Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
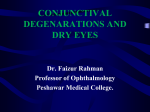
Department of Ophthalmology University of Siena, Italy PTERYGIUM PROGRESSION DETECTED BY IN VIVO CONFOCAL MICROSCOPY Martone Gianluca, Malandrini Alex, Balestrazzi Angelo, Tosi Gian Marco, Pichierri Patrizia , Caporossi Aldo No author has a financial or proprietary interest in any material or method mentioned Introduction Pterygium is a benign growth of the conjunctiva from the nasal side of the sclera towards the centre of the cornea. It is associated with, and thought to be caused by ultraviolet-light exposure. The pathogenesis is still debated (1). The histopathology is characterized by basophilic degenerative fibrovascular tissue invading the superficial cornea with destruction of the underlying Bowman’s membrane. IVCM is becoming a useful diagnostic tool for ocular surface imaging to describe limbus and corneal diseases (2). It can provide details of ocular structures at the cellular level . In some studies, IVCM was used to examine the typical structure of pterygium (3-4). Purpose To perform a qualitative assessment of anatomical and pathological changes in the cornea and conjunctiva of patients affected by pterygium and to describe the typical components of progressive and not-progressive pterygium by IVCM. Methods 40 eyes of 32 patients with primary pterygium was examined by slit lamp examination and IVCM in a prospective randomized double blind study. IVCM (Heidelberg Retina Tomograph II with the Rostock Cornea Module) analysis was performed in two different corneal areas, in the central and peripheral pterygium zone. The IVCM images (400 µm x 400 µm) were acquired from the periphery to central pterygium areas. During the examination, all subjects were asked to fixate external light target in order to good visualization of the pterygium. All eyes were evaluated at baseline, after 6 and 12 months. After 12 months they were classified in two groups: progressive and non-progressive group. Results: Progressive group Actvated keratocytes and stromal edema at body of pterygium Cloudy and hyperreflective margin of the apex head Irregular corneal epithelium adjacent to the pterygium head and not well defined transfer zone Many capillaries and an important infiltration of dendritic cells in pterygium head Hyperreflective formations as scars that could be Bowman’s membrane breaks Results: Not progressive group Reduction of stromal edema with low activated keratocytes and low inflammatory cells and vessels Many irregular hypereflective areas were also present between the head of pterygium and adjacent cornea (Fuchs' dots) Irregular epithelium morphology adjacent to the head of the pterygium but the margins are well defined Bright intracellular inclusions in the basal epithelial cell layer (Stoker’ s line) and the surrounding epithelium appears absolutely normal Discussion In this study, IVCM was used to examine the typical structure of primary pterygium. The body and the head of the pterygium and the corneal epithelium and stroma adjacent to the pterygium head were characterized by the presence of different findings between the progressive and not-progressive groups. Significant correlations were found between clinical progression of the pterygium and IVCM parameters. Furthermore, the findings obtained by IVCM suggest that it may be helpful as a non-invasive and uncomplicated method to study the anatomical structural corneal and conjunctival changes in patients with pterygium and understanding its condition of progression. Larger studies should be carried out to understand further the changes at the level of the cornea induced by the pterygium and correlate them with signs of clinical progression to plan the surgery. References 1. Hill JC & Maske R. Pathogenesis of pterygium. Eye 1989;3:218–226. 2. Cavanagh HD, Petroll WM, Alizadeh H et al. Clinical and diagnostic use of in vivo confocal microscopy in patients with corneal disease. Ophthalmology 1993;100:1444-54 3. Papadia M, Barabino S, Valente C, Rolando M. Anatomical and immunological changes of the cornea in patients with pterygium. Curr Eye Res 2008;33:429-34. 4. Gheck L, Dupas B, Denion E, Amar N, Baudouin C. Advantages of in vivo confocal microscopy for investigation of the pterygium. J Fr Ophtalmol 2007;30:703-10.