Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
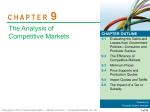
CXLUSA Clinical Trial Results S. Lance Forstot, MD, FACS Corneal Consultants of Colorado Founding Partner Clinical Professor of Ophthalmology University of Colorado School of Medicine ®Copyright Rubinfeld 2013 CXLUSA Clinical Trial Results Roy S. Rubinfeld, MA, MD Georgetown University Medical Center, Washington Hospital Center, Washington, DC Dr. Rubinfeld has intellectual property in corneal strengthening technology and financial interests in CXLO and CXLUSA ®Copyright Rubinfeld 2013 What’s What? o Non-commercial, physician-sponsored UV research studies approved by IRBs since 2009. No IP, no investors Limited number of centers o Commercial start up with IP, investors, BOD, Novel Technology, Commercial Drug, Advisors ®Copyright Rubinfeld 2013 CXLUSA Study Group Centers Rubinfeld: Rockville MD, Fairfax VA Miami FL : Center for Excellence in Eye Care Chicago IL: Chicago Cornea Consultants, Ltd Denver, CO: Corneal Consultants of Colorado Los Angeles CA: LA Sight West Hills, CA: Davidorf Eye Group San Diego, CA: Clear View Eye and Laser Center San Francisco, CA: Goodman Eye Center Orange County, CA: Harvard Eye Associates Boston, MA: Talamo Laser Eye Consultants ®Copyright Rubinfeld 2013 CXLUSA Study Group Centers St. Louis, MO: Ophth Assoc- Corneal & Laser Long Island, NY: South Shore Eye Care Scottsdale, AZ: Schwartz Laser Eye Center Dallas, TX: Cornea Associates of Texas Cleveland, OH: Clear Choice Custom LASIK Center Seattle, WA: Northwest Eye Surgeons Spokane, WA: Empire Eye Physicians Bloomington, MN: Minnesota Eye Consultants Atlanta, GA: Woolfson Eye Institute ®Copyright Rubinfeld 2013 CXLUSA Study Group Centers Arizona: Scottsdale California: Los Angeles Orange County San Diego San Francisco West Hills Colorado: Denver Florida: Miami Georgia: Atlanta Illinois: Chicago ®Copyright Rubinfeld 2013 CXLUSA Study Group Centers Maryland: Rockville Massachusetts: Boston Minnesota: Bloomington Missouri: St. Louis New York: Long Island Ohio: Cleveland Texas: Dallas Virginia: Fairfax Washington: Seattle Spokane ®Copyright Rubinfeld 2013 CXL Mythology ®Copyright Rubinfeld 2013 Epi-Off is Better Epi-On is Better Epithelium removal is needed to load the stroma with riboflavin See pictures Transepithelial Riboflavin Loading @12 min 15 Min Epi-On CXLO (~20 y/o pt) Cobalt Blue Light SL Pix ®Copyright Rubinfeld 2013 Epi-on Flare ®Copyright Rubinfeld 2013 Epi-Off is Better Epi-On is Better With Epi-On CXL, the riboflavin only loads epithelium which blocks the UVA and limits CXL See picture 15 Min Epi-On CXLO White Light SL Pix (18 y/o Pt) Epi-Off is Better Epi-On is Better Epithelium off CXL is safer than epi-on See pictures Haze after Epi-Off CXL ®Copyright Rubinfeld 2013 Delayed Epithelial Healing and Infiltrate after Epi-Off CXL Courtesy of W. Trattler, MD Postop Day 2 ®Copyright Rubinfeld 2013 Postop Day 5 ®Copyright Rubinfeld 2013 Perforation after Epi-Off CXL Epi-off Complications o Microbial keratitis after corneal collagen crosslinking. Perez-Santonja JCRS 2009;35(6):1138-40 o Pseudomonas keratitis after collagen crosslinking for keratoconus: case report and review of literature. Sharma. JCRS 2010;36(3):517-20 o Complication and failure rates after corneal crosslinking. Koller, Seiler, et. al. JCRS 2010;36(1):185 o Permanent corneal haze after riboflavin-UVA-induced cross-linking in keratoconus. Raiskup, Spoerl, JRS2009 Sep;25(9):S824-8. o Corneal melting in both eyes after simultaneous corneal cross-linking in a patient with keratoconus and Down syndrome. Ophthalmologe. 