Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Oesophagostomum wikipedia , lookup
Hepatitis C wikipedia , lookup
Gastroenteritis wikipedia , lookup
Neonatal infection wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
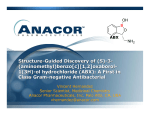
ENDOPHTHALMITIS By : SAAD AL-DAHMASH Endophthalmitis The term refers to intraocular inflammation predominantly involving the vitreous cavity and A/C, as a result of intraocular colonization by microrganisms. Pathophysiology In 29 – 43% of cataract surgery , intraocular contamination occurs with facultative bacteria from ocular surface without development of endophthalmitis . Immune privilege mechanisms are particularly effective in the anterior part of the eye. pathophysiology Ocular infection with infectious bacterial load /with impairment of immune privilege of the eye ,leads to intense destructive inflammatory reaction . ( Bact. Toxins ,proteases + intense host inflammatory response ---------- injury to retina ,CB, A/S structures . Intense inflammatory response ----- negative microbiological studies . Classification 1) Endogenous : bacterial / fungal / parasite. 2) Exogenous : a) postoperative. b) post traumatic . c) Bleb associated . d) miscellaneous ; e.g. microbial keratitis ,scleritis (infectious) Incidence *Post cataract 0.07 – 0.5 %. *post PKP 0.11%. *post PPV 0.05 %. *Bleb related 0.2 – 9.6 %. *traumatic 2.4 – 8.0 % , up to 40% in rural areas with IOFB. Signs and symptoms *Decrease VA. *pain. *A/C reaction +/- hypopyon. *Vitritis . *others: lid swelling , discharge , C.edema, chemosis. D.Dx *TASS. *Complicated , prolong surgery . *Preexisting uveitis . *Retained lens material. *Associated ocular injury . NB : presence of significant vitritis = infectious Endoph. Till proven otherwise . Microbial spectrum Post cataract :CNS 33-77% Staph. Aurus 10-21% Streptococci 9-19% G –ve, fungi 6-22% Delayed onset (chronic) post cataract: Prop. Acne ,corynebacteria,fungi. Post glaucoma Sx: CNS 67% early Strept, H influ. Cont. Post traumatic : CNS 16 – 44 % Bacillus 17 – 32% G -ve 10 -18% Strept. 8 – 21% Fungi 4 – 14 % Source of infection *Mainly eye lids and conjunctiva. *Other sources : e.g. - lacrimal drainage syst. Infections. - Blephritis. - infected socket in contralateral prosthetic eye. Risk factors for Endoph. Post cataract surgery *Disruption of the integrity of the barrier between A/S and P/S ( post. Caps.tear,zonular dialysis,vitreous loss). *clear corneal incision > scleral tunnel. *wound leakage in the first day post op. *Silicon IOL > PMMA. *no difference of incidence between sutureless and suture technique if no leak. *No diff. between inpatients and outpatients. *No diff. between DM and non DM. *No diff. between disposable and reusable instruments. Prophylaxis *Antiseptics: 5% povidone – iodine for at least 3 minutes is the most important prophylaxis in many studies; decreasing conj +periorbit.skin flora . *Single use instruments is always preferable esp. tubes. *there has been no randomised controlled studies of preoperative cutting of eye lashes, available data in the literature showed no association with the reduction of the risk of Endoph. *But taping back of the lashes with adhesive tape is recommended. * Treat any underlying predisposing cause e.g. blephritis. Antibiotics Topical antibiotics esp. 4th generation fluoroquinolones appears to be very effective in reducing conj. Flora load , achieving high concentrations in the in the A/C. But no controlled clinical trial prove their effect in reducing incidence of Endoph. Abx Systemic antibiotics preopertive or post op has not proven to be of benefit against post op Endoph. In penetrating ocular trauma systemic +/intravitreal Abx shown to have some protective effects ; two recent studies. Abx Adding antibiotics to irrigation solution , there was a debate about there use but there is no study based evidence showing reduction of Endoph. Also , risk of endoth. Toxicity not studied . Abx Injection of intracameral 1mg/0.1ml of cefuroxime (3000ug/ml @ a/c ) at the end of surgery: It has bee shown the