Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
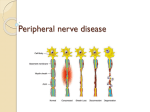
DISORDERS OF THE PERIPHERAL NERVOUS SYSTEM Prepared by: Dr. Sarwer Jamal Al-Bajalan M.B.Ch.B, F.I.B.M.S(Neurology) 2014 Disorders Of The Peripheral Nervous System ○ Introduction and clinical approach ○ Acquired polyneuropathies(PNP) ○ Hereditary neuropathies ○ Mononeuritis Multiplex ○ Mononeuropathies Peripheral neuropathy: Introductionand clinical approach General considerations Peripheral neuropathy or polyneuropathy: diffuse peripheral nerve lesion, often symmetrical Mononeuropathy—lesion of a single nerve (i.e., median, femoral, or abducens). Often entrapment or trauma Mononeuritis multiplex—focal involvement of two or more individual nerves, often asymmetric Types and causes of peripheral neuropathy Polyneuropathy: clinical manifestations Age of onset varies, for example ○ Childhood—CMT ○ Adulthood—Diabetes ○ Older adult—Paraproteinemia Acuity of onset ○ Acute—AIDP, porphyria, toxic, tick paralysis, diphtheria, vasculitis ○ Chronic—B12 deficiency, paraproteinemia, diabetes, most other causes Symptoms ○ Motor symptoms—distal weakness predominates in most neuropathies. Diffi culty opening jars, tripping over feet ○ Sensory symptoms—may be • positive (tingling, burning) or • negative (numbness). ○ Autonomic symptoms—orthostatic lightheadedness, gastroparesis, sweating abnorma ities, erectile dysfunction, tachycardia Positive Sensory symptoms ○ Paresthesia — spontaneous abnormal sensations, which are not unduly painful ○ Dysesthesia — painful paresthesia ○ Allodynia — painful sensation resulting from a nonpainful stimulus, such as stroking, high sounds ○ Hyperesthesia — increased sensitivity to a stimulus ○ Hyperalgesia stimulus — increased sensitivity to a painful Signs of PNP Large-fiber neuropathy • Loss of vibration and position sense • Diminished or absent reflexes • Positive Romberg sign • Pseudoathetosis Small-fiber neuropathy • Loss of pain and temperature sensation • Reflexes may be normal. Autonomic dysfunction • Miosis • Orthostatic hypotension (BP supine and erect after 3 minutes) Cutaneous sensory loss in a stocking-glove distribution Foot deformities such as pes cavus, pes planus, or hammertoes may indicate a hereditary neuropathy. Nerve thickening may be seen in CMT, leprosy, Refsum disease, amyloidosis, or HNPP. Investigations in PNP EMG and ENG o Can distinguish polyneuropathy from polyradiculopathy or plexopathy o Can identify mononeuropathy and mononeuritis multiplex o Can distinguish axonal and demyelinating neuropathies o Can identify subclinical sensory or motor involvement Blood tests ○ I) 75 gram 2 hour oral GTT, B12, TSH, SPEP, immunofixation, ESR, renal and liver function tests ○ II) ANA, dsDNA, anti-Ro, anti-La, HIV, Lyme ○ III) Others… CSF examination; (AIDP/CIDP) Nerve biopsy: sural, radial, superficial peroneal(vasculitis) Investigation of peripheral neuropathy Acquired polyneuropathies Diabetic neuropathies Guillain–Barre syndrome (GBS) Chronic demyelinating polyneuropathy Chronic axonal polyneuropathy Brachial plexopathy Lumbosacral plexopathy Spinal Root Lesions Diabetic neuropathies Commonest cause of neuropathy worldwide. o 8% have neuropathy at diagnosis; o 50% after 25 years. Diagnosis o Diabetes = fasting glucose >126, 2 hr postprandial glucose of 200 mg/dL o Impaired fasting glucose = fasting glucose 100–125 mg/dL o Impaired glucose tolerance = 2 hr postprandial glucose 140–199 mg/dL Classification of diabetic neuropathies: o o o o o Diabetic polyneuropathy Diabetic neuropathic cachexia Diabetic amyotrophy Diabetic cranial neuropathies Diabetic mononeuropathies Diabetic polyneuropathy Length dependent, painful sensory > motor