Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
A COMPARISON OF STABILITY OF 3 & 6 MM MINISCREW
IMPLANTS IMMEDIATELY-LOADED WITH
TWO DIFFERENT FORCE LEVELS
IN THE BEAGLE DOG
Micah G. Mortensen, D.D.S.
An Abstract Presented to the Faculty of the Graduate School
of Saint Louis University in Partial Fulfillment
of the Requirements for the Degree of
Master of Science in Dentistry
2007
Abstract
Introduction: Because the minimum size and maximum
load of miniscrew implants (MSI) have not been established,
this study compared the stability of 3 mm and 6 mm long
MSIs.
Methods: Using a split-mouth experimental design, 3
mm and 6 mm long MSIs were placed into the jaws of mature
beagle dogs and immediately loaded with either 600 or 900g
of force.
Continuous forces were applied for six weeks by
reciprocally loading pairs of MSIs with NiTi coil springs.
The mandible received 3 mm MSIs, with 600g and 900g forces
being randomly assigned to the right and left sides.
In
the maxilla, 3 mm and 6 mm long MSIs were randomly assigned
to the two sides, and loaded with 600g of force.
An
unloaded, control MSI was placed in each quadrant.
success was defined as lack of MSI pull-out.
Overall
Net success
rates excluded MSIs that sheared off or MSIs that failed in
one dog that was frequently chewed his run bars and food
bowl.
Intraoral measurements of inter-implant distance and
MSI mobility, measured with the Periotest, were recorded at
weeks 0 and 6.
Results: The overall success rates of the 3
mm and 6 mm experimental MSIs were 66.7% and 100%,
respectively.
The net success rate was 95.2% for the 3 mm
experimental MSIs.
The overall success rates of 3 and 6 mm
control MSIs were 66.7% and 100%, respectively.
1
The net
success rate of 3 mm controls was 81.8%.
The overall
success rates of the 3 mm mandibular MSIs loaded with 600
and 900g of force were both 60%. The net success rates were
100% for those loaded with 900g, and 85.7% for those loaded
with 600g.
The overall success rate of the 3 mm
experimental MSIs placed in the maxilla was 80%, compared
to a 60% overall success rate in the mandible; the net
success rates were 100% and 85.7% in the maxilla and
mandible, respectively.
Except the overall differences in
success rates between 3 mm and 6 mm MSIs, there were no
significant differences associated with force or location.
Both 3 mm and 6 mm loaded MSI pairs showed significant
decreases in inter-implant distance, averaging 2.2 mm and
1.8 mm, respectively.
There was no significant correlation
between initial MSI mobility and success or failure of
MSIs.
Conclusions: Success rates of immediately-loaded
3 mm MSIs were significantly lower than those of
immediately-loaded 6 mm MSIs.
Both 3 mm and 6 mm loaded
MSI pairs experienced significant linear displacement.
There was no significant difference in success rates of 3
mm MSIs placed in the maxilla and mandible.
2
A COMPARISON OF STABILITY OF 3 & 6 MM MINISCREW
IMPLANTS IMMEDIATELY-LOADED WITH
TWO DIFFERENT FORCE LEVELS
IN THE BEAGLE DOG
Micah G. Mortensen, D.D.S.
A Thesis Presented to the Faculty of the Graduate School
of Saint Louis University in Partial Fulfillment
of the Requirements for the Degree of
Master of Science in Dentistry
2007
COMMITTEE IN CHARGE OF CANDIDACY:
Adjunct Professor Peter H. Buschang,
Chairperson and Advisor
Professor Rolf G. Behrents,
Assistant Professor Donald R. Oliver
i
Dedication
I dedicate this project to my beautiful wife Amy,
whose love and support made the completion of this project
possible.
I am grateful for her unwavering support
throughout my education.
I also dedicate this to my two wonderful children,
Samuel and Ella, who fill my life with joy.
I express gratitude to my parents for their years of
support and guidance throughout my life.
ii
Acknowledgements
I would like to acknowledge the following individuals:
Dr. Peter Buschang for chairing my thesis committee.
Thank you for your guidance, insights and time.
You have a
passion for teaching and instill a desire to learn upon
those you are entrusted to educate.
Dr. Rolf Behrents for serving on my thesis committee.
You are a great teacher and mentor.
all aspects of education show.
Your reflections on
Thank you for your time and
suggestions.
Dr. Donald Oliver for serving on my thesis committee.
It has been a privilege to work with you, and I truly
appreciate your thought-provoking guidance.
Dr. George Vogler, Wanda Morgenthaler, Nancy Roth, and
the entire Comparative Medicine Department for your many
hours caring for the dogs used in this project.
Dr. Heidi Israel for your assistance with the
statistics of this project.
Dr. Nancy Galvin for providing SEM images of the
miniscrew implants used in this study.
Dr. H.M. Kyung and the Dentos Corporation for
supplying the miniscrew implants used in this experiment.
