Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
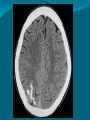
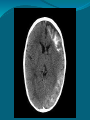
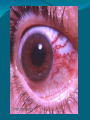
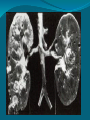
Neurocutaneous syndromes Dr. Ibrahim Khasraw Lecturer in Pediatrics School of Medicine University of Sulaimani They are group of syndromes characterized by involvement of the brain & skin. Because both originated from ectoderm embryologic ally. Types ; neurofibromatosis type1&2 tuberous sclerosis sturge webber syndrome ataxia telangectasia incontinentia pigmenti von hipple lindau disease Neurofibromatosis NF1&NF2 Incidence 1:3000 live birthes/prevalenc 1/50000 A.D 1/3 due to new mutation Abnormality due to chromosome 17& neurofibrin Criteria for diagnosis (NF1:Von-wrikling hausen dis.) : >=2 of these should be present 1. >=6 of cafe-au-lait spot>5 mm in size before puberty later on >15 mm. 2. >1 NF (nodular overgrowth of NF) 3. Axillary or inguinal freckles' . 4. Optic glioma which cause blurring of vision . 5. Iris –lesh nodule on slit lamp exam . 6. Bony lesion: sphenoid dysplasia lead to protrusion of eye ball . 7. 1st degree relative with NF1 . Other features: Skin lesion more common after puberty, may be mild or severe . NF may occur in peripheral N. &cranial N. Visual ,auditory involvement if the 2nd &8thcranialN. Megalencephaly, learning difficulty ,epilepsy may present. Pseudoarhrosis, scoliosis ,cardiac involvement may occur . NF2(central) Present with bilateral aquastic neuroma. More common in adolescents. Deafness & cerebro pontine angle syndrome(facial palsy +- cerebellar ataxia . Feature of both NF1 &NF2 may be mixed . Both may have endocrinal disorder(MEN). Phaeochromocytoma ,pulmonary hypertension, renal artery stenosis ,glioma of the brain & sarcoma . Rx: no radical treatment for both, apart from symptomatic Surg. For ,hydrocephalus and brain tumor. Drugs for Epilepsy to prevent farther attacks. Tuberous sclerosis (Epiloea) : A.D 70% newmutation . Prevalence 1:9000 live birth . Hamartoma in many organs :brain ,eye, skin,kidney ,heart . Abnormality in hamartin & tuberin in chr.16 . C/F(cutaneous) Ash-leaf patch (depigmented)better seen by woods light& U.V . Shagreen patch (roughened patch) in area of lumber spine . Adenoma sebaceum (angiofibroma) like butter fly on the bridge of nose & cheeks unusually before 5 years old . Neurological Infantile spasm + -developmental delay . Epilepsy: usually focal, salaam attack, myoclonus, atonic, grandmal. Intellectual impairment. Autistic feature. Brain glioma. Others : Subangual fibroma. Retinal phakoma. Cardiac tumor (Rabdomyoma,)in early weeks may disappears in infancy . Polycystic kidney ,renal angioglioma . Investigation CT scan show calcification, sub ependymal nodules & tubers in 2nd year of life . Woods light for ash leaf spot. DNA study. Sturge webber syndrom(SWS) 1:50000 Sporadic Presence of port- wine stain in area of trigeminal N. which must involve ophthalmic branch, uni or bilatera lly. There is underlying piamatar venous hemangioma Contra lateral hemi paresis . Calcification of gyri in form of rail-road track shape on skull X –ray, CT scan ,MRI 60 % . Epilepsy, M.R. ,hemiplagia,(contra lateral),intractable epilepsy. Glaucoma 30-50% hemianopia . Treatment Supportive for epilepsy ,glaucoma by drugs or surgery(hemi spherectomy) ,lesionectomy. Laser therapy for nevus flummus. Monitor intra ocular pressure. Thanks