Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
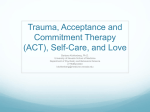
COMPLICATIONS OF TRAUMA ANN O’ROURKE, MD, MPH SCRTAC TRAUMA CARE BEYOND THE ED DECEMBER 4, 2014 Saving Lives By Strengthening Our Region’s Trauma Care System OUR CASE • 31 yo man MVC with prolonged extrication • Presents to ED: • Confused, HR 120, RR35, BP90/65 • Diminished breath sounds on right with palpable chest crepitus • Unequal leg length • Abdominal bruising • What are your concerns? OUR PATIENT • Right hemopneumothorax-facility placed 28Fr chest tube • Liver laceration-managed non-operatively • Right acetabular fracture dislocation with proximal femur fx-traction with planned operation • C3 fracture with small epidural hematomamanaged with PMT collar POST INJURY DAY 2 OUR PATIENT STILL COMPLAINS OF DIFFICULTY BREATHING • What are your concerns? • Worsening pulmonary contusion • Pneumothorax • Hemothorax • Pain from fractures • Abdominal fluid/blood • Pneumonia/pneumonitis • Pulmonary embolism RETAINED HEMOTHORAX • Our chest tube did a good job of evacuating air and most of the blood, but some clotted blood remained. This can lead to: • Empyema • Chronic fibrothorax with trapped lung RETAINED HEMOTHORAX Prevention: • Properly positioned, LARGE chest tube (36-42Fr) • Post placement CXR • Retained hemothorax post chest tube placement independent predictor of empyema in up to 33% of patients RETAINED HEMOTHORAX Treatment: • Operative • Early VATS (3days) significant reduction in operative difficulty, contamination/infection of clot, and hospital length • After day 5 more likely to need thoracotomy • Fibrinolytic • VATS is a more effective procedure than intrapleural streptokinase • VATS patients having a statistically significant shorter hospital stay and decreased need for additional therapy • Fibrinolytic agents would have to be seen as a second-line agent behind surgery when the risks of surgery are too great to the patient’s overall outcome EMPYEMA • • Approximately 3% of patients with chest trauma will develop a posttraumatic empyema. Risk factors • persistent pleural effusion/hemothorax • duration of a tube • placement of multiple tubes • • No good evidence for or against prophylactic abx prior to chest tube for prevention As with retained hemothorax, first line treatment is operative in patients who will tolerate EMPYEMA PNEUMONIA • Our patient had difficulty coughing and clearing secretions • What risk factors for this? • Rib fractures with impaired mechanics • Pulmonary contusion • Inadequate analgesia • C-collar impaired swallowing FROM THE NTDB ALL AGES Half-a-dozen ribs: The breakpoint for mortality. Flagel, et al. Surgery 2005;138:717-25 RIB FRACTURE CORRELATION WITH MORTALITY Half-a-dozen ribs: The breakpoint for mortality. Flagel, et al. Surgery 2005;138:717-25 OUR PATIENT DEVELOPED RLE SWELLING • What are your concerns? • DVT • Compartment syndrome • Morel-Lavallée DVT • What are his risk factors for DVT? • Prolonged extrication • Immobility • LE/pelvic fracture • Holding DVT prophylaxis WHEN SHOULD WE BEGIN DVT PROPHYLAXIS? AND WHAT MEDICATION DO WE USE? • What factors in to the decision for this patient? • Solid organ injury (liver) • Pelvic fracture • Spinal epidural hematoma • Other factors: • Head bleed • Planned operations • Epidural catheters DVT PROPHYLAXIS IN SOLID ORGAN INJURY • DVT prophylaxis is safe in patients with solid organ injury • BUT timing of initiation is not established • Some retrospective trials suggest OK to begin early DVT PROPHYLAXIS IN TRAUMA MOREL-LAVALLÉE OUR PATIENT DEVELOPS ABDOMINAL PAIN, TACHYCARDIA AND FEVER • What are your concerns? • Biloma/bile leak • Missed bowel injury • Delayed bleed • Urinary tract infection • Hepatic necrosis • Abscess • Cholecystitis DELAYED LIVER COMPLICATIONS • Delayed bleed 1-6% severe liver injuries • Expanding bleed • Pseudoaneurysm • Biliary leak 2-7% • Mean 7-10d post injury • Most in grade 4-5 injuries • Treat with drainage and ERCP and stent BILIARY COMPLICATIONS Table 2 Analysis of factors influenced development of complications, including biliary complications in the study group Complications No complications Biliary complications (n = 22) (n = 24) (n = 15) 17 17 13 NS 23.7 ± 11.9 20.6 ± 15 22.5 ± 12.2 NS ISS (mean ± SD) 36 ± 14 32.6 ± 15 35 ± 15 NS Grade of liver injury (mean ± SD) 4 ± 0.6 3.8 ± 0.6 4 ± 0.75 NS Angioembolization (%) 6 (27.2) 5 (20.8) 5 (33.3) NS 15 (68.2)* 8 (33.3) 9 (60) 0.038 7 (31.8) 5 (20.8) 5 (33.3) NS Male Age (years) OR (%) Penetrating injury (%) P value OR - operative group; ISS - Injury severity score; NS - Differences not significant; * - p < 0.05 - complication rate was higher in OR patients. Bala et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2012 20:20 doi:10.1186/1757-7241-20-20 SMALL BOWEL INJURY MISSED SMALL BOWEL INJURY OUR PATIENT DEVELOPS MENTAL STATUS CHANGES • What are your concerns? • Hypoxia or hypercarbia • Sepsis • Stroke • Medications • Drug withdrawal BLUNT CEREBROVASCULAR INJURY BCVI OUR PATIENT IS BACK IN CLINIC WITH SLEEP DISTURBANCES • What are your concerns • Inadequately treated pain • Medication withdrawal • Post traumatic stress disorder • Sleep apnea • Insomnia related to stroke PTSD IN CIVILIAN TRAUMA • More than 20% of trauma patients have PTSD at 12 months following injury • Risk factors: • Post-injury emotional distress • Pain • Pre-injury depression • Benzodiazepine use Zatzick, et al. Annals of Surgery • Volume 248, Number 3, September 2008 PTSD CRITERIA • Historically, benzodiazepines were used for treatment of acute stress and ptsd • change: use with caution or discourage use • theoretical, animal, and human evidence to suggest that benzodiazepines may actually interfere with the extinction of fear conditioning or potentiate the acquisition of fear responses and worsen recovery from trauma • Very high co-morbidity of PTSD with alcohol misuse and substance use disorders (upwards of 50 percent of co-morbidity) and potential problems with tolerance and dependence. • Once initiated, benzodiazepines can be very difficult, if not impossible, to discontinue due to significant withdrawal symptoms compounded by the underlying PTSD symptoms.