Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
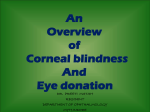
Head and Eyes Dr. Megan Gonzales ND, EAMP SIOM Western Clinical Sciences Fall 2012 External Eye Anatomy Internal Eye Anatomy Eyelid and Lacrimal Ducts Blepharitis Exopthalmos Ptosis Orbital Cellulitis Dacrocystitis Chalazion Stye Blepharitis Blepharitis is from an overgrowth of bacteria and may be linked to repeated styes and chalazia. You are more likely to develop this condition if you have seborrheic dermatitis of the face or scalp, rosacea, lice, and allergies. Exophthalmos Exophthalmos Exophthalmos (also called exophthalmia or proptosis) is a bulging of the eye anteriorly out of the orbit. Exophthalmos can be either bilateral (as is often seen in Graves' disease) or unilateral (as is often seen in an orbital tumor). other causes - infection, parasitic cysts, pseudoexophthalmos related to paralysis of the extraocular muscles Signs and symptoms: bulging eyeballs, with diplopia, extraocular muscle edema causes malallignment of the eyes. Other symptoms are related to systemic cause of exophthalmos (hyperthyroidism, tumor, cavernous sinus thrombosis) Diagnosis: usually based on obvious sign of bulging eyes, CT or MRI, culture of any discharge, Bx of orbital tissue Treatment: depends on underlying cause of dysfunction. Cold compress for trauma, treatment with antimicrobials, surgery, partial or total thyroidectomy Ptosis Ptosis PTOSIS: is also called "drooping eyelid." It is caused by weakness of the muscle responsible for raising the eyelid, damage to the nerves that control those muscles, or looseness of the skin of the upper eyelids. can be congenital either genetic or through a trait where the levator palpebrae muscles fail to fully develop aquired: advanced age - from cataract surgery, eyelid edema or other mechanisms leading to a heavy eyelid muscular dystrophy or myasthenia gravis where muscles are malfunctional paralysis nutritional factors such as thiamine deficiency in chronic alcoholism and other states of malnutrition can lead to lazy eye in children diagnosis is based on physical exam and finding the underlying condition causing ptosis may not require treatment but will be surgically correct if it interferes with vision. Can also be prescribed special glasses that contain and eyelid “crutch” Orbital Cellulitis Orbital Cellulitis Orbital cellulitis is an acute infection of the tissues immediately surrounding the eye, including the eyelids, eyebrow, and cheek. related to any type of infection from direct inoculation via the blood stream or near-by structures eg. sinuses. Also surgery, insect or animal bites, and foreign body trauma can cause cavernous sinus thromosis, hearing loss, septicemia, meningitis, optic nerve damage usually unilateral eyelid edema, reddened eyelids, hyperemic orbital tissue, extreme orbital pain, impaired eye movement, purulent discharge. Associated: fever, chills, malaise according to the cause of cellulitis. Diagnosis is based on clinical picture, CT and MRI of sinuses and brain, culture and sensitivity of discharge or wounds. Treatment: antimicrobials both systemic and topical, moist compresses, bed rest and fluids, I & D if abscess is present Dacrocystitis Dacryocystitis is an infection of the nasolacrimal sac, frequently caused by nasolacrimal duct obstruction. The term derives from the Greek dákryon (tear),[1] cyst (sac), and -itis (inflammation). It causes pain, redness, and swelling over the inner aspect of the lower eyelid. It is most commonly caused by Staphylococcus aureus and Streptococcus pneumoniae. The most common complication is corneal ulceration, frequently in association with S. pneumoniae. can lead to orbital cellulitis it is extremely painful and presents with constant tearing, there can be a sensation of pain or pressure over the nasolacrimal sac and applied pressure may or may not cause discharge from the punctum clinical picture, CBC and culture and sensitivity of any discharge is used to determine type of infection, in infants if it is due to duct atresia and x-ray after radiopaque injection shows the location treatment: warm compresses with topical and systemic antimicrobials, surgery can also be performed. Chalazion A chalazion (a more intense stye) is a small lump in the eyelid caused by obstruction of an oil producing or meibomian gland. Chalazia may occur in the upper or lower lids, causing redness, swelling and soreness in some cases. can lead to astigmatism diagnosis: visual exam and palpation of the eyelid. A Bx should be performed if the chalazion is persistent or recurring to rule out meibomian cancer. Treatment: warm compresses for 10-15 minutes up to 4 times a day. Incision and curettage may be necessary. After surgery antibiotic topicals may be prescribed but otherwise are not useful. Stye Hordeolum AKA Stye Stye (hordeolum) A stye is caused by bacteria from the skin that get into the oil glands in the eyelids that provide lubrication to the tear film. Styes are similar to common acne pimples that occur elsewhere on the skin. You may have more than one stye at the same time. Styes usually develop over a few days and may drain and heal on their own. A stye can become a chalazion -- this is when an inflamed oil gland becomes fully blocked. If a chalazion gets large enough, it can cause trouble with your vision. Conjunctival Disorders inclusion conjunctivitis conjunctivitis trachoma Inclusion