risk of Endoph. with this regimen reduced by almost 5 folds (ESCRS ) study NB: cefuroxime resist. MRSA,MRSE,Ent.faecalis,pseud.aur. Abx Subconjunctival antibiotics: It is very common practice to inject Abx subconj. at conclusion of surgery. *Gentamycin is not effective against Strept. Species ,prop.acne. *Subconj.cefuroxime --- 20ug/ml in A/C much lower than intracameral. *till now no proven evidence of it’s help. Abx *post op Abx use : It is recommended to use post op Abx of same type used preop esp. quinolones for 1 - 2 weeks until the wound is secured ; but this also not proven to be effective but it is not harmful. NB they recommendation to start them in the first day very frequent (Q2hrs) for one day then QID to decrease A/C contamination load. Diagnosis *It is mainly clinical. *Delay in diagnosis is not uncommon (steroids ,complications ,expected post op inflam.). *B-scan is an aid , but some times it is misleading . *if doubt, be safe and consider it as Endoph., no body is blaming of over protection but missing serious irreversibly damaging pathology is this the situation. Management of acute post op Endophthalmitis *It is a real ophthalmic emergency. *controversies in management : Vitreous tap + A/C sampling + intravitreal Abx&steroids---- in cases VA >=HM (EVS) VS Primary Vitrectomy +intravitreal Abx&steroids in all cases (ESCRS). Mx ESCRS recommend Primary Vitrectomy +intravitreal Abx&steroids as a gold standard of care : To: dec. bact. Load , pus , remove most of the inflammatory destructing cells and mediators , removing the scaffold (vitreous) Mx EVS recommends : a) Vitreous tap + A/C sampling + intravitreal Abx&steroids---- in cases VA >=HM. b) Vitrectomy +intravitreal antibiotics &steroids in cases VA < HM. Why ? -Comparative results founded ( organism virulence). -Avoiding delay vitreous tap + Abx . -Avoiding vitr. Complications In a fragile retina . * Inravitreal antibiotics can be repeated every 48 hours according to the response Adjunctive measures According to EVS systemic Abx do not appear to have any effect on the course and the outcome of endophthaalmitis. But : they use ( amikacin + ceftazidime ) systemically ; and ( vancomycin +ceftazidime ) intravitrealy. They don’t use same Abx , they don’t take in consideration of G +ve to be the most common to be covered. So, at least in theory; IV Abx of same type of intravitreal Abx can contributes towards maintaining effective Abx level within the eye . Also , some practitioners will use topical fortified same Abx for same principle. Cont. Adjunctive measures *As mentioned earlier , the destructive agent in Endoph. Is the intense inflammatory response + the bacterial toxins . *Systemic (oral) steroids is recommended, studies does not shown any negative effect on the infection course in cases of bacterial endophthalmitis . *also , topical steroids has same principle. Chronic (delayed onset) post operative endophhalmitis It is very commonly misdiagnosed as uveitis or post op. inflammation . Problems: a)High rate of recurrence. b)Difficulty in culturing the organism(mostly prop. Acne) because it is enclosed in the synechised capsular bag. Dx &Mx *If clinical diagnosis suspected : 1st step: start systemic Clarithromycin 250mg po BD for 2/52 ( it is concentrated 200 X more in macrophages,PMN containing intracellular bacteria as prop.acne ) If improvement is successful keep close F/U 2nd step : If no improvement in step one, consider PPV + intravitreal Abx ( vancomycin +cefazoline ) + posterior capsulotomy . 3rd step: If no mprovements in step 2 remove IOL +surrounding bag . Outcomes of treatment *in general more virulent organisms as : staph aureus,strept, bacillus sp,pseud. Carry the worst visual outcomes. *low virulent organisms as ( CNS, P acne ) carry better visual outcomes . Out comes from EVS @ 3/12 --- 41% had >=20/40. 69% had >=20/100. @9 – 12/12 ---- 53% had >=20/40. 74% had >=20/100. 15% had < 5/200. @ final follow up visit 5% had NLP. Cont. Chronic endoph. Carries a favorable visual prognosis , one study showed final VA >=20/40 in 80% of cases . THANK YOU