Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Video relay service wikipedia , lookup
Telecommunications relay service wikipedia , lookup
Hearing aid wikipedia , lookup
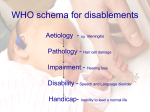
Hearing loss wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Sensorineural hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
Universal Newborn Hearing Screening What It Is and How It Happens Karl White, Ph.D. National Center for Hearing Assessment and Management Utah State University www.infanthearing.org Early Hearing Detection and Interveniton (EHDI) Programs Hospitals with Universal Newborn Hearing Screening Programs 4000 Number of Hospitals 3500 3000 2500 2000 1500 1000 500 0 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 Year Percentage of Newborns Screened for Hearing Prior to Hosptial Discharge 100.0% 90.0% 80.0% 100.0% 70.0% 90.0% 60.0% 80.0% 70.0% 50.0% 60.0% 40.0% 50.0% 30.0% 40.0% 30.0% 20.0% 20.0% 10.0% 10.0% Jan-02 Jan-01 Jan-00 Jan-99 Jan-98 Jan-97 Jan-96 Jan-95 Jan-94 Jan-93 0.0% Percentage of Newborns Screened for Hearing in the United States (Dec 2001) . Percentage of Births Screened 90%+ 51 - 90% 21 - 50% 1 - 20% 3 States with Legislative Mandates Related to Universal Newborn Hearing Screening Status of UNHS Legislative Mandates States with mandates No mandate, but statewide programs No mandate National Universal Newborn Hearing Screening Programs • • • • • • Austria United Kingdom Poland Flemish Belgium Singapore Canada (Ontario) Why is Implementation of Newborn Hearing Screening Accelerating? Improved Screening Techniques/Equipment Acceptance By Policy Makers • National Institutes of Health • American Academy of Pediatrics • Maternal and Child Health Bureau • Centers for Disease Control & Prevention • Joint Committee on Infant Hearing • American Academy of Audiology • American Speech-Language-Hearing Association • National Association of the Deaf Why is Implementation of Newborn Hearing Screening Accelerating? Improved Screening Techniques/Equipment Acceptance by Policy Makers Increased Number of Successful Programs Public Awareness/Demand Why is Early Identification of Hearing Loss so Important? • Hearing loss occurs more frequently than any other birth defect. Rate Per 1,000 of Permanent Childhood Hearing Loss in UNHS Programs Site Sample Size Prevalence Per 1000 Rhode Island (3/93 - 6/94) 16,395 1.71 Colorado (1/92 - 12/96) 41,976 2.56 New York (1/95 - 12/97) 69,761 1.95 Texas (1/94 - 6/97) 52,508 2.15 Hawaii (1/96 - 12/96) 9,605 4.15 New Jersey (1/93 - 12/95) 15,749 3.30 Incidence per 10,000 of Congenital Defects/Diseases 40 30 30 20 5 6 10 11 12 1 2 0 ia m U ne lA PK el C le ck a Si fid bi a in s Sp ct fe de e b m m ro Li nd Sy te n la ow pa D or lip ft le ss C Lo g rin ea H Why is Early Identification of Hearing Loss so Important? • Hearing occurs more frequently than any other birth defect. • Undetected hearing loss has serious negative consequences. Grade Equivalents Reading Comprehension Scores of Hearing and Deaf Students 10.0 9.0 8.0 7.0 6.0 5.0 4.0 3.0 2.0 1.0 Deaf Hearing 8 9 10 11 12 13 14 15 16 17 18 Age in Years Schildroth, A. N., & Karchmer, M. A. (1986). Deaf children in America, San Diego: College Hill Press. Effects of Unilateral Hearing Loss Normal Hearing Keller & Bundy (1980) (n = 26; age = 12 yrs) Math Language Peterson (1981) (n = 48; age = 7.5 yrs) Math Language Bess & Thorpe (1984) (n = 50; age = 10 yrs) Social Blair, Peterson & Viehweg (1985) (n = 16; age = 7.5 yrs) Math Language Culbertson & Gilbert (1986) (n = 50; age = 10 yrs) Math Language Social Average Results Math = 30th percentile Language = 25th percentile Social = 32nd percentile 0th 10th 20th Unilateral Hearing Loss 30th 40th Percentile Rank 50th 60th Effects of Mild Fluctuating Conductive Hearing Loss Teele, et al., 1990 194 children followed prospectively from 0-7 years. Days child