Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
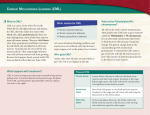
CML
Chronic myelogenous leukemia
CML accounts for 15 - 20% of all leukemias affecting adults
Hematopoietic Progenitors and CML
Acquisition of the
Philadelphia
Chromosome
Leukocytosis with the presence of precursor cells of the myeloid lineage. In addition,
basophilia, eosinophilia, and thrombocytosis can be seen
whole granulocytic lineage, including an eosinophil and a basophil
A promyelocyte, an eosinophil, and 3 basophils
Diagnostic Considerations in CML
A peripheral blood smear or bone marrow aspirate can only give a
presumptive diagnosis of CML – one still needs to confirm the
presence of the t (9 ; 22)
Common Peripheral Blood Findings
1.
Leukocytosis with a ‘left shift’
2.
Normocytic anemia
3.
Thrombocytosis in ~ 50% of patients
4.
Absolute eosinophilia
5.
Absolute and relative increase in
basophils
6.
LAP score is low (not frequently
employed today)
LAP = leukocyte alkaline phosphatase.
Most CML Patients Are Diagnosed
in the Chronic Phase
Chronic Phase
Blast Phase
CML
Bone marrow film at 400X magnification demonstrates clear dominance of
granulopoiesis. The number of eosinophils and megakaryocytes is increased
Ph Is the Result of t(9;22)(q34;q11)
{
q11
BCR
BCR
ABL
Ph
22
{
q34
ABL
9
ABL
BCR
9q+
The ABL oncogene encodes a tyrosine protein kinase. The resulting BCR/ABL
fusion gene encodes a chimeric protein with strong tyrosine kinase activity.
p210Bcr-Abl Alone Is Necessary and
Sufficient for Development of CML
p210Bcr-Abl
I.
Two forms of the BCR/ABL mutation have been identified.
II. These vary according to the location of their joining regions on bcr
3' domain.
III. Approximately 70% of patients who have the 5' DNA breakpoint
have a b2a2 RNA message
IV. And 30% of patients have a 3' DNA breakpoint and a b3a2 RNA
message. The latter is associated with a shorter chronic phase,
shorter survival, and thrombocytosis
Additional chromosomal abnormalities, such as an additional or double Ph1-positive
chromosome or trisomy 8, 9, 19, or 21; isochromosome 17; or deletion of the Y
chromosome, have been described as the patient enters a transitional form or
accelerated phase of the blast crisis as the Ph chromosome persists.
CML: Epidemiology and Etiology
•
In the US, there were 4,870 cases in 2010 and an expected
5,430 cases in 2012
• Most patients present in CP
• Majority of CML-related deaths due to progression to AP/BC
• 50% of CML patients are asymptomatic at diagnosis
Epidemiology and Etiology
Incidence increases significantly
with age
– Median age: ~ 67 yrs
Risk factors
– Prior high-dose radiation exposure
– Exposure to certain organic solvents
• Benzene
• Carbon tetrachloride
– Age
– Gender (male > female ~ 1.4:1)
– Majority of cases have no known
inciting factor
Approximate US Prevalence of the
4 Major Types of Leukemia as of 1/1/07
Signs and symptoms in the chronic
phase are as follows:
• Fatigue, weight loss, loss of energy, decreased exercise tolerance
• Low-grade fever and excessive sweating from hypermetabolism
•
•
•
•
Elevated (WBC)
Splenomegaly
Hepatomegaly
Early satiety and decreased food intake from encroachment on
stomach by enlarged spleen
• Left upper quadrant abdominal pain from spleen infarction
signs and symptoms of progressive
disease:
• Bleeding, petechiae, and ecchymoses during the
acute phase
• Bone pain and fever in the blast phase
• Increasing anemia, thrombocytopenia, basophilia,
and a rapidly enlarging spleen in blast crisis
Blood count and peripheral smear findings
• WBC 20,000-60,000 cells/μL, mildly increased basophils and
eosinophils
• Mild to moderate anemia, usually normochromic and normocytic
• Platelet counts low, normal, or increased