neuropathy Autonomic dysfunction is common. NCS: Show length-dependent axonal polyneuropathy. May be normal if only small fibers involved. Rx : Foot care, Control of hyperglycemia, and Medications for neuropathic pain (i.e., gabapentin, nortriptyline, duloxetine, pregabain). Diabetic amyotrophy Clinical manifestations Abrupt onset of severe pain in backs, hips, and thighs followed by weakness and wasting of proximal muscles > distal muscles Usually unilateral, but may progress to be bilateral Associated with weight loss D Dx : Vasculitis, malignant infiltration Investigations NCS(ENG) usually show distal sensorimotor polyneuropathy Needle EMG shows denervation in proximal lower extremity muscles including paraspinals Consider MRI to rule out structural or infi trative process causing radiculopathy or plexopathy Management Spontaneous recovery over 1–3 years Methylprednisolone (1g iv tiw x 1, then qweek x 3, then q2 weeks x 4) may speed recovery IVIG reported to be beneficial as well Diabetic amyotrophy Diabetic cranial neuropathies ○ Oculomotor (III) palsy — pupil sparing ○ Abducens (VI) palsy Diabetic mononeuropathies DM patients are prone to entrapment syndromes. Surgery should be considered if motor involvement, but results may not be as good as in nondiabetics. ○ Median at the wris(CTS) ○ Ulnar at the elbow ○ Common peroneal at the fibular neck Guillain–Barre syndrome (GBS) 1. Acute inflammatory demyelinating polyradiculoneuropathy (AIDP) Epidemiology: The most common cause of acute neuromuscular weakness. Annual incidence 1–2 /100,000 Two-thirds are preceded by a GI or upper respiratory tract infection (Campylobacter jejuni, CMV, EBV, haemophilus influenzae, mycoplasma). Pathogenesis There is a predominantly cell-mediated inflammatory response directed at the myelin protein of spinal roots, peripheral and extra-axial cranial nerves, possibly triggered by molecular mimicry between epitopes found in the cell walls of some microorganisms and gangliosides in the Schwann cell and axonal membranes. The resulting release of inflammatory cytokines blocks nerve conduction and is followed by a complement-mediated destruction of the myelin sheath and the associated axon Clinical features Neurologic symptoms begin 5 days to 3 weeks after antecedent event. Ascending weakness. Proximal weakness may occur as well because of root demyelination Early loss of reflexes Paresthesias common. Actual sensory loss is variable. Progressive over days to weeks, nadir by 4 weeks Often associated with back pain Involvement of cranial nerves can cause facial and bulbar weakness. Up to 25% have respiratory involvement requiring mechanical ventilation. Autonomic dysfunction (hypotension, hypertension, cardiac arrhythmia) Diagnostic studies NCS: May be normal early in the course of the disease Prolongation of F-responses, Prolongation of motor latencies, and Prolongation of motor conduction velocities. Conduction block correlates with degree of weakness. CSF: Elevation of protein (may be normal first 10 days). Little or no CSF pleocytosis, unless associated with HIV or Lyme. Management IVIG 0.4 g/kg/day x 5 days Plasma exchange (2–5 exchanges, depending on the severity of the disease) No benefit from corticosteroids Supportive measures ○ ○ ○ ○ ○ ○ Follow vital capacity (VC) and negative inspiratory force (NIF Transfer patient to the I CU and consider elective intubation IF: fVC <20 mL/kg (1.5 L for an average adult) or NIF is worse than –30 cm H2O, Do not wait for O2 saturation or PO2 to drop. Swallowing assessment Cardiac monitoring in all patients who are severely affected, at least until they start to improve. Treat neuropathic pain ○ ○ ○ (gabapentin, pregabalin, or tramadol). Avoid