Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
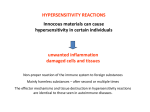
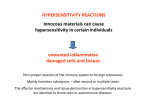
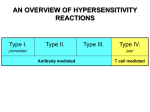
HYPERSENSITIVITY REACTIONS HYPERSENSITIVITY REACTIONS Innocous materials can cause hypersensitivity in certain individuals unwanted inflammation damaged cells and tissues Non-proper reaction of the immune system to foreign substances Mainly harmless substances – after second or multiple times TYPES OF HYPERSENSITIVITY REACTIONS Type I Type II Type III Type IV „immediate” „delayed” Antibody mediated T cell mediated specific IgE cell surface antigen specifically reacting with antibody aspecifically deposited soluble immuncomplex MHC restricted T cell activation mediators produced by mast cells FcR mediated inflammation, inhibition of cell functions FcR mediated complement activation, inflammation cytokines, cytotoxicity „classic allergy” newborn haemolytic anaemia, penicillin sensitivity, M. gravis Serum sickness, SLE Contact dermatitis mostly appear together with autoimmune diseases TYPES OF HYPERSENSITIVITY REACTIONS HYPERSENSITIVITY REACTIONS TYPE I ALLERGY TYPE II TYPE III Soluble antigen Cell surface or matrix antigen Soluble antigen IgE Mast cell Hay fever Asthma Systemic anaphylaxis IgG – immune complex FcγR+ cells NK, macrophage Certain drug allergies (penicillin) IgG – immune complex FcγR+ cells Complement Serum sickness Arthus reaction TYPE I HYPERSENSITIVITY REACTION ALLERGY ALLERGENES USUALLY ENTER THE BODY VIA MUCOSAL SURFACES AND THEY ARE PRESENT AT A LOW DOSE DC B cell Th2 Th2 antigen presentation T cell priming and polarization allergy response soluble proteins on te surface of small particles (pollen, dust mite „drops”) small Mol. Weight, soluble trans mucosal entry, enzymatic activity low dose (ragweed: 1µg/year) Mechanism of the initiation of Th2 response IL-4 DC CD4+ T h2T CD40L IL-4 A L L E R G É N Allergen Th2 C D 4 0 nyá lka Mucosa há rtya IL-10 CD40L B C D 4 0 M H CII B IgE Mast cell degranulation, wheel and flare reaction Ragweed Saline Histamine IgE a g b I I TT AA MM PLA2 foszfa tidil-kolin LYSO-PC arachidonsav Fc eRI I T A M MAPkináz I T A M Lyn MAST CELL RESPONSE TO SURFACE FcRεI CROSSLINKING II TT AA MM Syk endoplazmás retikulum 2 Ca + 5-lipoxigenáz PIP2 PI-PLCg DAG IP3 foszfolipid ciklooxigenáz Ca 2+ PGD2 citokin gének transzkripciója LTC4 NFAT AP-1 NF-k B PAF szekretoros granulum 2+ PKC Ca Ca 2+ proteinek (miozinkönnyűlánc) foszforilációja Ca 2+ szekréció PGD2 LTC4 EARLY MEDIATORS LTD4 LTE4 LATE MEDIATORS mediátorok citokinek IL-3, IL-4, IL-5, IL-6 TNFa Biognic amins – histamin Enzymes – triptase, chymase, carboxypeptidase The effect of mast cell degranulation varies with the tissue exposed to allergen Systemic anaphylaxis is caused by allergens that reach the blood stream GENETIC/ENVIRONMENTAL PREDISPOSITION TO ALLERGY Genetic factors chromosome 11q FcERβ chain gene chromosome 11q IL-3-5 IL-9, IL13 GMCSF HLAII DRB1*150 Improper immunregulation Th1/Th2 inbalance regulation of IgE synthesis immunodeficiency high eosinophil counts allergy Environmental factors lack of tolerance Types of IgE-derived allergic response SYNDROME ALLERGENS ROUTE OF ENTRY RESPONSE systemic anaphylaxis drugs anti-serum peanuts intravenous peroral edema, increased vascular permeability tracheal occlusion circulatory collapse, death acute utricaria bug bite allergy test subcutan local increase in blood flow and vascular permeability allergic rhynitis pollen dust mite drops inhaled irritation and edema of nasal mucosa airway inflammation