had otitis media between 0-3 years assessed during normal visits to physician. Data on intellectual ability, school achievement, and language competency individually measured at 7 years by "blind" diagnosticians. Results for children with less than 30 days OME were compared to children with more than 130 days adjusted for confounding variables. Outcome Measure WISC-R Full Scale Metropolitan Achievement Test Math Reading Goldman Fristoe Articulation Effect Size for Less vs. More OME .62 .48 .37 .43 Teele, D.W., Klein, J.O., Chase, C., Menyuk, P., Rosner, B.A., and the Greater Boston Otitis media Study Group (1990). Otitis media in infancy and intellectual ability, school achievement, speech, and language at age 7 years. The Journal of Infectious Diseases, 162, 685-694. Why is Early Identification of Hearing Loss so Important? • Hearing loss occurs more frequently than any other birth defect. • Undetected hearing loss has serious negative consequences. • There are dramatic benefits associated with early identification of hearing loss. Yoshinaga-Itano, et al., 1996 Compared language abilities of hearing-impaired children identified before 6 months of age (n = 46) with similar children identified after 6 months of age (n = 63). All children had bilateral hearing loss ranging from mild to profound, and normally-hearing parents. Language abilities measured by parent report using the Minnesota Child Development Inventory (expressive and comprehension scales) and the MacArthur Communicative Developmental Inventories (vocabulary). Cross-sectional assessment with children categorized in 4 different age groups. Yoshinaga-Itano, C., Sedey, A., Apuzzo, M., Carey, A., Day, D., & Coulter, D. (July 1996). The effect of early identification on the development of deaf and hard-of-hearing infants and toddlers. Paper presented at the Joint Committee on Infant Hearing Meeting, Austin, TX. Language Age in Months Expressive Language Scores for Hearing Impaired Children Identified Before and After 6 Months of Age 35 30 25 20 15 10 Identified BEFORE 6 Months Identified AFTER 6 Months 5 0 13-18 mos (n = 15/8) 19-24 mos (n = 12/16) 25-30 mos (n = 11/20) Chronological Age in Months 31-36 mos (n = 8/19) Boys Town National Research Hospital Study of Earlier vs. Later 129 deaf and hard-of-hearing children assessed 2x each year. Assessments done by trained diagnostician as normal part of early intervention program. Language Age (yrs) 6 Identified <6 mos (n = 25) Identified >6 mos (n = 104) 5 4 3 2 1 0 0.8 1.2 1.8 2.2 2.8 3.2 3.8 Age (yrs) Moeller, M.P. (1997).Personal communication , [email protected] 4.2 4.8 Implementing Effective EHDI Programs out Then a miracle occurs Start Good work, but I think we might need just a little more detail right here. Is the Glass Half Empty or Half Full? • Half full? More than 2.5 million babies are screened every year prior to discharge Less than 30 hospitals with UNHS in 1993; compared with almost 2500 today 37 states have passed legislation related to newborn hearing screening Or half empty? 1,500 hospitals are not yet screening for hearing loss Almost 1.5 million babies are NOT screened every year prior to discharge Existing legislation is of variable quality Follow-up rates are often alarmingly low Some hospitals have unacceptably high referral rates Status of Early Hearing Detection and Intervention (EHDI) in the United States Diagnosis before 3 months Screening Intervention before 1 month before 6 months Medical Home Data Management and Tracking Program Evaluation and Quality Assurance Family Support!! Status of EHDI Programs in the US: Universal Newborn Hearing Screening • With over half of all babies are screened prior to discharge, has newborn hearing screening become the standard of care? • There are hundreds of excellent programs - - - regardless of the type of equipment or protocol used • Many programs are