Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
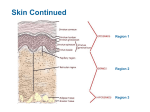
2015 Week5/2 NURS1004 The Integument Parts I & II Martini et al. 10th ed. Ch5 & p.539-542 Martini 9th ed Ch5 & p498-501. OR International ed. Ch 5 & p.561-563 The skin, hair, nails, glands and several specialised receptors make up the integumentary system. Functions of the skin: 1. Body temperature regulation 2. Protection (against abrasion, water loss, bacteria, UVRadiation) 3. Perception of stimuli 4. Excretion 5. Synthesis of vitamin D (calcitriol) 6. Immunity 7. (social function !) Structure of the skin About 7% of body weight, from 1.5 to 4.0 mm thick. Epidermis (outer layer) composed of epithelial cells, and a dead layer. Dermis (inner layer) composed of fibrous connective tissue and exocrine glands [Hypodermis (or superficial fascia) composed of adipose (& some areolar connective) tissue. Not part of skin, stores fat, anchors skin to muscle, allows skin to slide over muscle] 1. Epidermal cells (4 distinct types) 1. Keratinocytes. Tightly connected to each other (by desmosomes), produce keratin (a fibrous protein). 2. Melanocytes. Have numerous branching processes that touch all keratinocytes in the basal layer. Produce melanin, (a pigment which protects against UV) that is transferred to nearby keratinocytes. 3. Dendrocytes (langerhans’ cells & granstein cells). Interact with lymphocytes (T cells) to assist in the immune response. Are macrophages. 4. Merkel cells. Associated with a sensory nerve ending (called Merkel disc) for fine touch & pressure. Epidermis is NOT VASCULARISED ! Nutrients reach epidermal cells by diffusion Strata (layers) of the epidermis 1. Stratum germinativum/basale. Deepest layer, attached to dermis, single cell thick, youngest rapidly dividing keratinocytes. New cells push up the older ones above. 10%-25% are melanocytes. Form epidermal ridges. 2. Stratum spinosum. 7 to 10 cells thick. Cells contain keratin filaments that span cells, attach to desmosomes & so hold cells together. Blisters (from repeated rubbing) are fluid-filled pockets in stratum spinosum caused by disruption of junctions between cells – layers of skin separate. 3. Stratum granulosum. 3 to 5 cells thick. Contain granules which aggregate keratin & contain waterproofing glycolipid*. Cells flatten, nuclei & organelles disintegrate. (*glycolipids are lipids that contain carbohydrates, usually simple sugars like glucose) 4. [Stratum lucidum. (only present in thick skin – palms, soles) a few rows of clear, dead, flattened keratinocytes.] 5. Stratum corneum. Most superficial layer, 15 to 30 cells thick - up to ¾ of thickness of epidermis. Dead, flat, filled with keratin. Protects body against heat, light, chemicals, bacteria, abrasion. Cholesterol & Glycolipid between cells waterproofs this layer. – burns victims lose much water because skin is lost. 2. Dermis Contains hair follicles, oil & sweat glands, nerve fibres, blood and lymph vessels. Strong flexible connective tissue containing collagen, elastin and reticular fibres. (Dermis of animals can be tanned to make leather.) Reticular dermal layer (deep) 80% of thickness of dermis. Contain Pacinian corpuscles sensitive to deep pressure. Interlacing collagen fibres arranged in parallel bundles, (lines of cleavage) give skin strength & resilience. Elastin fibres provide the stretch/recoil properties of skin. Flexure lines (at joints). Mammary glands, specialized sweat gland that secrete milk. Papillary dermal layer (superficial) Contain folds and ridges called papillae that push up into epidermal layer - fingerprints Papillae contain capillary loop or light touch receptors – Meissner’s corpuscles. When capillaries dilated, blood comes close to skin surface, so energy may be radiated from body. Sensory receptors in skin Glands of the dermis Sebaceous (oil) glands found all over body (except palms & soles). Secrete sebum into a hair follicle, keeps skin & hair from drying out. Contains triglycerides, cholesterol, proteins, electrolytes & cell fragments. Sebum is bactericidal. Blocked ducts – whiteheads, blackheads Sudiferous (sweat) glands Eccrine (merocrine) sweat glands, coiled tube in dermis discharging through duct to pore on skin. Sweat is hypotonic filtrate of blood. It contains 99% water, Na+Cl-, vit.C, antibodies, urea, uric acid, ammonia, lactic acid, K+ (pH = 4-6.8). Under control of sympathetic division of autonomic NS. Sweat makes it difficult for non-normal flora to adhere to skin. Contains dermicidin – an antibiotic. Evaporation of water molecules (sweat) requires energy which is drawn from the skin – this leaves the skin cooler. Body needs to be hydrated to produce sweat (otherwise