asthma animal fur pollen dust mite drops inhaled bronchial constriction, increased mucus production food allergy nut, peanuts, fish, shellfish milk, eggs peroral vomiting, diarrhea pruritis (itching) urticaria (hives) anaphylaxia (rare) Short/Common ragweed (Ambrosia artemisiifolia) Short/Common ragweed (Ambrosia artemisiifolia) levélfonák zöld Mugwort (Artemisia vulgaris) levélfonák fehéresen molyhos Mugwort (Artemisia vulgaris) Mugwort (Artemisia vulgaris) – ? Wormwood (Arthemisia absinthium) – Absinthe (thujone: max 35 mg/l) HYPERSENSITIVITY REACTIONS INDUCED BY IMMUNE COMPLEXES TYPES II and III Type II hypersensitivity IgG tpye antibodies bound to the cell surface or to tissue antigens • cells expressing the antigen become sensitive to complement mediated lysis or to opsonized phagocytosis • frustrated phagocytosiss tissue demage • the antibody inhibits or stimulates target cell function – no tissue damage (e.g. M. gravis – receptor blocker antibodies) MECHANISMS OF TYPE II HYPERSENSITIVITY REACTIONS Hemolytic anemia of newborns Erythroblastosis fetalis NK Mf Killing of target cell by effectormacrophage or NK-cell IgG ADCC IgG C' complement activation Killing of target cell by complementmediated lysis Receptor-specific autoantibody interferes with signal transduction Drug induced Hemolytic anemia Trombocytopenia Agranulocytosis Penicillin-based antibiotics Anti-arythmic quinidin Goodpasture syndrome (type IV collagen) Pemphigus vulgaris (desmosomal antigens) Damage of epidermal and mucosal junctions, acantholysis MECHANISM OF THE DEVELOPMENT OF DRUG SENSITIVITY Th B Healthy cell Drug-modified cell surface protein IgG type antibodies FRUSTRATED PHAGOCYTOSIS MEDIATED BY IgG TYPE ANTIBODIES Binding Opsonization Internalization C3b C3b C3b C3b Enzyme release C3b C3R FcR The tissue, which can not be phagocytosed, is damaged C3b Internal or absorbed antigen Opsonized surface Binding Frustrated Enzyme release phagocytosis (drug) Examples - Type II hypersensitivity Newborn haemolytic anaemia Transfusion reaction Hyperacut allograft rejection Drug-derived • Haemolitic anaemia • Thrombocytopenia • Agranulocitosis • • Penicillin-based antibiotics Anti-arithmic quinidin Goodpasture syndrome (kidney, membrane basalis, collagen type IV) Myasthaenia gravis (anti-acetyl-choline receptor antibodies) Basedow-disease (anti-TSH-receptor antibodies) Pemphigus vulgaris (mucosal bubbles) atoantibody against desmosomal antigen desmoglein-3, interruption of epidermal and mucosal connections, acantolysis (disintegration into single cells) Transplantation - hyperacut allograft rejection • HLA-A, B, C, DR, DQ, DP, minor histocompatibility antigens • foreign MHC-antigens recognized by T cells Direct: self T cells - donor APCs (CD8+ T cells) Indirect: self APC presents donor MHC-molecule fragments (CD4+ T cells) cytokine release • Hyperacut rejection Causes: immunization against alloantigens, preformed antiHLA-antibodies, blood group incompatibility antibodies bound to endothel activation of complement system thrombosis of venules vascularis necrosis Therapy resistent MHC I: MHC II: HLA typing HLA-A, HLA-B, HLA-C HLA-DP, HLA-DQ, HLA-DR - used for transplantations (generally the -B and -DR is the most important and the -C does not matter) - diagnostical value (connections between the HLA alleles and the diseases) Serotyping (microcitotoxicity tests) Based on the serological reaction between the examined cells and the typing serum. Complement mediated lysis with the help of MHC I and/or MHC II antigen recognizing antibody containing serum. There