• Leukocyte alkaline phosphatase stains very low to absent in most
cells
• Leukoerythroblastosis, with circulating immature cells from the
bone marrow
• Early myeloid cells (eg, myeloblasts, myelocytes, metamyelocytes,
nucleated red blood cells)
Bone marrow findings
• Philadelphia (Ph) chromosome (a reciprocal translocation
of chromosomal material between chromosomes 9 and
22)
• BCR/ABL mutation
• Hypercellularity, with expansion of the myeloid cell line
(eg, neutrophils, eosinophils, basophils) and its progenitor
cells
• Megakaryocytes are prominent and may be increased
• Mild fibrosis in the reticulin stain
Sokal score
widely used prognostic index, is calculated for
patients aged 5-84 years by the following equation:
Hazard ratio = exp 0.0116 (age - 43) + 0 .0345 (spleen size
[cm below costal margin] - 7.5 cm) + 0.188 [(platelet
count/700)2 - 0.563] + 0.0887 (% blasts in blood - 2.1)
• Good risk (average survival of 5-6 years)
• Intermediate risk (average survival of 3-4 years)
• Poor risk (average survival of 2 years)
3 categories of the Sokal score
• Low risk: score < 0.8
• Intermediate risk: score 0.8-1.2
• High risk: score > 1.2
The Sokal score correlates with the likelihood of
achieving complete cytogenetic response, as follows:
• Low-risk patients: 91%
• Intermediate-risk patients: 84%
• High-risk patients: 69%
Poor-prognosis characteristics
Clinical and laboratory factors
•
•
•
•
•
•
•
•
•
•
•
•
•
Older age
Symptomatic presentation
Poor performance status
African American descent
Hepatomegaly
Splenomegaly
Negative Ph chromosome or BCR/ABL
Anemia
Thrombocytopenia
Thrombocytosis
Decreased megakaryocytes
Basophilia
Myelofibrosis (increased reticulin or collagen)
Therapy-associated factors may indicate a
poor prognosis in patients with CML:
• Longer time to hematologic remission with
myelosuppression therapy
• Short duration of remission
• High total dose of hydroxyurea or busulfan
• Poor suppression of Ph-positive cells by
chemotherapy or interferon alfa therapy
Physical Examination
• Splenomegaly correlates with the peripheral blood granulocyte
counts
• A very large spleen is usually a harbinger of the transformation
into an acute blast crisis form of the disease.
• Hepatomegaly also occurs, although less commonly than
splenomegaly.
• Leukostasis and hyperviscosity can occur in some patients, with
extraordinary elevation of their WBC counts, exceeding
300,000-600,000 cells/μL. Upon funduscopy, the retina may
show papilledema, venous obstruction, and hemorrhages.
Blast crisis
• Increase in the bone marrow or peripheral blood blast
count or by the development of soft-tissue or skin leukemic
infiltrates.
• Typical symptoms are due to increasing anemia,
thrombocytopenia, basophilia, a rapidly enlarging spleen
• Failure of the usual medications to control leukocytosis
and splenomegaly.
Leukocyte Alkaline
Phosphatase (LAP)
Naphthol AS-MX phosphate LAP at pH8.6 >
Naphthol AS-MX + Diazonium salt
(eg, Fast blue RR)
> Insoluble pigment
LAP Score
Count 100 consecutive segs and bands
• Score:
0 = no granules
1+ = occasional diffuse granules
2+ = moderate number of granules
3+ = many strongly positive granules
4+ = confluent strongly positive granules
0
2+
1+
3+
4+
LAP Score
Example:
0
1+
2+
3+
4+
x
x
x
x
x
35 cells
30 cells
20 cells
10 cells
5 cells
=
=
=
=
=
0
30
40
30
20
120 LAP Score
Bcr-Abl Translocation and CML
Philadelphia Chromosome
ABL-BCR Fusion Gene
NCI, 2011.
The Cytogenetic Hallmark of CML
Is the Philadelphia Chromosome
9q+
Ph
9
22
22q- = Ph chromosome
FISH showing the BCR (green), ABL (orange), and BCR-ABL fusion
signals (arrow): A=positive (contains a residual ABL signal), B=normal
Small Molecule TKIs
Molecular Mechanisms of
BCR-ABL Induced Leukemogenesis
Marley et al, 2005.