The Orthodontic Education and Research Foundation for
contributing to the funding of this project.
iii
Table of Contents
List of Tables...........................................vi
List of Figures.........................................vii
CHAPTER 1: INTRODUCTION...................................1
CHAPTER 2: REVIEW OF THE LITERATURE
Types of Anchorage.......................................5
Simple Anchorage.....................................6
Stationary Anchorage.................................7
Reciprocal Anchorage.................................7
Intraoral Anchorage..................................8
Extraoral Anchorage..................................8
Intramaxillary Anchorage.............................8
Intermaxillary Anchorage.............................9
Traditional Anchorage Strategies........................10
Implants................................................14
Palatal Implants....................................17
Palatal Onplant.....................................20
Surgical Miniplate..................................21
Miniscrew Implants......................................22
Nomenclature........................................22
Design..............................................23
Surgical Procedure..................................26
Miniscrew Implant Studies...............................26
Risk Factors........................................27
Loading Time........................................29
Force Application...................................32
Placement Torque....................................34
Implant Length......................................36
Primary vs. Secondary Stability.....................37
Cortical Anchorage..................................39
References..............................................42
CHAPTER 3: JOURNAL ARTICLE
Abstract................................................53
Introduction............................................55
Materials and Methods...................................58
Animals.............................................58
Preparation.........................................58
Miniscrew Implants..................................60
Initial Measurements................................61
Loading of Miniscrew Implants.......................61
Interim.............................................62
iv
Statistical Methods.................................64
Results.................................................65
Success Rates by Implant Length.....................65
Success Rates by Location...........................67
Success Rates by Force Levels.......................68
Linear Displacement.................................68
Success/Mobility Correlations.......................69
Discussion..............................................69
Conclusions.............................................76
Acknowledgements........................................77
References..............................................77
Figures.................................................81
Tables..................................................87
Vita Auctoris............................................90
v
List of Tables
Table 2.1:
Properties of several commercially available
MSIs......................................25
Table 3.1:
Success rates of MSIs by length...........87
Table 3.2:
Success rates of MSIs by location.........88
Table 3.3:
Success rates of mandibular MSIs by force
level applied.............................89
vi
List of Figures
Figure 2.1:
The Straumann Orthosystem® (Institut
Straumann AG, Waldenburg, Switzerland)....18
Figure 2.2:
The Straumann Orthosystem® (Institut
Straumann AG, Waldenburg, Switzerland)
with transpalatal arch connection.........19
Figure 2.3:
The palatal onplant.......................20
Figure 2.4:
Example of miniplates.....................21
Figure 2.5:
Dentos AbsoAnchor Implants................24
Figure 2.6:
The Spider Screw®.........................24
Figure 2.7:
IMTEC Ortho Implant.......................24
Figure 2.8:
Stability Pattern of Endosseous Dental
Implants (From Raghavendra, Wood, and
Taylor, 2005).............................38
Figure 3.1
3 mm and 6 mm MSIs........................81
Figure 3.2
MSI placement locations and force levels
applied...................................82
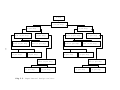
Figure 3.3
Experimental design outline...............83
Figure 3.4
Scanning electron microscope images of
MSIs......................................84
Figure 3.5
Stability patterns of endosseous dental
implants..................................85
Figure 3.6
Failure times for 3 mm MSIs...............86
vii
Chapter I: Introduction
Since the early days of orthodontics, anchorage
control has been one of the more difficult goals of
treatment.
Anchorage control is essential for establishing
the proper position of teeth.
While the idea of “absolute”
anchorage is often pursued, it is seldom achieved.
Many
attempts have been made to minimize the deleterious side
effects of moving certain teeth while maintaining the
position of others.
This is, however, difficult to
accomplish using tooth-borne anchorage alone. Teeth serving
as anchor units invariably undergo unwanted tooth movement.
Therefore, auxiliary sources of anchorage, such as
headgears, palatal buttons, and transpalatal and lingual
arches are typically employed.
Although these devices
improve the level of anchorage control, they do not allow
for complete control over dental movements.
Furthermore,
many of these methods rely on patient compliance, which
often cannot be expected.
Lack of compliance leads to
further loss of anchorage control and can result in
compromised treatment results, prolonged treatment, and
frustration for both the patient and practitioner.
Several forms of implants are now being used to
establish absolute anchorage and avoid unwanted tooth
1
movement.
Restorative implants are approximately 4 mm in
diameter and 7 to 20 mm in length.
When placed in the
dental arches and allowed to heal, they may be used for
orthodontic anchorage in addition to being prosthetic
replacements for teeth.
However, the arch space needed,
healing times, and strict location requirements limit their
use.
Palatal implants (3.3-3.75 mm X 4-6 mm) and onplants
(10 mm wide X 2 mm thick) have also been used for
orthodontic anchorage.
Unlike restorative implants,
palatal implants may be used in patients who do not require
replacement of missing teeth.
However, they have drawbacks
similar to restorative implants in that they require
significantly invasive surgery for their placement.
Mechanical attachment to palatal implants is also more
complicated than their restorative counterparts.
Onplants
were developed as sources of absolute anchorage without the
requirement for bone preparation.
However, they still
require surgical interventions and extended healing times,
and their use has not become commonplace.