are no reaction in the case of serotype identity (dead cells can be visualized by specific dye) Typing sera containing antibodies to Class I and II proteins were collected from multiparous women, or individuals who had received multiple blood transfusions. (immunized against multiple alleles). The specificity identification have been done on international workshops. The procedures have been done on microtiter plates (with 10µl working aliquots – Terasaki plates) because of the available quantity of the typing sera were always limited. Sera have been replaced by monoclonal antibodies later. Serotyping (2.) HLA-D (MHC II) antigenes had been examined on nylon column separated B cells The polymorphism of the MHC II antigens could be examined by mixed lymphocyte reactions (MLR). (A normal person can have 1-10% alloreactive lymphocytes.) Microtiter plates serotyping have some limits – crossreactions (HLA-B27 – HLA-B7) – there is no sera against HLA-C because of the low immunogenicity – some subtype cannot be discriminated Genomic DNA based examinations - PCR-SSP is using the PCR amplification reaction directly to detect HLA polymorphisms. Primers can be constructed specifically to complement HLA polymorphisms; if the primers bind the complementary polymorphism and amplify the gene segment, then the PCR product can be detected by standard techniques. An array of PCR primers complementary to the range of HLA polymorphisms has been constructed. HLA-A 0201 0202 0203 … -PCR-SSOP (sequence specific oligonucleotid probe) The examined HLA genes are amplified by PCR with non allele specific primer pairs. The amplificates are immobilized on nitrocellulose membranes or microtiter plates and are hybridized by HLA allele specific labeled oligonucleotides. The label can be enzimatic, fluorescent or radioactive -SBT (sequence based typing) allotypes can be evaluated by sequencing MHC region of the genomic DNA (minor mutations can be examined) Diseases (autoimmune) HLA frequency concerned control SLE DR3 B8 55 50 20 20 Hydralazine(?) induced lupus erythematosus DR4 73 32 DR3 B8 DR3 DR2 B7 B8 56 43 55 60 37 44 25 20 21 30 24 20 DR4 53 19 DR3 DR3 B8 DR3 B8 DR3 B8 DR3 DR7 B8 DR2 DR3 DR3 B8 B35 B27 DR4 72 49 40 70 46 70 50 79 60 68 88 81 82 75 70 79 95 24 22 21 20 23 20 22 22 15 22 29 20 20 22 15 9 20 Basedow-disease Active chronic hepatitis Sclerosis multiplex Myasthenia gravis Autoimmune IgA glomerulonephritis Type I diabetes Addison-disease (idiotopic, autoimmune) Sjörgen-syndrome Coeliaca Goodpasture-syndrome IgA loss Dermatitis herpetiformis De Qervain-thyreoiditis Reiter-syndrome Felty-syndrome ref: Klinikai immunológia (II. klinikum) (OHVI 1990 szerk.: Szegedi, Gergely, Sipka, Szemere) Stenszky Valéria: Autoimmun betegségek genetikai vonatkozásai Diseases Narcolepsia Bechterew-disease Adrenogenitális syndrome salt lost late virilizing Psoriasis vulgaris Idiophatic haemochromatosis Bechet-disease Gold induced thrombocytopenia Gold induced leucopenia HLA frequency concerned control DR2 B27 100 89 22 9 Bw47 B14 B5 Cw6 B13 B17 DR7 A3 B51 DR3 DR3 36 57 48 56 24 27 48 76 50 50 47 1 4 10 15 8 8 23 28 11 13 13 HLA allotypes and diseases HLA-A A*01010101A*0214 A*01010102N A*0215N A*010102 A*0216 A*010103 A*021701 A*010104 A*021702 A*0102 A*0218 A*0103 A*0219 A*0104N A*022001 A*0106 A*022002 A*0107 A*0221 A*0108 A*0222 A*0109 A*0224 A*0110 A*0225 A*0111N A*0226 A*0112 A*0227 A*0113 A*0228 A*0114 A*0229 A*0115N A*0230 A*0116N A*0231 A*0117 A*0232N A*0118N A*0233 A*0119 A*0234 A*0120 A*023501 A*02010101A*023502 A*02010102L A*0236 A*020102 