2010 Oct; 107(10):951-5 o Corneal melting corneal collagen cross-linking for keratoconus: A case report. Labiris. Journal of Medical Case Reports 5:15 2012 o Early ocular surface-related complications after CXL. Gutman. Modern Medicine Sept, 2012. ®Copyright Rubinfeld 2013 Critical Balance of 3 Reactants is Essential Oxygen UV light Riboflavin Clear Cornea- Epi-On CXL POD 1 ®Copyright Rubinfeld 2013 Epi-On Advantages Safety Treat thinner, steeper, younger corneas, Return to preop vision, function POD 1 Return to CLs in days 1 day of discomfort KCN as indication for PKP ®Copyright Rubinfeld 2013 But Epi-on is not “better” if it doesn’t work ®Copyright Rubinfeld 2013 Clinical Experience - Keratoconus Vision Improvement (>= 1 line of vision) CXLUSA vs. Hersh/Avedro N = 177 N = 48 N = 49 N = 177 c/o William Trattler, MD N = 48 N = 49 1 Year Results (Advanced KCN) Formulation 1 (36 eyes) UCVA: Improved ≥1 Lines: 56% Worsened: 3% No Change: 40% BSCVA: Improved 1 ≥ Lines: 41% Worsened: 32% No Change: 24% K Max: Avg Flattening vs. Pre Op= 1.55D Formulation 2 (31 eyes) UCVA: Improved ≥1 Lines: 64% Worsened: 8% No Change: 28% BSCVA: Improved 1≥ Lines: 56% Worsened: 8% No Change: 35% K Max: Avg Flattening vs. Pre Op= 1.41D Epi- On CXLUSA Results UCVA, BSCVA by ≥ 1 line ~50% Kmax by ~0.7 to 1.55 D Tx failures <1%, 0 Adverse Events Comparable to Epi-Off with reduced risk, discomfort, visual recovery time KCN as indication for PKP ®Copyright Rubinfeld 2013 Limitations of CXL Alone Stops Progression Mild improvement in ~50% Can we do better for advanced cases? ®Copyright Rubinfeld 2013 Limitations of CXL Alone Terrific for early KCN before vision is lost CXL stops progression of vision loss and corneal steepening For those who have lost vision from KCN or ectasia, CXL usually yields only mild improvement in vision and topo/tomos Can we do better for more adv cases? ®Copyright Rubinfeld 2013 What if we Could Do This Consistently With Two Non-invasive Procedures? ®Copyright Rubinfeld 2013 Observant keratoconus patients sometimes point out, “Pressing on my eye right here, my vision gets much sharper.” c/o Anita Nevyas Wallace, MD No Finger Pressure 20/200 Finger Pressure at 6 o’clock 20/40 Finger Pressure at 7 o’clock 20/30+ ®Copyright Rubinfeld 2013 CK Plus CXL Technique ®Copyright Rubinfeld 2013 Immediately Postop CK vs Preop ®Copyright Rubinfeld 2013 27 y/o F Caucasian w KCN @ 1 Mo VAsc PREOP: 20/80 VAsc 1 MO PO: 20/20Preop RFx: -2.00 +5.50 X 170 20/25 1 MO PO RFx: pl +0.75 X 150 20/25+ ®Copyright Rubinfeld 2013 27 y/o F Caucasian w KCN @ 6 Mo VAsc PREOP : 20/80 VAsc 6 MO PO : 20/25Preop RFx: -2.00+5.50 X 170 20/25 6 MO PO RFx: pl + 1.25 X 155 20/25 ®Copyright Rubinfeld 2013 CK + CXL Average UCVA OU 300 Average UCVA 250 Visual Acuity 200 # Eyes Treated Pre-Op = 99 1 month = 71 3 months = 52 6 months = 34 12 months = 3 150 100 50 0 Pre-Op 1 month 3 months Time 6 months 12 months ®Copyright Rubinfeld 2013 Best Corrected Visual Acuity CK + CXL BCSVA OU BCSVA OU 60 50 40 30 20 10 0 Avg Pre-Op Avg. 1 month Avg. 3 months Time Avg. 6 months Avg. 12 months ®Copyright Rubinfeld 2013 Ongoing Data Collection ®Copyright Rubinfeld 2013 There are known knowns; there are things we know that we know. There are known unknowns; that is to say there are things that, we now know we don't know. But there are also unknown unknowns – there are things we do not know, we don't know. 2/12/02 ®Copyright Rubinfeld 2013 “Known Known” Epi-On is safer, as effective and likely to supplant Epi-Off Known unknown: Epi-On CXL may “lock in” CK and become important procedure ®Copyright Rubinfeld 2013 Thank You ®Copyright Rubinfeld 2013