still struggling with high refer rates and poor follow-up Typical UNHS Screening Protocols (example for 1,000 newborns) Inpatient Screening 1 Stage OAE / AABR Inpatient Screening Inpatient Screening Fail=80 Pass=920 Fail=40 Outpatient Screening n=80 Fail=10 Pass=70 Diagnosis n=10 Diagnosis n=40 Pass=960 Fail=20 Pass=980 Diagnosis n=20 Hearing Loss=3 Normal Hearing=7 Hearing Loss=3 Normal Hearing=37 Hearing Loss=3 Normal Hearing=17 Status of EHDI Programs in the United States • Universal Newborn Hearing Screening • Effective Tracking and Follow-up as a part of the Public Health System Purposes of an EHDI Data System Research Program Improvement and Quality Assurance Screening Diagnosis Intervention Medical, Audiological and Educational Rate Per 1000 of Permanent Childhood Hearing Loss in UNHS Programs Site Sample Size Prevalence Per 1000 % of Refers with Diagnosis Rhode Island (3/93 - 6/94) 16,395 1.71 42% Colorado (1/92 - 12/96) 41,976 2.56 48% New York (1/96 - 12/96) 27,938 1.65 67% Utah (7/93 - 12/94) 4,012 2.99 73% Hawaii (1/96 - 12/96) 9,605 4.15 98% Tracking "Refers" is a Major Challenge (continued) Initial Refer Rescreen Rescreen Refer Births Screened Rhode Island (1/93 - 12/96) 53,121 52,659 (99%) 5,397 (10%) 4,575 (85%) 677 (1.3%) Hawaii (1/96 - 12/96) 10,584 9,605 (91%) 1,204 (12%) 991 (82%) 121 (1.3%) New York (1/96-12/96) 28,951 27,938 (96.5%) 1,953 (7%) 1,040 (53%) 245 (0.8%) Options for Developing an EHDI Patient/Data Management System • Develop your own • Modify an existing system, for example • • • electronic birth certificate, or “heelstick” data management system Purchase an existing system Can EHDI Data Management be Combined with Heelstick? • Both do initial screening of babies in the nursery prior to hospital discharge • Both do outpatient screening for many babies • Poor follow-up is biggest challenge for hearing screening • Heelstick programs extremely successful with follow-up • Infrastructure for Heelstick follow-up already exists Issues to be Resolved Before Combining EHDI with Heelstick Follow-up Systems • Recording results of EHDI on heelstick form is only the beginning • Timing and procedures of data collection/entry are quite different for EHDI • Electronic transfer of data from screening equipment to data form • Availability of staff with expertise in EHDI issues to do follow-up • Hospital staff need timely access to data • Costs of modifying data entry/ reporting systems and duplicate data entry Efficiency of Early Hearing Detection and Intervention in a Statewide Evaluation 1999 (n=43,547) 2000 (n=46,771) 2001(6 mos.) (n=23,307) 85.2% 92.8% 70.7% 85.5% 93.4% 63.4% 87.5% 93.7% 74.4% Outpatient completion (state average) 70.1% 10 most effective hospitals 94.5% 10 least effective hospitals 45.3% 67.1% 95.9% 52.9% 68.3% 94.7% 58.08% 133 of 357 37.3% 165 of 380 43.4% 41 of 110* 40% % of babies who complete Diagnostic 33 of 133 Eval & have permanent hearing loss 24.8% 65 of 165 39.4% 12 of 41* 29.3% Inpatient Refer Rates (state average) 10 most effective hospitals 10 least effective hospitals Reported Completion of Diagnostic Evaluations (state average) Number of babies still “in process” *only 3 months worth of data 224 215 69 Status of EHDI Programs in the United States • Universal Newborn Hearing Screening • Effective Tracking and Follow-up as a part of the Public Health System • Appropriate and Timely Diagnosis of the Hearing Loss State Coordinator’s Ratings of Obstacles to Effective EHDI Programs Serious or Extremely Serious Obstacle Shortage of qualified pediatric audiologists 49% Physicians don’t know enough about newborn hearing screening, diagnosis, and intervention 41% Unwillingness of third-party payers to reimburse for hearing screening 28% Status of EHDI Programs in the US: Audiological Diagnosis • Equipment and techniques for diagnosis of hearing loss in infants continues to improve • Severe shortages in experienced pediatric audiologists delays confirmation of hearing loss • State coordinators estimate only 56.1% “receive diagnostic evaluations by 3 months of age Confirmation of Permanent Hearing Loss 35 Coplan (1987) 19 Eissman et al. (1987) 30 Gustason (1987) 30 Meadow-Orlans (1987) 24 Yoshinago-Itano (1995) 25 Stein et al. (1990) 31 Mace et al. (1991) 56 O'Neil (1996) 3 Johnson et al. (1997)* 3 Vohr et al. (1998)* 0 10 20 30 40 50 Average Age in Months 60 70 Status of EHDI Programs in the United States • Universal Newborn Hearing Screening • Effective Tracking and Follow-up as a part of the Public Health System • Appropriate and Timely Diagnosis of the Hearing Loss • Prompt Enrollment in Appropriate Early Intervention Status of EHDI Programs in the US: Early Intervention • Current system designed to serve infants with bilateral severe/profound losses--but, majority of those identified have mild, moderate, and unilateral losses • Part C of IDEA is severely under utilized • State Coordinators estimate: – Only 53% of infants with hearing loss are enrolled in EI programs before 6 months of age – Only 31% of states have adequate range of choices for EI programs Who is Eligible for Part C Services? • • • • • • • • • • Child has a profound, permanent sensorineural hearing loss in both ears (PTA>100 dB) Child has a profound, permanent sensorineural hearing loss in one ear (PTA>100dB), but normal hearing in the other ear Child has a moderate, permanent sensorineural hearing loss in both ears (PTA=55dB) Child has a mild, permanent sensorineural hearing in both ears (PTA=35dB) Child has a mild, fluctuating conductive hearing loss (PTA=35dB) in both ears due to otitis media (ear infections) Hawai'i EHDI Progress Age of Identification and Intervention 60 Identification Intervention Age in Months 50 40 30 20 10 0 pre 1992 1993 1994 1995 Year Data from Hawai’I Zero to Three Project 1996 1997 1998 Status of EHDI Programs in the United States • Universal Newborn Hearing Screening • Effective Tracking and Follow-up as a part of the Public Health System • Appropriate and Timely Diagnosis of the Hearing Loss • Prompt Enrollment in Appropriate Early Intervention • A Medical Home for all Newborns What Is a Medical Home? • A primary care physician provides care which is: • Accessible • Family-centered • Comprehensive • Continuous • Coordinated • Compassionate • Culturally effective EHDI and the Medical Home Birthing Hospital Parent Groups Audiology Mental Health Primary Provider 3rd Party Payers ENT Child/Family Deaf Community Services for Hearing Loss Early Intervention Programs Genetics Types of Hearing Loss Sensorineural versus Conductive versus Mixed Congenital versus Acquired (prelingual or post lingual) Progressive versus non-progressive Syndromic versus non-syndromic Familial versus sporadic What Causes Hearing Loss? Environmental CMV meningitis rubella prematurity head trauma asphyxiation ototoxicity hyperbilirubin other infections Syndromic Alport Norrie Pendred Usher Waardenburg Branchio-oto-renal Jervell and Lange-Nielsen ~50% Congenital Hearing Loss ~50% ~30% Non-syndromic Autosomal dominant Genetic 21% Autosomal recessive 77% ~70% ~1% X-Linked ~1% Mitochondrial Common Forms of Syndromic Hearing Loss Syndrome Main Features (in addition to hearing loss) Alport Kidney problems Branchio-oto-renal Neck cysts and kidney problems Jervell and Lange-Nielsen Heart problems Neurofibromatosis Type 2 Nerve tumors near the ear Pendred Thyroid enlargement Stickler Unusual facial features, eye problems, arthritis Usher Progressive blindness Waardenburg Skin pigment changes Benefits of Genetic Testing for Hearing Loss • Determine the chances of hearing loss in subsequent children • Avoid unecessary (and often costly) tests such as electroretinograms, temporal bone imaging, and electrocardigrams • Anticipate potential health