Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
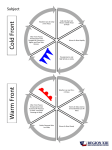
WARM ANAESTHESIA GREETINGS Dr . S.PARTHASARATHY MD., DA., DNB Dip. Diab. DCA, Dip. Software statistics PhD (physio) Mahatma Gandhi medical college and research institute , puducherry – India Why temperature?? Start with some tempo? No Temperature is a vital sign!! History 1776 – John hunter first measured temperature 1895 – Harvey cushing measured temperature in anaesthesia Skin and core Skin temperature – surface of the skin Core temperature – temperature of blood in Main pulmonary artery. Skin usually less than core Normal 37*C± 0.2 Core – naso pharygeal, distal esophagus, tympanic, Rectal bladder , axillay and oral also All other skin surface – skin temperature Normal regulation Sensors: Cells through out the body ,abdomen and thoracic tissues, ↓ Anterior hypothalamus: ↓ Posterior hypothalamus ↓ Effector organs Cold – A delta fibres Warm – C fibres Vasoconstriction – AV shunts Nutrition? BP ? Cold warm Behavioural Vasoconstriction Shivering Nonshivering.Th. anaest. Normal behavioural vasodilation sweating anaest -----------I-----------I-------I------------I-------------33 37 39 Heat loss Radiation – infra red Convection – movement of air Conduction –contact loss Evaporation – as water vapour Nonshivering thermogenesis Non-shivering thermogenesis usually occurs in brown adipose tissue (brown fat) that is present in human infants (between scapulae) uncouples oxidative phosphorylation, and the energy is dissipated as heat rather than producing ATP from ADP Hypothermia Anything below 36.7 !! But -- clinically below 35 Severe -- when below 32 Feel of the cold Hypo – what does it do?? ↓ liver blood flow ↓ renal blood flow ↑ blood viscosity Shift of ODC Adrenergic surge Drug metabolism altered Hypo – what does it do?? ↓ Cerebral blood flow ↓ heart rate. ↑ contractility ↓ Cardiac output Defib – ineffective ↓ ADH – cold diuresis pH measurement ?? Corrected. Periop Hypo – what does it do?? Wound infection is more Bleeding more Recovery delayed- Anaesth. and Relaxants more action Mortality and cardiac events more. Shivering and its problems Some advantages But it does give better outcomes in neuro protection Intracranial aneurysm surgery It is useful in cardiac anaesthesia Operating room – what does it do?? Cold environment, IV fluids Laminar flow Regional anaes. - vasodilation Body cavities washed with NS. Anaesthesia widens gap and relaxants inhibit shivering With the exception of Ketamine all general anaesthetics impair thermoregulation I unit blood or 1 litre crystalloid administered at room temp. ↓ core temp by 0.25* C Hypothermia during GA develops with a characteristic pattern An initial rapid decrease in core temperature core-to-peripheral redistribution of body heat. Then - slow, linear reduction in core temperature that results simply from heat loss exceeding heat production. core temperature stabilizes and subsequently remains virtually unchanged. This plateau phase Regional Prevents vosoconstriction and shiverring Cold receptors – concentrated in the legs Hypothermic patient feeling warm sometimes – clinical paradox. Incidence of hypo-- 60% ?? Prevention Radiant heat lamps. Warm blankets. Warm OR Closed circuit. Warm IV fluids. Forced air circulation –the best Humidifiers Heat and Moisture Exchangers ( HMEs) Oesophageal Rewarmers These devices consist of a double lumen esophageal tube through which water is circulated at upto 42°C Blankets- IV warmer- warmed IVF shivering involuntary contractions of muscles, in response to the chilling effect of low temperatures. Shivering may also occur at the onset of a fever when the body's heat balance is disturbed. Tonic phase 4-8 cycles/min. Clonic phase. 5-7 Hz Clonic phase may resemble fits. Incidence 40% Clonic more common after inh. Agents Nonthermoregulatory tremors in labour. shivering ↑ IOT ↑ ICT ↑ O2 consumption Hence a big no in IHD patients. Shivering – treatment Clonidine 75 µg Pethidine 25 mg Tramadol 50 mg Ondansetron 4 mg IV Others like doxapram, ketanserin,physostigmine,magsulf used. Hence the mechanism of shivering!! After cold, we move to hot Hyperthermia Atropine,ether, allergy, mismatched blood infection, inflammation Blood in 4th ventricle. Atropine and sweating!! To cool, Refrigerated IV fluids. Endovascular cooling with heat exchange catheters Malignant hyperthermia!! is a rare life-threatening condition triggered by exposure to IAS skeletal muscle oxidative metabolism, which overwhelms the body's capacity to supply oxygen, remove carbon dioxide, and regulate body temperature, eventually leading to circulatory collapse and death if not treated quickly. Symptoms Autosomal dominant Males more 1:20,000 Masseter spasm and ↑ ETCO2 Tachycardia, tachypnoea, arrythmias, unstable BP, hyperkalemia ,myoglobinuria renal failure coma C O D S C U P- pneumonic Circuit Oxygen Dantrolene 3 mg/kg , Azumolene is a 30-fold more water-soluble analogue of dantrolene Supportive measures,Soda bicarb Cold washes Urine – mannitol, frusemide. Potassium disturbance Preop check up Family history. ↑ CPK Positive muscle biopsy Avoid IAS Probes Thermistors are made from certain metal oxides whose resistance decreases with increasing temperature. resistance falls off with increasing temperature Thermocouples are based on the effect that the junction between two different metals produces a voltage which increases with temperature. clear advantage of a higher upper temperature limit, up to several thousand degrees Celsius. Indications of temp. monitoring Adults – surgery more than 30 minutes All children. Major iv shifts Nasopharygeal or axillary is ok Carry home message Temperature is a vital sign. Hypo and hyperthermia has significant dangerous repercussions in anaesthesia Are we monitoring? Are we taking precautions? Are we noting morbidity?? Thank you