tricyclic antidepressants early, which may lower threshold for arrhythmia. DVT prophylaxis Bowel regimen for constipation Physical therapy to prevent contractures and speed recovery of function Prognosis Overall, 80% of patients recover completely within 3–6 months. Untreated, about 35% of patients have residual weakness, atrophy, hyporeflexia, and facial weakness. Partial recovery followed by relapse occur in <10% of patients. Recurrence after full recovery is 2%. Mortality is 4 %. Poor outcome associated with ○ ○ ○ ○ Older age Preceding diarrheal illness Rapid deterioration and severe weakness Electrically inexcitable nerves and muscle wasting (axonal loss) Other Variants of GBS 2. Acute motor axonal neuropathy (AMAN) ○ Little or no demyelination ○ Often associated with Campylobacter jejuni infection ○ A subset of patients will recover rapidly 3. Acute motor sensory axonal neuropathy (AMSAN) ○ Little or no demyelination ○ Poorer prognosis than AIDP and AMAN 3. Miller Fisher syndrome ○ ○ ○ ○ Ophthalmoplegia Ataxia Areflexia Associated with GQ1b antibody 4. Acute sensory neuropathy 6. Acute pandysautonomia Chronic polyneuropathy A chronic symmetrical polyneuropathy, evolving over months or years, is the most frequently seen form of neuropathy. In about 30% of patients no cause can be established, even after thorough investigation. These patients usually have a mild axonal neuropathy which, whilst causing unpleasant symptoms, does not lead to motor disability. Therefore, if a patient with what seems to be an idiopathic polyneuropathy progresses to significant disability, further thought needs to be given to finding a specific cause (usually inflammatory or genetic). Chronic Demyelinating Polyneuropathy This type of chronic polyneuropathy is often : Hereditary or Immune -mediated (including those caused by abnormal paraproteins). Causes: ○ ○ ○ ○ ○ ○ ○ ○ Hereditary CIDP Lymphoma Osteoclastic myeloma IgM paraproteinaemia Arsenic toxicity Amiodarone toxicity Diphtheria Heriditary Demyelinating Polyneuropathy Many inherited disorders cause demyelinating peripheral neuropathies and one of the best known is Charcot–Marie– Tooth disease (CMT). This neuropathy produces: ○ Distal wasting (‘inverted champagne bottle’ or ‘stork’ legs), ○ Often with pes cavus, and ○ Predominantly motor clinical involvement. ○ In 70–80% the cause is duplication of the PMP-22 gene on chromosome 17 (autosomal dominant CMT type 1) ○ Similar phenotypes are produced by mutations in other genes with differing modes of inheritance CMT Pes cavus, Inverted champagne bottole, Samll muscle atrophy Hereditary peripheral neuropathies Hereditary demyelinating neuropathies Chronic Inflammatory Demyelinating Polyradiculopathy (CIDP) Presents with a relapsing or progressive generalised neuropathy. Sensory, motor or autonomic nerves can be involved but the signs are predominantly motor; A variant causes only motor involvement (multifocal motor neuropathy, MMN). RX Immunosuppressive treatment: Corticosteroids , Methotrexate or Cyclophosphamide , or Plasma exchange Intravenous immunoglobulin, IVIG MMN is best treated by IVIG. Some 10% of patients with acquired demyelinating polyneuropathy have an abnormal serum paraprotein, sometimes associated with a lymphoproliferative malignancy. Treatment flowchart for CIDP Chronic axonal polyneuropathy This is the most common type of chronic polyneuropathy. Where the cause can be found, it is usually a disorder affecting axonal metabolism and transport, either acquired (drugs and toxins) or genetically determined ○ ○ ○ ○ ○ ○ ○ ○ Metabolic/endocrine diseases (including diabetes) Alcohol Drugs and toxins Vitamin deficiency Hereditary IgG paraproteinaemia Paraneoplastic