problems – Monitoring for myopia and early retinal detachment for Stickler syndrome – Renal examinations can identify kidney problems in BOR – Vitamin A therapy may be beneficial in slowing retinal degeneration in child with Usher syndrome – Treatment of children with Jervell and Lange-Nielsen syndrome can minimize cardiac complications • Dispel misinformation and offer emotional support by allaying parental guilt Connexin 26 • A protein responsible for intracellular communication (transfer of ions between the hair cells in the cochlea and their support cells) • Responsible for 20-30% of all congenital hearing loss • Several different mutations 35delG is found in 2-3% of all Caucasians of European descent 167delT is found in 5% of Ashkenazi Jewish population • Usually recessive, occasionally dominant • Almost always results in hearing loss that is: Congenital Severe-profound Non-progressive Non-syndromic Susceptibility to Aminoglycoside Ototoxicity • mitochondrial mutation A1555G in the rRNA gene in combination with exposure to aminoglycoside antibiotics results in rapid onset of hearing loss • prevalent in Chinese and other oriental ethnic groups but has also been found in Caucasians, Greeks, etc. Status of EHDI Programs in the United States • Universal Newborn Hearing Screening • Effective Tracking and Follow-up as a part of the Public Health System • Appropriate and Timely Diagnosis of the Hearing Loss • Prompt Enrollment in Appropriate Early Intervention • A Medical Home for all Newborns • Culturally Competent Family Support Emotions of Families with a Deaf or Hard of Hearing Baby • • • • (grief) Reactions to Unexpected Diagnosis (pressure) Urgency of Communication Decisions Search (confusion) Search for Experienced Professionals (isolation) Availability of Services and Support Communication Choices • American Sign Language • Total Communication • Auditory Verbal • Auditory-Oral • Cued Speech Information Information Wanted Wanted vs. vs. Received Received by by Parents Parents at Hearing Loss Confirmation Degree of loss Auditory system Amplification Educational options Speech/Lang dev Wanted Received Etiology Home activities *Written Information *Financial Support *Emotional Support *Parent Contacts *Referral Sources 0 20 40 60 80 Martin, George, O'Neal, & Daly (1987); *Sweetow & Barrager (1980) 100 Parent’s Attitudes About Newborn Hearing Screening (Results of a Statewide Evaluation) After all hearing tests were completed, how did you feel? Strongly Agree or Agree Worried about my baby’s hearing 11% Confused about the results of screening tests 10% Glad hearing screening is done at this hospital 91% Confident the hearing tests were correct 91% Frustrated by how long it took to get results 13% Happy with the professional way screening was done 86% Confident about what I needed to do next 88% If the analysis is limited to those whose babies did not pass the inpatient or outpatient screen After all hearing tests were completed, how did you feel? Worried about my baby’s hearing Strongly Agree or Agree total group subgroup 11% 24% Confused about the results of screening tests 10% 24% Glad hearing screening is done at this hospital 91% 70% Confident the hearing tests were correct 91% 70% Frustrated by how long it took to get results 13% 28% Happy with the professional way screening was done 86% 76% Confident about what I needed to do next 88% 56% EHDI Materials Available from “State” Programs (n=54) General Screening Brochure 39 states What To Do If Your Baby Refers 35 states What To Do If Your Baby has a Hearing Loss 41 states Guidelines for Audiologic Diagnostic Evaluations 30 states List of Qualified Pediatric Audiologists 39 states Brochure about Genetics of Hearing Loss 7 states Fair or Excellent Availability of Materials in other Languages 34 states Efforts by the Federal Government to Promote Early Identification of