OFF ELASTIC KEEPER (BELT LOOP) Figure 4 Nerve Stimulation of PC6 • Reliefband® (now PrimaBella®) – Electrical current emitted – Rotate dial to 5 settings – Patients randomized to active or sham device – Researchers assessing outcomes not blinded – 3 week trial, 95 active device, 92 controls – Nausea and vomiting less in study group (P = 0.01) – Weight gain 5.5 lbs versus 2.9 lbs controls (P = 0.003) – Weight gain 77% versus 54% controls (P = 0.001) – Medication use 25% both groups Rosen T, de Veciana M, Miller HS et al. Obstet Gynecol. 2003;102:129-35. Alternative Therapies: Ginger • Randomized double-blind trials – 70 outpatients with NVP1 • 250 mg ginger capsules versus placebo QID x 4 d – 27 women with HG2 • 250 mg ginger capsules versus placebo QID × 4 d • Reduced nausea and episodes of vomiting in ginger groups 1Vutyavanich T, Kraisarin T, Ruangsri R et al. Obstet Gynecol. 2001;97:577-82. 2Fischer-Rasmussen W, Kjaer SK, Dahl C, Asping U. Eur J Obstet Gynecol Reprod Biol. 1991;38:19-24. Pyridoxine vs. Ginger • Randomized trial, identical appearing capsules – Pyridoxine 25 mg TID (N = 145) – Ginger 350 mg TID (N = 146) • No differences between 2 groups at 1 week, 2 weeks, 3 weeks in nausea and vomiting • Ginger -- More belching, heartburn • No differences in fetal outcome, birth weight, or congenital anomalies Smith C, Crowther C, Willson K et al. Obstet Gynecol. 2004;103:639-45. Ginger for NVP • 6 double-blind, randomized controlled trials for efficacy, N = 675 – 4 showed superiority over placebo – 2 showed equivalence to pyridoxine • 1 observational cohort study, N = 187 – No significant side effects – No adverse effects on pregnancy outcome Borrelli F, Capasso R, Aviello G et al. Obstet Gynecol. 2005;105:849-56. Case #2 • 28-year old female presents to the ED with severe NV • Patient about 10 weeks along (best guess based on last known menstruation) • Patient placed in L & D for evaluation • Patient complains of vomiting 4 times in the last 5 days • Nausea and excessive salivation precede vomiting Antiemetic Drugs • • • • • Antihistamines Phenothiazines Prokinetic agents Serotonin (5-HT3) antagonists Corticosteroids • None are FDA-approved for use in pregnancy except Diclegis® Koren G and Levichek Z. Am J Obstet Gynecol. 2002;186:5248-52. Phenothiazines Used for NVP FDA Category • Promethazine (Phenergan®) C • Prochlorperazine (Compazine®) C • Chlorpromazine (Thorazine®) C • Adverse effects of phenothiazines -- sedation, hypotension, dry mouth, extrapyramidal symptoms NVP: Metoclopramide (Reglan®) • Prokinetic agent -- increases upper GI motility, lower esophageal sphincter tone • Dopamine antagonist • No increased risk of birth defects in 303 newborns in Michigan (Medicaid data) • Category BM Safety of Metoclopramide (Reglan®) in Pregnancy • 3,458 women (4.2% of pregnancies) exposed in the first trimester in Israel • Most exposed for 1-2 weeks • No increased risk of congenital malformations, low birth weight, preterm delivery, or perinatal death • Safe for use for nausea and vomiting in pregnancy except if patient on an SSRI Matok I, Gorodischer R, Koren G et al. N Engl J Med. 2009;360:2528-35. Promethazine vs. Metoclopramide for NVP • Promethazine 25 mg IV (N = 76) or metoclopramide 10 mg IV (N = 73) both every 8 hours • Similar vomiting frequency and well-being scores • Metoclopramide less drowsiness, dizziness, dystonia • 3 refusals due to pain at injection site (tissue damage) – FDA black box warning promethazine (Phenergan®) 2009 – Give deep IM, not SC or IV • Metoclopramide preferred over promethazine except in patients on SSRI’s Tan PC, Khine PP, Vallikkannu N, Omar SZ. Obstet Gynecol . 