Primary amyloidosis Brachial plexopathy Trauma usually damages either the upper or the lower parts of the brachial plexus, according to the mechanics of the injury. The clinical features depend upon the anatomical site of the damage . Causes of Lower Brachial Plexopathy: ○ Infiltration from breast or apical lung tumours (Pancoast tumour). ○ Therapeutic irradiation ○ Thoracic outlet syndrome: which may be accompanied by circulatory changes in the arm due to subclavian artery compression. Brachial plexus anatomy: L, lateral; M, medial; P, posterior Neuralgic Amyotrophy An acute brachial plexopathy of probable inflammatory origin. In this syndrome, a period of very severe shoulder pain precedes the appearance of a patchy upper brachial plexus lesion. Often affecting the long thoracic nerve which produces winging of the scapula. Recovery occurs over months and is usually complete. Lumbosacral plexopathy May be caused by: Neoplastic infiltration or Compression by retroperitoneal haematomas in patients with a coagulopathy. A small vessel vasculopathy can produce a lumbar plexopathy, especially in elderly patients when it may be the presenting feature of; ○ Type 2 diabetes mellitus (‘diabetic amyotrophy’) or ○ A vasculitis. Spinal Root Lesions Compression at or near their spinal exit foramina by prolapsed intervertebral discs or degenerative spinal disease. Infiltration by spinal and paraspinal tumour masses and Inflammatory or infective processes. The clinical features include: ○ ○ ○ ○ Muscle weakness and wasting and Dermatomal sensory loss with Reflex changes that reflect the pattern of roots involved. Pain in the muscles whose innervating motor roots are involved. Mononeuritis Multiplex Lesions of multiple nerve roots, peripheral nerves or cranial nerves. It is due either to involvement of the vasa nervorum or to malignant infiltration of the nerves. The clinical expression of a very widespread multifocal neuropathy may become confluent so that the clinical picture eventually resembles a polyneuropathy. In this case neurophysiology may be required to identify the multifocal nature of the problem. Causes of Mononeuritis Multiplex Infections: ○ ○ ○ ○ ○ ○ ○ ○ Lyme disease Leprosy Acute viral hepatitis A Hepatitis B Hepatitis C Acute parvovirus B-19 infection Herpes simplex virus infection AIDS and HIV infection Rheumatological: ○ ○ ○ ○ ○ ○ ○ ○ ○ Wegener granulomatosis Henoch-Schönlein syndrome Sjögren syndrome Behçet’s disease Temporal (giant cell) arteritis Systemic lupus erythematosus Rheumatoid arthritis Polyarteritis nodosa Scleroderma Chronic: ○ ○ ○ Diabetes mellitus Amyloidosis[8] Neurosarcoidosis[36, 37] Cancer -related: ○ ○ ○ ○ ○ Chronic graft versus host disease (GVHD) Direct tumor invasion with intraneural spread of Lymphoma B-cell leukemia carcinoid tumor Paraneoplastic – Small cell lung cancer Hematologic: ○ ○ ○ ○ ○ ○ Churg-Strauss syndrome Hypereosinophilia Cryoglobulinemia Hypereosinophilia Atopy-related peripheral neuritis Idiopathic thrombocytopenic purpura Miscellaneous: ○ ○ ○ ○ Amphetamine angiitis Gasoline sniffing Genetic disorder; Tangier disease. Multiple compression neuropathies. Mononeuropathies Facial mononeuropathy (Bell palsy) Weakness: Upper and lower face, inability to close the eye, mouth drawn to the affected side. Patients often describe the face as ‘numb’, but there is no objective somatosensory loss. Loss of direct & consensual corneal reflex on the affected side. Decreased tearing, hyperacusis, and loss of taste to the anterior two thirds of the tongue may be present. Onset is sudden, usually over hours. EMG/NCV are rarely necessary to make the diagnosis, but can be used to determine prognosis. DDx: Herpes zoster, HIV, Lyme, facial