Hearing Loss • Federal funding for research and program development • NIH Consensus Development Conference in 1993 • Consortium for Universal Newborn Hearing Screening funded in 1993 • Marion Downs National Center for Infant Hearing Established in 1996 • National EHDI Technical Assistance System Established in 2000 • NIH and Dept of Educ Projects at Boys Town and University of North Carolina National EHDI Technical Assistance System • EHDI Network members located in each of ten geographic regions National EHDI Assistance Network Region VIII (91% currently born in UNHS hospitals) Terry Foust Region V Region II (26% currently born in UNHS hospitals) (16% currently born in UNHS hospitals) Karen Munoz Beth Prieve I Puerto Rico Virgin Islands X Region I VIII II Antonia MaxonB V III Region X (21% currently born in UNHS hospitals) VII Curt Whitcomb Region III (49% currently born in UNHS hospitals) IX Sean Kastetter VI Region IX (23% currently born in UNHS hospitals) Randi Winston Yusnita Weirather (38% currently born in UNHS hospitals) IV - Guam, American Samoa, Marshall Islands, Palau, No. Mariana Islands, Fed. Micronesia Region IV (46% currently born in UNHS hospitals) Faye McCollister Region VI (38% currently born in UNHS hospitals) Region VII (33% currently born in UNHS hospitals) Les Schmeltz = indicates the locations of MCHB Regional Offices Karen Ditty Patti Martin Examples of Network Activities • State-wide EHDI meetings • Individualized TA with state EHDI programs • Telephone Conference calls with State EDHI Coordinators • Assist with development of state plans and grant applications • Regional workshops on Diagnostic ABR – 6 weeks of on-line preparation – 2 day face-to-face workshop – 3 month follow-up practicum National EDHI Meetings • Next meeting: February 24-26, 2002 (Atlanta) • Speakers, panels, and round tables • State displays • Product exhibits (commercial and non-profit) • Networking opportunities National EHDI Technical Assistance System (continued) • EHDI Network members located in each of the MCHB regions • Information dissemination and training Support for Program Implementation • Implementation Guide • Booklets for AAP and March of Dimes • Materials posted at www.infanthearing.org • Video tape for parents • Evaluation instruments and procedures Sound Ideas Newsletter • Topical articles, suggestions for program improvement • Upcoming events • Available online or mailed National EHDI Technical Assistance System (continued) • EHDI Network members located in each of the MCHB regions • Information dissemination and training • Web site (www.infanthearing.org) www.infanthearing.org www.babyhearing.org National EHDI Technical Assistance System (continued) • EHDI Network members located in each of the MCHB regions • Information dissemination and training • Web site (www.infanthearing.org) • Collaboration with other groups and agencies National EHDI Technical Assistance System (continued) Collaboration with Other Groups and Agencies • Groups actively promoting and assisting with EHDI activities – AG Bell, NCHH, ASHA, AAA, JCIH, AAP, SKI-HI, ASDC, Boys Town, DSHPSHWA • Relevant groups whose main focus has been elsewhere – NEC*TAS, Early Head Start, 0-3, Family Voices, NCCC, AMCHP, AHEC, March of Dimes, MCH Health Policy Center Collaboration with AAP • AAP News article • Assisted with booklets for physicians and parents • Collaborated on implementation of recently funded EHDI Initiative – Chapter Champions – Speaker’s Kit – Bulletin Board – Physician Guidelines • Analysis of legislation • National survey of physicians “Take Home” Messages • Deceptively simple—the devil is in the details • EHDI is more than screening • Medical Home is where the action is • Thoughtful, ongoing, self appraisal • You’re not alone “I am a great believer in luck, and I find that the harder I work, the more I have of it.” ---Thomas Jefferson