Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
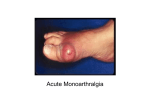
Case A 23-year-old woman with a one-week history of swelling and pain in her right third finger was seen by an orthopedist, who prescribed cephalexin and indomethacin for suspected tenosynovitis. Case She presented to the emergency department the day after pain developed in her right ankle with generalized malaise. PE showed a temperature of 39.4 C and a rash. What is your diagnosis? What is further management? Presented by Yaowapruek W. 18 Sep 2007 Introduction Neisseria gonorrhoeae infects human exclusively Colonize diverse mucosal surfaces -> local and disseminated infections Most frequently reported communicable disease in the US Most common cause of acute septic arthritis in young sexually active adults Contents Epidemiology Pathogenesis Clinical features Differential diagnosis Culture Treatment Annual incidence in US Epidemiology HIV epidemic -> reduction in number of cases Peak incidence in men occurred at ages 20 -24, women at ages 15 – 19 Disseminated gonococcal infection(DGI) occurs between 0.5% and 3% of cases of mucosal infection Pathogenesis Host Factors Local mucosal-microbial interaction Complement activation Cytokines Women (perimenstrual interval and pregnancy) Microbial Factors Pili Protein IA Protein II+ Protein III Iron-repressible membrane protein Lipo-oligosaccharide Proteoglycan IgA proteases Host factors Male : female ratio = 1:4 Gonorrhea in women often asymptomatic, -> delayed treatment -> bacteria spreading Pregnancy and perimenstrual interval Inherited complement deficiencies , esp C5-C8 def Surface of the Gonococcus Microbial Factors Mainly cell-surface structure Pili Major virulence factor! Pili protein subunits, pili-associated proteins Two variations : antigenic, phase -> help gonococci avoid host defense Microbial Factors Outer-membrane proteins Gonococci that lack of protein II in their outer membrane may have an impaired chemotactic response and are ass with DGI. Protein IA and AHU (arginine, hypoxantgine, uracil) strains more likely to disseminate Structure Pathogenic Role Pilus Adherence to mucosa Attachment to sperm Inhibition to phagocytosis Protein I “Spiking” host cells Protein II Adherence to certain mucosal cells Adherence to neutrophils Clumping of organisms Structure Pathogenic Role Protein III Binding site of blocking Ab Lipopolysaccharide Serum resistance Toxic to ciliated fallopiantube cells (marked endotoxic activity) Peptidoglycan Toxic to ciliated fallopiantube cells Pathogenesis Immune – mediated theory Aseptic inflammatory response Clinical Features Classic clinical triad in DGI Dermatitis DGI Tenosynovitis Migratory polyarthritis Clinical Features 2 clinical pictures Bacteremic infections (arthritis-dermatitis syndrome) ~ 60% Localized septic arthritis ~ 40% GU, Rectal, Pharynx Bacteremic stage Suppurative arthritis Patterns of arthritis Migratory polyarthralgia Tenosynovitis Purulent arthritis Monoarthritis Polyarthritis 70% 67% 42 % 32 % 10 % Diagnostic clue = Tenosynovitis ! and pain often out of proportion with clinical sign ( typically at hands and fingers) Clinical Features Joint involvement usu asymmetric, involves knee, elbow, wrist, MCP, ankle. HIV -> unusual joint (hip, sternoclavicular), aggressive course Synovial – WBC ~ 50,000 -200,000 and PMN > 90% Dermatitis 2/3 of cases Painless, nonpruritic skin rash ->usu. MP, pustular, necrotic, or vesicular on an erythematous base. Infrequently -> hemorrhagic skin lesions, EN, urticaria, EM Occurs below the neck (body, limbs, palms & soles) spare scalp, face and mouth Dermatitis Typically resolve over 4 to 5 days without residual scarring Rare manifestations • Pericarditis, endocarditis esp aortic valve, perihepatitis, pyomyositis, osteomyelitis, meningitis Differential diagnosis Nongonococcal septic arthritis Reiter’s syndrome Rheumatic fever Syphilis Hepatitis and bacterial endocarditis Lab tests Mild leukocytosis Elevated ESR Mild anemia and abnormal LFT’s Gram stain Culture Positive C/S ->confirms the diagnosis and allows determination of drug susceptibility Proven DGI = C/S from blood, synovial, skin , other sterile sources Probable DGI = C/S from primary mucosal sites Possible DGI = Typical clinical syndrome and response to Rx without positive culture Culture Site Genitourinary Synovial fluid Rectum Pharynx Blood Skin Isolation rate (%) 80 25-50 20 10 5-10 Rare Culture Joint fluid and other sterile sites -> Chocolate agar GU, rectum, pharynx -> Thayer-Martin media Warmed c/s plate and plate specimens bedside immediately Treatment Hospitalization is recommended if the diagnosis is unclear, frank suppurative arthritis, or poor compliance. Pts should be examined for clinical evidence of endocarditis and meningitis Ceftriaxone 1 g iv OD is the mainstay (Cefotaxime or ceftizoxime 1 g iv q 8 ) Treatment Switched to a oral FQ after clinical improvements for 24-48 hrs (Ciprofloxacin, Levofloxacin) Treatment duration = 1 week Treat Chlamydia co-infection -> doxycycline(100) 1*2 ~1 wk or single oral dose of azithromycin (1g) Treatment Closed drainage of purulent effusions NSAIDs for alleviate pain and prevent recurrent joint effusions Open drainage in difficult joints (i.e.hip) >1 episode of DGI -> work up for complement deficiency! Contents Epidemiology Pathogenesis Clinical features Differential diagnosis Culture Treatment Case A complete blood count showed a leukocyte count of 31,000 cells per cubic millimeter. The patient reported having had unprotected sexual intercourse during the previous three weeks. Case A cervical culture was positive for Neisseria gonorrhoeae The patient’s symptoms and rash resolved within three days after treatment with intravenous ceftriaxone.