RT-PCR for BCR-ABL
Target
sequence
1 Denaturation:
RT-PCR for BCR-ABL in CML
Heat briefly to
separate DNA
strands
2 Annealing: Cool
1)
2)
3)
4)
Qualitative RT-PCR allows for the
diagnosis of CML
Cycle 1
yields 2
molecules
Quantitative RT-PCR is used to
quantify the amount of disease
Allows for the identification of
cryptic BCR-ABL translocations
Does not require a bone marrow
aspirate for optimal results
RT-PCR = real time polymerase chain reaction.
to allow primers
to form hydrogen
bond with ends
of target
sequence
Primers
3 Extension: DNA
polymerase adds
nucleotides to the
3” end of each
primer
Cycle 2
yields 4
molecules
Cycle 3 yields
8 molecules;
2 molecules
(in white
boxes)
match target
sequence
New
nucleotides
Monitoring Response:
Sensitivity of Strategies
100%
Diagnosis: 1012 Leukemia Cells
Complete
Hematologic
Response
Blood Counts
10%
Cytogenetics
1%
PCR
0.1%
4.5 log = 0.0032%
Undetectable Range
Complete
Cytogenetic
Response
Major
Molecular
Response
Complete
Molecular
Response
BCR-ABL Kinase Activity Is Essential for
CML Pathogenesis
L
AB
R
BC
0
1
2
Imatinib (mM)
0.1
0.5
1.0
5.0
BCR-ABL-
2 D p
6
K5 32 32
BCR-ABL
NALM-1 cells (Ph+)
10
NCCN Recommendations
for Evaluation of Possible CML
Consideration for
a diagnosis of CML
H&P including documentation of spleen size
CBC, platelets
Chemistries
HLA typing
Bone marrow aspirate and biopsy including
–
–
–
–
aKaryotyping
Aspirate for blast percentage
Karyotypea
FISHb
Quantitative RT-PCR for Bcr-Ablc
is recommended to identify additional chromosomal changes not detectable by FISH; including CE,
complex translocations, and Ph(-) ACAs.
bFISH is acceptable for confirming the diagnosis of CML when BMB is not feasible.
cqRT-PCR is recommended to establish a baseline since the majority of labs do not use the International Scale.
qRT-PCR = quantitative real-time polymerase chain reaction; CE = clonal evolution; ACAs = additional
chromosomal abnormalities;
Treatment Milestones for CML
Definitions of Responses to Treatments
Hematologic Response
Complete Hematologic response
Amount of Dz
1X1012
1X1011
1) Normal PB counts (WBC < 10 x 109/L and plts < 450 x 109/L)
2) Normal WBC differential
3) No Dz symptoms
4) Normalization of the size of the liver and spleen
Cytogenetic Responses: Ph+ Metaphases
1) Complete: 0%
1X1010
2) Partial: 1%–35%
3) Minor: 36%–65%
4) Minimal: 66%–95%
5) None: 96%–100%
Molecular Responses: Ratio of Bcr-Abl/Abl
Major Molecular Response
≥ 3-log10 reduction from initial diagnosis sample
(ie, 25 → 0.025)
1X10 8-9
Responses Correlate With
Decreasing Burden of Disease
RT-PCR = real-time polymerase chain reaction; Dx = diagnosis.
Options for Establishing the Diagnosis of CML
Karyotyping
Requires BM aspirate for optimal
metaphases
Allows for evaluation of CE as
well ACA in Ph- clones
Occasionally, cryptic and complex
translocation events may
result in the missed
identification of t(9;22)
FISH
Can be done with interphase
cells
Allows for the identification of
potential duplications of the
Ph chromosome
Allows for the identification of
the loss of der(9) chromosome
Allows for the identification of
cryptic translocations involving
BCR-ABL that can be missed
on karyotypes
Fails to identify CE or ACA
BM = bone marrow; CE = clonal evolution; ACA = additional chromosomal abnormatlities. .