2010;115:975-81. 5-HT3 Receptor Antagonists Used for NVP FDA Category • Ondansetron (Zofran®) BM • Dolasetron (Anzemet®) BM • Granisetron (Kytril®) BM • Limited information in human pregnancy (except Zofran®) • Ondansetron efficacy similar to promethazine, yet less sedating Einarson AK, Chandra K, Maltepe C et al. Teratology. 2002;65:308 (abs). Sullivan CA, Johnson CA, Roach H et al. Am J Obstet Gynecol. 1996;174:1565-8. Ondansetron (Zofran®) & Pregnancy Outcomes • 1233 first trimester exposures • 1784 total pregnancy exposures • No differences in: – Spontaneous abortions, stillbirth, any major birth defect, preterm delivery, low birth weight, small for gestational age Pasternak B, Svanström H, Hviid A. N Engl J Med. 2013;368:814-23. Methylprednisolone (Medrol®) • 16 mg PO TID x 3 days, then taper by 4 mg/day x 2 weeks • Initial study suggested benefit (N = 40) versus promethazine • Larger study no difference in rate of rehospitalization compared to placebo (N = 110) – All patients received promethazine – Promethazine 25 mg + metoclopramide – Metoclopramide 10 mg IV + PO PRN • Increased risk of CL CP before 10 weeks gestation Safari HR, Fassett MJ, Souter IC et al. Am J Obstet Gynecol. 1998;179:921-4. Yost NP, McIntire DD, Wians FH et al. Obstet Gynecol. 2003;102:1250-4. Park-Wyllie L, Mazzotta P, Pastuszak A et al. Teratology. 2000;62:385-92. Treatment Algorithm for NVP Monotherapy Pyridoxine Add Doxylamine (Unisom SleepTabs®) Adjust according to severity of symptoms Add Dimenhydrinate (Dramamine®) PO/PR (not to exceed 400 mg/day; not to exceed 200 mg/day if patient is also taking doxylamine) or Promethazine (Phenergan®) PO/PR (Add alternative therapies at any time) Koren G and Levichek Z. Am J Obstet Gynecol. 2002;186:S248-52. Treatment Algorithm for NVP No Dehydration Add any of the following: Add: Metoclopramide (Reglan®) IM/PO or Ondansetron (Zofran®) IM/PO or Prochlorperazine (Compazine®) IM/PO/PR or Promethazine (Phenergan®) IM/PO/PR Koren G and Levichek Z. Am J Obstet Gynecol. 2002;186:S248-52. Treatment Algorithm for NVP Dehydration IV fluid replacement IV multivitamin supplementation (thiamine) Dimenhydrinate (Dramamine®) IV Add: Metoclopramide (Reglan®) IV or Prochlorperazine (Compazine®) IV or Promethazine (Phenergan®) IM, PO, PR not IV Add: Methylprednisolone (Solu-Medrol®) IV/PO, taper to lowest effective dose, < 6 weeks’ duration or Ondansetron (Zofran®) IV Koren G and Levichek Z. Am J Obstet Gynecol. 2002;186:S248-52. Case #2: Summary • Etiology still not clear, thus many therapies • Rule out other pathology • Dietary alterations • Diclegis® • Other antiemetic drugs • Alternative remedies Conclusions Ralph W. Hale, MD Past Executive Vice President, The American College of Obstetrics and Gynecologists Oak Hill, Virginia Commercial Interest(s) Duchesnay USA Honorarium Conclusions • NVP is a prevalent condition with clinical impact for many pregnant women. • Many pregnant women, as well as their physicians, do not treat NVP with pharmacological therapy. • Pharmacological as well as non-pharmacological treatment options are currently available to women with NVP to improve their quality of life and overall pregnancy. Question • How many antiemetic medications are FDA Category A for use in the first trimester of pregnancy? Answer: One Antihistamines Used for NVP FDA Category • Diclegis® A • Dimenhydrinate (Dramamine®) BM • Diphenhydramine (Benadryl®) BM • Meclizine (Antivert®) BM • Hydroxyzine (Vistaril®, Atarax®) C • Cetirizine (Zyrtec®) BM Thank you!