heatstroke). Apocrine sweat glands in axillary, nipple and anogenital areas. Function after puberty. Ducts empty sweat + fatty substances & proteins into hair follicles. Ceruminous glands in ear canal secrete cerumin (ear wax). Tactile receptors Merkel discs: detect fine touch Meissner’s corpuscles: for fine touch Pacinian (lamellated) corpuscles: for deep pressure Ruffini corpuscles: for pressure and distortion in skin Root hair plexus: to detect movement/distortion of hair follicle Free nerve endings between epidermal cells (with small receptive fields) for touch & pressure Thermoreceptors Heat free nerve endings: detect heat Cold free nerve endings: detect cold Nociceptors for pain: free nerve endings with large receptive fields (3 types: extremes of temp, mechanical damage, dissolved chemicals – strong stimuli excite all 3 ! “burning sensation” excited by many stimuli) About 100 sweat glands, 15 oil glands, 230 sensory receptors per cm2 of skin. Hair, consists of keratinised cells, protective function. Arrector pilli muscle stands hair up when cold (goosebumps). Nails, modified epidermis consisting of keratin, useful for scratching, picking things up. Rich bed of capillaries underlie nails (in dermis). Burns 1st degree: only epidermis is damaged (sunburn). Heals in 2-3 days 2nd degree: injures epidermis & upper dermis, blisters appear (partial thickness burns). Skin regenerates (1-2 wks) with little or no scarring. 3rd degree: full thickness burns, involve whole thickness of skin. Nerve endings destroyed. Extensive burns cannot heal themselves. Skin grafting required to avoid fluid loss & infection. If > 10% of skin area is burnt, critical. If > 20% of skin area burnt, life threatening. Ageing of skin Newborn skin is thin. During infancy & childhood skin thickens & subcutaneous fat deposited. During adolescence skin & hair become oilier, acne may appear. After 30 years skin begins to show effects of “environmental assault”. With old age rate of epidermal cell replacement slows, skin thins, glands secrete less. Elastin fibres clump, degenerate, collagen fibres become fewer & stiffer, hypodermal fat layer diminishes wrinkling. Number of active hair follicles diminishes hair thinning. Drug administration Topical: patted or wiped onto skin, absorbed through skin & act locally (eg corticosteroids) Transdermal absorbed through skin, acts systemically (eg nicotine patch, HRT, nitroglycerine) Intradermal: injections of < 1 cm3 into dermis. (eg allergy testing, tuberculin testing) Subcutaneous: (up to 2ml) injected into subcutaneous fat (hypodermis) layer (eg heparin, insulin) Lipid-soluble substances (eg steroids) can penetrate skin because glycolipids between cells of stratum corneum present no barrier. Vitamin D = calcitriol – required for uptake of Ca++ from gut In Skin: UV radiation causes “modified cholesterol molecules” (=provitamin D3) to be converted to “vitamin D precursor”. In Liver: enzymes modify this precursor (add a hydroxyl group) In Kidneys: “modified precursor” used to produce (add a 2nd hydroxyl group) and release calcitriol (vit D3) upon being signalled by PTH (hormone). Vit D3 is actually a hormone & skin an endocrine organ. M.Caon, 2013 Didy Button 2014 (Additional info) Human beta defensin 2 is a natural antimicrobial peptide produced by keratinocytes when injured. Part of skin’s natural defense mechanism (against atopic dermatitis, psoriasis). Actinic keratoses (solar keratoses = sun spots) reported in 40% of Australian pop! Can progress to squamous cell carcinoma. Treatment = cryotherapy with liquid nitrogen or CO2 slush, surgical removal, or topical therapy with fluorouracil cream. Non-melanoma skin cancer is the most common type of skin cancer. This type of skin cancer is more common in men, with almost double the incidence compared to women. Over 434,000 people are treated for one or more non-melanoma skin cancers in Australia each year. In 2011, 543 people died from non-melanoma skin cancers. 1. Superficial basal cell carcinoma 2. Nodular basal cell carcinoma surgically removed with scarring 3. Squamous cell carcinoma Sunburn causes 95% of melanomas, the most deadly form of skin cancer. In 2009, more than 11,500 people in Australia were diagnosed with melanoma and in 2011, 1,544 people died due to melanoma. The five-year relative survival rate for melanoma is 90% for Australian men and 94% for Australian women. More than 2000 Australians died from skin cancer in 2011. Majority cured by surgery. Patients with stage IV disease have poorer prognosis with 46% not surviving longer than 12months from diagnosis http://www.cancer.org.au/about-cancer/types-ofcancer/skin-cancer.html#jump_5 accessed 11/1/14.