Conjunctivitis Inclusion Conjunctivitis caused by Chlamydia trachomatis an obligate intracellular organism, can be a cause of “ophthalmia neonatorum” due to infection while passing through the birth canal. usually occurs in adults 18-30 years of age can cause otitis media and blindness. in neonates the first signs are reddened eyelids and slight discharge. A psuedomembrane can form which causes conjunctival scarring. In adults follicles appear inside the lower eyelids. It can persist for weeks or months with superficial corneal involvement. Inclusion Conjunctivitis Diagnosis is based on clinical features and history of sexual behavior including contact with an infected individual, a conjunctival scraping will be performed to check for the specific organism. A systemic anti-microbial is prescribed generally erythromycin and neonates are treated with anti-microbial ointment to the eyelids at 1 hour post birth. Conjunctivitis Conjunctivitis, commonly known as pink eye, is an infection of the conjunctiva (the outer-most layer of the eye that covers the sclera). The three most common types of conjunctivitis are: viral, allergic, and bacterial. Each requires different treatments. With the exception of the allergic type, conjunctivitis is typically contagious and self-limiting. Common bacterial causes: Staph aureus, Neisseria gonorrhoeae Common viral causes: adenoviruses, herpes simplex type 1 complications include: corneal infiltrates, reinfection and eye loss hyperemia of the conjunctiva with tearing and sometimes discharge, pain and photophobia. It often begins in one eye but spreads quickly to the other. Acute bacterial conjunctivitis lasts about 2 weeks, viral conjunctivitis has little to no exudate and can produce a severe disabling disease or be 2-3 weeks in course. Diagnosis -symptoms, stained conjunctival scrapings revealing lymphocytes due to viruses, neutrophils with a bacterial infection and eosinophils when allergens are the culprit. Treatment: application of broad-spectrum anti-biotics, prevention of a secondary infection with viral infections. The most important thing is to prevent spread of the disease. As Neisseria gonorrhoeae can be an infective agent diagnosis is important and the health care provider must report the infection! Trachoma Trachoma the most common cause of preventable blindness in less developed nations a form of chronic keratoconjunctivitis, may have a systemic symptomatic picture it is self limiting but permanently damages the cornea and conjunctiva due to scarring, the resulting secondary infections can cause blindness it is therefore important to diagnose and treat the condition early this is a result of an infection from Chlamydia trachomatis gram negative obligate intracellular bacterium. Transmitted eye-to-eye by flies and gnats or hand-to-eye contact. it is prevalent in Africa, Latin America and Asia primarily in children. Can lead to conjunctival scarring and corneal scarring, eyelid deformities and loss of vision it begins with a mild-looking bacterial conjunctivitis. After 1 month untreated the conjunctival follicles become enlarged and yellow and gray. At this time small blood vessels invade the cornea and upper lid. Contracture of the eyelid leads to entropion (the eyelids turn in and eyelashes scratch the cornea) Diagnosis is made based on symptoms and signs confirmed with a special stain detecting chlamydia Treatment requires topical and systemic antibiotic medications with erythromycin, doxycycline or sulfonamides and surgery for the entropion. Entropion Corneal Disorders Keratitis Corneal Abrasion Corneal ulcer Keratitis Keratitis inflammation of the cornea it may result from bacterial, fungal or viral infections and can lead to blindness commonly caused by the herpes simplex virus type 1. Bacterial infections can result due to infection of a corneal abrasion. can cause blindness and corneal scarring and perforation it is usually unilateral, presenting with decreased vision and discomfort to acute pain and tearing with photophobia. the corneal light reflexes may be distorted when examined with a penlight. it is diagnosed by patient history - a recent URI with cold sores and eye irritation after wearing contacts. Treatment - if due to herpes antiviral drops , ointment or oral acyclovir is prescribed. Bacterial infections require antibacterial drops given every half hour for the first 48 hours. Corneal Abrasion Corneal Abrasions a scratch on the epithelium of the cornea, usually due to foreign body under the eyelid. They happen in people who don’t wear protective eye coverings in high risk fields or when people fall asleep with contacts in. Can also be due to accidental dust, dirt or grit. The most common cause of ophthalmologic EMERGENT hospital visits in the US. Can cause corneal erosion, ulceration or permanent vision loss causes erythema, increased tearing, discomfort on blinking, feeling of “something in the eye”, pain disproportionate to the size of injury secondary to high innervation from the trigeminal nerve. Diagnosis is made based on history of eye trauma or prolonged use of contacts and symptoms of an abrasion. An ophthamologist will use a stain and special light to discern scratches. Treatment: topical anesthetics, removal of foreign body, antibiotic eye drops, a pressure patch to relieve pain on blinking, discontinued use of contacts while healing. Corneal Ulcer Corneal Ulcers a major cause of blindness