tumor, sarcoidosis & neuro-brucellosis. Rx Artificial tears, protective goggles, eye patch at night Prednisone 40–60 mg/d for a week ; speeds recovery if started within 72 hrs. Anti-virals probably not beneficial?? ( Acyclovior 400x5 for 10 days) Prognosis some recovery within 3 weeks(85%). Complete recovery(75%) Poor recovery predicted if: Complete paralysis, Older age Comorbidity; DM , HTN Hyperacusis Loss of taste for > 1wk Reto-auricular pain Axonal loss Aberrant re-innervation may occur during recovery, producing unwanted facial movements such as eye closure when the mouth is moved, or ‘crocodile tears’ (tearing during salivation). Rt LMN VII palsy Hemifacial spasm Usually presents after middle age with intermittent twitching around one eye, spreading ipsilaterally over months or years to affect other parts of the facial muscles. The spasms are exacerbated by talking or eating, or when the patient is under stress. The cause is probably an aberrant arterial loop irritating the nerve just outside the pons. The facial nerve should be imaged to exclude a structural lesion, especially in a young patient. Treatment o Drug is not effective. o Botulinum toxin (repeated every 3 months). o Microvascular decompression. Trigeminal Nerve Lesions Isolated trigeminal sensory neuropathy is rare. It causes unilateral facial sensory loss and is associated in some patients with; oscleroderma, oSjögren’s syndrome or oother connective tissue disorder. Trigeminal neuralgia do not have sensory loss on examination unless there have been operative procedures on the nerve. Herpes Zoster (most frequently in the ophthalmic division) and is followed in about one-third of patients by postherpetic neuralgia). Herpes Zoster Ophthalmicus Entrapment neuropathy Focal compression or entrapment is the usual cause of mononeuropathy. The pressure damages the myelin sheath slowing NCS. Sustained or severe pressure axonal loss loss of sensory AP distal to the site of compression. Causes: Acromegaly , Hypothyroidism , Pregnancy Diabetes Osteophytes HNPP(hereditary neuropathy with liability to pressure palsies) - multiple recurrent entrapment neuropathies, - especially at unusual sites - autosomal dominant Symptoms and signs in common Entrapment Neuropathies Median at wrist (CTS) Ulnar at elbow Meralgaia Paraesthetica Differential diagnosis by pattern of symptoms Pattern 1: Symmetrical proximal and distal weakness with sensory loss. (Consider CIDP, vasculitis.) Pattern 2: Symmetrical distal weakness with sensory loss. (Consider diabetes, drugs and toxins, hereditary neuropathies, amyloidosis, paraproteinemia.) Pattern 3: Asymmetric distal weakness and numbness. (Consider vasculitic neuropathy, HNPP, infectious neuropathy, multifocal trauma or entrapment.) Pattern 4: Asymmetric distal or proximal weakness without sensor loss. (Consider multifocal motor neuropathy, motor neuron disease, inclusion body myositis.) Pattern 5: Asymmetric proximal and distal weakness with sensory loss. (Consider polyradiculopathy or plexopathy, ma ignant infi ltration, brachial neuritis, HNPP.) Pattern 6: Symmetric small fiber sensory neuropathy without weakness. (Consider diabetes, Fabry disease, amyloidosis, HIV.) Pattern 7: Symmetric small and large fiber sensory neuropathy without weakness. (Consider diabetes, drugs, toxins, paraproteinemia.) Pattern 8: Marked proprioceptive sensory loss. (Consider paraneoplastic, B6 toxicity, Sjogren, HIV.) Pattern 9: Autonomic predominant. (Consider autoimmune, amyloidosis, diabetes, AIDP.) Pattern 10: Neuropathy with cranial nerve involvement. (Consider Lyme, HIV, AIDP, sarcoidosis, malignant infiltration, Tangier disease, trichloroethylene toxicity, anti-Gd1b neuropathy.)