qRT-PCR
Can quantify the amount of
disease
Allows for the identification of
cryptic translocations involving
BCR-ABL
Many primers sets only detect
the p190 and/or p210 translocation
and may miss p230 or alternative
translocations
Requires consistent use of the
same laboratory give different
control genes
Fails to identify CE or ACA
Role of the Bone Marrow Biopsy in the
Diagnosis of CML
One Disease – Three Phases
Chronic Phase
• Myeloproliferative neoplasm associated with the balanced
chromosomal translocation between the long arms of Chromosome 9
and 22 [t(9;22)(q34;q11.2)]
• < 10% of the cells in the blood and bone marrow are blast cells
(immature blood cells)
Accelerated Phase
• Blasts 10%–19% of WBCs in peripheral and/or nucleated bone
marrow cells
• Peripheral blood basophils ≥ 20%
• Persistant thrombocytopenia (< 100 x 109/L) unrelated to therapy, or
persistent thrombocytosis (> 1,000 x 109/L) unresponsive to therapy
• Increasing spleen size and increasing WBC count unresponsive to
therapy
• Cytogenetic evidence of clonal evolution
Blast Crisis
• Blasts ≥ 20% of peripheral blood white cells or of nucleated bone
marrow cells
• Extramedullary blast proliferation
• Large foci or clusters of blasts in the bone marrow biopsy
Imatinib Greatly Improved Survival
in CML-CP (MDACC data)
Diagnostic Considerations
Problems to be considered include the following:
Acute myeloid leukemia
Chronic myelomonocytic leukemia
Chronic neutrophilic leukemia
Thrombocythemia
Leukemoid reactions from infections (chronic
granulomatous [eg, tuberculosis])
Tumor necrosis
Differential Diagnoses
Agnogenic
Myeloid Metaplasia With
Myelofibrosis
Essential
Thrombocytosis
Myelodysplastic
Syndrome
Myeloproliferative
Polycythemia
Disease
Vera
Management
Goals of treatment of CML include the following:
Hematologic remission (normal CBC and physical
examination [ie, no organomegaly])
Cytogenetic remission (normal chromosome
returns with 0% Ph-positive cells)
Molecular remission (negative polymerase chain
reaction [PCR] result for BCR/ABL mRNA
Goals of treatment
Hematologic remission normal CBC and physical
examination ie, no organomegaly
Cytogenetic remission (normal chromosome
returns with 0% Ph-positive cells)
Molecular remission (negative polymerase chain
reaction [PCR] result for the mutational BCR/ABL
mRNA), which represents an attempt for cure and
prolongation of patient survival
Tyrosine kinase inhibitors for CML
Imatinib mesylate (Gleevec): For chronic,
accelerated, and blastic phases; standard
treatment of choice
Dasatinib (Sprycel): For chronic phase
Nilotinib (Tasigna): For chronic phase
Bosutinib (Bosulif): For chronic, accelerated, and
blast phases
Ponatinib (Iclusig): For chronic, accelerated, and
blast phases
Other medications for CML
Interferon-alfa: Former first-line agent; now
combined with newer drugs for refractory cases
Hydroxyurea (Hydrea): Myelosuppressive agent
for inducing hematologic remission
Busulfan: Myelosuppressive agent for inducing
hematologic remission
Omacetaxine (Synribo): Protein translation
inhibitor indicated for chronic- or acceleratedphase CML with resistance and/or intolerance to 2
or more tyrosine kinase inhibitors
Treatment recommendations for
Chronic phase
Dasatinib 100 mg PO once daily or
Nilotinib 300 mg PO twice daily or
Imatinib 400 mg PO once daily or
Bosutinib 500 mg PO once daily or
Ponatinib 45 mg PO once daily
Accelerated / blast phase
Dasatinib 140 mg once daily or
Nilotinib 400 mg twice daily or
Imatinib 600-800 mg PO once daily or
Bosutinib 500 mg PO once daily or
Ponatinib 45 mg PO once daily
There is a high relapse rate in patients in accelerated phase even after
successful treatment; transplantation should be considered
Blast phase:
Patients in lymphoid blast phase can be treated with acute
lymphoblastic leukemia (ALL) induction chemotherapy
regimens in combination with a tyrosine kinase inhibitor
Patients in myeloid blast crisis can be treated with acute
myeloid leukemia (AML) induction chemotherapy regimens
in combination with a tyrosine kinase inhibitor; some
patients can be treated with a tyrosine kinase inhibitor
alone
Allogeneic bone marrow transplantation
(BMT) or stem cell transplantation
Only proven cure for CML
Ideally performed in the chronic phase
Candidate patients should be offered the procedure if they have
a matched or single–antigen-mismatched related donor
available
Overall survival for allogeneic BMT with matched unrelated
donors ranges from 31% to 43% for patients younger than 30
years and from 14% to 27% for older patients
Currently relegated to patients who do not achieve molecular
remissions or show resistance to imatinib and failure of secondgeneration tyrosine kinase inhibitors (eg, dasatinib)