worldwide. They produce scarring or perforation. Ulcers may occur anywhere but are most commonly found marginally. They require treatment within hours to prevent visual impairment. Usually due to a variety of infective agents. Commonly: Staph aureus, Pseudomonas aeruginosa, Herpes simplex type 1, varicella-zoster, Candida and Cephalosporium (bacterial, viral and fungal). Can cause corneal scarring, loss of the eye, loss of vision begins with pain that is worse on blinking, photophobia and increased tearing. Eventually a central ulceration will cause blurred vision. The eye may be injected and purulent discharge may be present. Diagnosis is based on history of trauma or over use of contact lenses. Use of a dye to show the ulcer confirms diagnosis. Treatment: PROMPT is NECESSARY TO SAVE VISION. Broad spectrum antimicrobial drops are used. If due to bacterial infection a patch SHOULD NOT be used because it generates an even better growth environment. Analgesics and observation for possible development of secondary glaucoma. Uveal tract, Retinal, Lens Disorders uveitis retinal detachment vascular retinopathies age-related macular degeneraton cataract retinitis pigmentosa Uveitis Uveitis is swelling and irritation of the uvea, the middle layer of the eye. The uvea provides most of the blood supply to the retina. Uveal Tract Uveitis usually idiopathic but can be the result of allergies, bacteria, viruses, fungi, chemicals, trauma and even surgery. can cause cataracts, glaucoma, retinal detachment, blindness moderate to severe unilateral eye pain, severe injection, tearing, small pupil non-reactive to light, blurred vision and sometimes produces deposits left on the back of the cornea. Onset is acute or insidious. Diagnosis is made with slit lamp examination. Treatment: is vigorous and prompt. One must ascertain the cause. For severe cases oral corticosteroids are prescribed. Retinal Detachment A retinal detachment occurs when the retina’s sensory and pigment layers separate. Because it can cause devastating damage to the vision if left untreated, retinal detachment is considered an ocular emergency that requires immediate medical attention and surgery. It is a problem that occurs most frequently in middle-aged and elderly populations. predisposing factors include myopia, intraocular surgery, trauma. Spontaneous retinal holes may develop as a normal part of aging. Rare in children. can lead to severe vision impairment, blindness initially there may be floating spots in the vision or recurrent flashes of light. It is a painless and gradual progression that can be described as a veil or curtain obscuring part of the visual field. An ophthalmologist will diagnose it will need to be surgically repaired. Vascular Retinopathy result from interference of eye blood supply often related to chronic medical conditions. There are 5 types: central retinal artery occlusion, central retinal veinous occlusion, diabetic retinopathy, hypertensive retinopathy, diabetic retinopathy, sickle-cell retinopathy. the diminished blood supply causes visual deficiencies. the cause can be idiopathic. More frequently it is due to atherosclerosis, embolism, carotid occlusion, temporal arteritis, heart failure, infection, hypercoagulation problems like sickle cell disease. can lead to blindness and secondary glaucoma central retinal artery occlusion causes sudden painless unilateral blindness. It typically causes permanent blindness. Central retinal venous occlusion is painless and results in partial loss of visual acuity - one can still see movement and light. Most patients develop secondary glaucoma shortly after onset. diabetic retinopathy can cause hemorrhages, microaneurysms and leakage of fluid into the macular area causing decreased visual acuity - reading and driving, night vision proliferative diabetic neuropathy shows neovascularization in the fundus. The new vessels are fragile and rupture causing sudden loss of vision. Scar tissue can form which pulls the retina and can lead to retinal detachment. hypertensive retinopathy - blurred vision and headache. Vascular changes reflect high blood pressure - like tortuous veins and swelling of the head of the optic nerve. Eventual leads to visual defects and blindness. Sickle cell retinopathy - shows peripheral arteriolar occlusions with anastomoses, neovascularization, hemorrhage and leads to retinal detachment. diagnosis is made with a visual acuity exam and vital sign check. An ophthalmologist will examine the fundus (posterior eye) for obvious changes. therapies directed at correcting the underlying condition and controlling the intraocular pressure are used to treat, surgery to decrease neovascularization may be used Age Related Macular Degeneration Age-related macular degeneration (ARMD) is a degenerative condition of the macula (the central retina). It is the most common cause of vision loss in the United States in those 50 or older, and its prevalence increases with age. AMD is caused by hardening of the arteries that nourish the retina. This deprives the sensitive retinal tissue of oxygen and nutrients that it needs to function and thrive. As a result, the central vision deteriorates. this is the most common cause of legal blindness in adults and a predominant cause of severe loss of central vision in the elderly. can cause blindness and nystagmus there is a change in central vision where straight lines become distorted and blank