A*0237 A*020103 A*0238 A*020104 A*0239 A*020105 A*0240 A*020106 A*0241 A*020107 A*0242 A*020108 A*0243N A*020109 A*0244 A*020110 A*0245 A*020111 A*0246 A*020112 A*0247 A*0202 A*0248 A*020301 A*0249 A*020302 A*0250 A*0204 A*0251 A*0205 A*0252 A*020601 A*0253N A*020602 A*0254 A*020603 A*0255 A*0207 A*0256 A*0208 A*0257 A*0209 A*0258 A*0210 A*0259 A*0211 A*0260 A*0212 A*0261 A*0263 A*0309 A*0264 A*0310 A*0265 A*0311N A*0266 A*0312 A*0267 A*0313 A*0268 A*0314 A*0269 A*0315 A*0270 A*0316 A*0271 A*0317 A*0272 A*0318 A*0273 A*0319 A*027401 A*0320 A*027402 A*0321N A*0275 A*0322 A*0276 A*0323 A*0277 A*0324 A*0278 A*0325 A*0279 A*110101 A*0280 A*110102 A*0281 A*110103 A*0282N A*110104 A*0283N A*110105 A*0284 A*110201 A*0285 A*110202 A*0286 A*1103 A*0287 A*1104 A*0288N A*1105 A*0289 A*1106 A*0290 A*1107 A*0291 A*1108 A*0292 A*1109 A*0293 A*1110 A*0294N A*1111 A*0295 A*1112 A*0296 A*1113 A*0297 A*1114 A*0299 A*1115 A*03010101A*1116 A*03010102N A*1117 A*03010103A*1118 A*030102 A*1119 A*030103 A*1120 A*030104 A*1121N A*030105 A*1122 A*0302 A*1123 A*0303N A*1124 A*0304 A*1125 A*0305 A*1126 A*0306 A*1127 A*0307 A*1128 A*2301 A*2428 A*2302 A*2429 A*2303 A*2430 A*2304 A*2431 A*2305 A*2432 A*2306 A*2433 A*2307N A*2434 A*2308N A*2435 A*2309 A*2436N A*2310 A*2437 A*2311N A*2438 A*2312 A*2439 A*2313 A*2440N A*2314 A*2441 A*24020101A*2442 A*24020102L A*2443 A*240202 A*2444 A*240203 A*2445N A*240204 A*2446 A*240205 A*2447 A*240206 A*2448N A*240207 A*2449 A*240208 A*2450 A*240209 A*2451 A*240210 A*2452 A*240211 A*2453 A*240212 A*2454 A*240301 A*2455 A*240302 A*2456 A*2404 A*2457 A*2405 A*2458 A*2406 A*2459 A*2407 A*2460N A*2408 A*2461 A*2409N A*2462 A*2410 A*2463 A*2411N A*2464 A*2413 A*2465 A*2414 A*2466 A*2415 A*250101 A*2417 A*250102 A*2418 A*2502 A*2419 A*2503 A*2420 A*2504 A*2421 A*2505 A*2422 A*2506 A*2423 A*260101 A*2424 A*260102 A*2425 A*260103 A*2426 A*260104 A*2603 A*300102 A*2604 A*300201 A*2605 A*300202 A*2606 A*300203 A*260701 A*3003 A*260702 A*3004 A*2608 A*3006 A*2609 A*3007 A*2610 A*3008 A*2611N A*3009 A*2612 A*3010 A*2613 A*3011 A*2614 A*3012 A*2615 A*3013 A*2616 A*3014L A*2617 A*3015 A*2618 A*3016 A*2619 A*3017 A*2620 A*3018 A*2621 A*310102 A*2622 A*3102 A*2623 A*3103 A*2624 A*3104 A*2625N A*3105 A*2626 A*3106 A*2627 A*3107 A*2628 A*3108 A*2629 A*3109 A*2630 A*3110 A*2631 A*3111 A*2632 A*3112 A*2633 A*3113 A*29010101A*3114N A*29010102N A*3201 A*290201 A*3202 A*290202 A*3203 A*290203 A*3204 A*2903 A*3205 A*2904 A*3206 A*2905 A*3207 A*2906 A*3208 A*2907 A*3209 A*2908N A*3210 A*2909 A*3211Q A*2910 A*3212 A*2911 A*3213 A*2912 A*3301 A*2913 A*330301 A*2914 A*330302 A*2915 A*3304 A*3306 A*6824 A*3307 A*6825 A*3308 A*6826 A*3401 A*6827 A*3402 A*6828 A*3403 A*6829 A*3404 A*6830 A*3405 A*6831 A*3406 A*6832 A*3407 A*6833 A*3408 A*6834 A*3601 A*6835 A*3602 A*6901 A*3603 A*7401 A*3604 A*7402 A*4301 A*7403 A*6601 A*7404 A*6602 A*7405 A*6603 A*7406 A*6604 A*7407 A*6605 A*7408 A*6606 A*7409 A*680101 A*7410 A*680102 A*7411 A*680103 A*7412N A*680104 A*8001 A*680105 A*9201 A*68020101A*9202 A*68020102A*9203 A*680301 A*9204 A*680302 A*6804 A*6805 A*6806 A*6807 A*6808 A*6809 A*6810 A*6811N A*6812 A*6813 A*6814 A*6815 A*6816 A*6817 A*6818N A*6819 A*6820 A*6821 A*6822 HLA-A alleles described until october 2006 http://www.ebi.ac.uk/imgt/hla/allele.html Type IV hypersensitivity reaction Chemokines, cytokines, cytotoxins Delayed-type Hypersensitivity (Type IV Hypersensitivity) Delayed-type Hypersensitivity (Type IV Hypersensitivity) Delayed-type hypersensitivity (DTH) (e.g., tuberculin skin test) TH1 from a previous immunization (memory) Tuberculin