areas appear in the center of vision. Diagnosis is based on examination of the fundus after dilation Treatment: laser photocoagulation is used to reduce the possibility of severe vision loss if related to serous macular degeneration. Laser treatments can also be used with wet macular degeneration to destroy abnormal blood vessels. Cataract A cataract is a clouding of the natural lens, the part of the eye responsible for focusing light and producing clear, sharp images. The lens is contained in a sealed bag or capsule. As old cells die they become trapped within the capsule. Over time, the cells accumulate causing the lens to cloud, making images look blurred or fuzzy. For most people, cataracts are a natural result of aging. patients will generally experience painless blurring and obscuring of vision over time. The black pupil begins to appear hazy and there can be blinding glare from lights at night. Diagnosis: visual acuity is decreased though opacity is unnoticed until advanced stage. Treatment: surgical extraction of lens opacity with correction of visual deficits. Common complication is infection. Retinitis Pigmentosa Retinitis pigmentosa (RP) is a rare, hereditary disease that causes the rod photoreceptors in the retina to gradually degenerate. The rods are located in the periphery of the retina and are responsible for peripheral and night vision. Cones, another type of photoreceptor, are densely concentrated in the macula. The cones are responsible for central visual acuity and color vision. no cure is known for this rare hereditary condition but vitamins A and E might help slow progression. Other Random Disorders optic atrophy extraocular motor nerve palsies glaucoma Optic Atrophy Optic Atrophy can develop spontaneously or secondary to inflammation or edema of the optic nerve head, it may subside without treatment but, if the optic nerve degenerates it is irreversible. usually results from central nervous system disorders like tumors, syphilis, retinal vascular disease. Can also be related to chronic papilledema, central retinal artery or venous occlusion, exposure to methanol and quinine or vitamin B12, amino acid or zinc deficiency. can cause abrupt or gradual painless loss of vision or acuity of vision. an ophthalmologist will examine visual acuity and the fundus to diagnose. Treatment: corrects underlying cause to prevent irreversible changes. Extraocular Motor Nerve Palsies Extraocular muscles and movement including CN innervations Extraocular Motor Nerve Palsies dysfunctions of the III, IV and VI cranial nerves associated with trauma, diabetes and intracranial aneurysm most commonly due to trauma Signs and Symptoms: usually diplopia varying in different visual fields related to which nerve is involved. CT or MRI are used to rule out tumors and to help find the cause of palsy. Treatment: identification and appropriate cure for underlying cause Glaucoma Glaucoma Glaucoma is a disease caused by increased intraocular pressure (IOP) resulting either from a malformation or malfunction of the eye’s drainage structures. Left untreated, an elevated IOP causes irreversible damage the optic nerve and retinal fibers resulting in a progressive, permanent loss of vision. However, early detection and treatment can slow, or even halt the progression of the disease. Open Angle • Open angle (also called chronic open angle or primary open angle) is the most common type of glaucoma. With this type, even though the anterior structures of the eye appear normal, aqueous fluid builds within the anterior chamber, causing the IOP to become elevated. Left untreated, this may result in permanent damage of the optic nerve and retina. Eye drops are generally prescribed to lower the eye pressure. In some cases, surgery is performed if the IOP cannot be adequately controlled with medical therapy. Acute Angle Closure • Only about 10% of the population with glaucoma has this type. Acute angle closure occurs because of an abnormality of the structures in the front of the eye. In most of these cases, the space between the iris and cornea is more narrow than normal, leaving a smaller channel for the aqueous to pass through. If the flow of aqueous becomes completely blocked, the IOP rises sharply, causing a sudden angle closure attack. Acute angle-closure glaucoma is an ocular emergency to treat IOP with agents like pilocarpine to constrict the pupil and allow fluid to escape Refractive Disorders Myopia Nearsightedness or myopia, occurs when light entering the eye focuses in front of the retina instead of directly on it. This is caused by a cornea that is steeper, or an eye that is longer, than a normal eye. Nearsighted people typically see well up close, but have difficulty seeing far away. Hyperopia Farsightedness or hyperopic, occurs when light entering the eye focuses behind the retina, instead of directly on it. This is caused by a cornea that is flatter, or an eye that is shorter, than a normal eye. Farsighted people usually have trouble seeing up close, but may also have difficulty seeing far away as well. Astigmatism Astigmatism means that the cornea is oval like a football instead of spherical like a basketball. Most astigmatic corneas have two curves – a steeper curve and a flatter curve. This causes light to focus on more than one point in the eye, resulting in blurred vision at distance or near. Astigmatism often occurs along with nearsightedness or farsightedness