skin test Chemical Mediators of DTH Contact Dermatitis *a contact-sensitizing agent is usually a small molecule that penetrates the skin then binds to self-proteins, making them “look” foreign Poison ivy Anacardiaceae (family), Toxicodendron (genus) Toxicodendron radicans or Rhus toxicodendron Delayed-type hypersensitivity is mediated by T cells (Type IV hypersensitivity) Delayed-type Hypersensitivity A positive tuberculin skin test is a DTH reaction TYPE III HYPERSENSITIVITY Antibodies binding to soluble antigens Small circulating immune complexes Depends on: Size of immune complexes Antigen-antibody ratio Affinity of antibody Isotype of antibody THE PROCESS OF TISSUE DAMAGE CAUSED BY IMMUNE COMPLEXES Antigen C' Immune complex Antibody Complementa ctivation (C3a , C5a ) PMN Chemotaxis C' Endothelium Ba sophil Ba sa l membra ne gra nulocyte Vessel wa ll Thrombocytes Deposition Blood vessel wall permeability Frustrated phagocytosis Vasoactive a mines Immune complexes activate the complement system, neutrophils, bazophil granulocytes and thrombocytes MANIFESTATION OF TYPE III HYPERSENSITIVITY IN SLE Facial, malar "butterfly" rash with characteristic shape across the cheeks. Discoid lupus erythematosus (DLE) involves mainly the skin, it is relatively benign compared to systemic lupus erythematosus (SLE). In either case, sunlight exposure accentuates this erythematous rash. A small number (5 to 10%) of DLE patients go on to develop SLE (usually the DLE patients with a positive ANA). Here is a more severe inflammatory skin infiltrate in the upper dermis of a patient with SLE in which the basal layer is undergoing vacuolization and dissolution, and there is purpura with RBC's in the upper dermis (which are the reason for the rash). DEPOSITION OF IMMUNE COMPLEXES IN THE SKIN OF SLE PATIENTS When immunofluorescence staining with an antibody to complement or immunoglobulin is performed, a brightly fluorescent signal staining the dermal epidermal junction is visable indicating immune complex deposition. Immunofluorescence staining pattern with antibody to IgG staining immune complexes at the dermal-epidermal junction. If such a pattern is seen only in skin involved by a rash, then the diagnosis is probably DLE, but if this pattern appears even in skin uninvolved by a rash, then the diagnosis is SLE. RENAL FAILURE IN IMMUNECOMPLEX DISEASES One of the feared complications of the rheumatic diseases is renal failure. This is most likely to occur in SLE. Here is a glomerulus in which the capillary loops are markedly pink and thickened such that capillary lumens are hard to see. This is lupus nephritis. Here is a glomerulus with thickened pink capillary loops, the so-called "wire loops", in a patient with lupus nephritis. The surrounding renal tubules are unremarkable. ANA Anti -nuclear antibody This is the so-called "nucleolar pattern" of staining in which the bright fluorescence is seen within the nucleoli of the Hep2 cells. This pattern is more suggestive of progressive systemic sclerosis. This is the so-called "rim" pattern that is more characteristic of SLE. This is the so-called "speckled" pattern of staining which is more characteristic of the presence of autoantibodies to extractable nuclear antigens, particularly ribonucleoprotein. This pattern is not very specific, but may be seen with an entity called "mixed connective tissue disease" which is a mix between SLE, scleroderma, and polymyositis, but without serious renal or pulmonary disease. The autoimmune diseases are very hard to classify, even for the experts.