Recently, miniscrew implants (MSIs) have gained
attention among orthodontists worldwide.
Their small size
(1.2-2 mm X 5-10 mm) allows them to be placed almost
anywhere, including between the roots of teeth.
2
Moreover,
surgical procedures for their placement and removal are
minimal, requiring only topical anesthetic in some
situations.
MSIs are also much less expensive than
restorative implants.
For these reasons, it appears that
MSIs are becoming the dominant player in the realm of
implant orthodontics.
Although MSI use is well-documented in the
literature1-6, there is no consensus regarding optimal
implant length.
Doi7 recently studied the stability of 6 mm
long MSIs that were immediately loaded with 300 or 600g of
force.
Over 90% of the 48 MSIs remained stable over a 5
week period.
The tissues surrounding 12 of the MSIs were
evaluated histologically. The analysis revealed that
several of the MSIs had only 3.5 mm of threads placed into
bone. Despite this, they remained stable when immediately
loaded with up to 600g of force.
This finding is the basis
of the present study, which proposes to evaluate the
stability of immediately-loaded 3 mm long MSIs.
When
compared to longer implants, 3mm long MSIs might be
expected to subject the patient to less risk during the
surgical placement.
There are currently no reports of 3 mm
long MSIs in the literature.
The purpose of this study is
to insert 3 mm MSIs into the jaws of beagle dogs,
3
immediately load them with orthopedic forces, and determine
their stability over a 6 week period.
This study is also based on the notion that MSIs gain
the majority of their retention from their location in the
cortical plate.
Because cortical bone is, by nature, much
denser than cancellous bone, it is theorized that the MSI
need not be significantly longer than the cortical plate
thickness.
The following review of the literature will begin with
a review of anchorage and its significance to orthodontic
tooth movement.
By explaining the importance of anchorage,
the use of implants for orthodontic anchorage will be
better understood.
The evolution of implant anchorage will
then be presented.
Because MSIs will be used in the
current study, emphasis will be placed on them.
Numerous
studies describing the use and clinical results of MSIs
will be discussed. This will serve to outline what work has
been done, and what remains to be done in the field of MSI
orthodontics.
4
Chapter II: Review of the Literature
In 1686, Sir Isaac Newton formulated the laws of
motion.
The third law, which states that for every action
there is an equal and opposite reaction, has particular
importance to orthodontics.
The negative effects of these
equal and opposite reactions are observed when malposed
teeth are moved into desirable positions and when, at the
same time, the reactive forces move other teeth into
undesired positions.
Anchorage to resist undesirable tooth
movement is the goal of many procedures that orthodontists
perform when moving teeth.
Ideally, only the malpositioned
teeth should be moved, leaving the well positioned teeth in
their correct location.
Types of Anchorage
According to Graber8, orthodontic anchorage refers to
the nature and degree of resistance to displacement offered
by an anatomic unit when used for the purpose of moving
teeth.
Anchorage can be divided into seven different
categories and three subtypes.
It will be shown that most
of these depend on factors such as the health of the
periodontium, tooth and root anatomy, occlusion, and
5
patient compliance.
These are presented in contrast to
implant anchorage, which is absolute, and can be totally
independent of patient compliance.
While miniscrew
implants are capable of replacing many traditional
anchorage strategies, they can also be used in conjunction
with them.
Therefore, a complete understanding of the
terminology used and types of anchorage employed is useful.
This review of traditional anchorage strategies will also
serve as a comparison to the simpler nature of absolute
implant anchorage.
Simple Anchorage
With simple anchorage, the axial inclination of the
tooth or teeth that make up the anchorage unit is changed
or displaced in the plane of space in which the force is
being applied (i.e., tipping).
The surface area of the
tooth’s root factors into this concept; a tooth with more
than one root has more anchorage potential than a single
rooted tooth.8
The amount of root attached to alveolar bone
also plays a role.
A periodontally compromised tooth will
have less functional surface area and thus less anchorage
potential than a periodontally healthy tooth.
6
Stationary Anchorage
Stationary anchorage occurs when the anchorage unit is
moved bodily (without tipping) in the same plane of space
as the force placed upon it.9
Because bodily movement
requires more force than tipping, this form of anchorage is
superior to simple anchorage.
Root surface area and
occlusion can both influence the amount of stationary
anchorage achieved.
Reciprocal Anchorage
When the resistance of one or more dental units are
employed to move one or more opposing dental units, the
result is reciprocal anchorage.
An example of this occurs
when anterior and posterior teeth are connected (via
elastomerics or coil springs) across an extraction site.
Reciprocal anchorage is used to simultaneously protract the
posterior teeth while the anterior teeth are being
retracted into the extraction site.
This form of anchorage
also applies when the maxillary arch is reciprocally
connected to the mandibular arch via intermaxillary
elastics.8
7
Intraoral Anchorage
Intraoral anchorage is entirely located within the
oral cavity and usually consists of the teeth, but may
include the palate and the oral musculature.8
Nance buttons
and lip bumpers are examples of intraoral anchorage
appliances.
Extraoral Anchorage
Any form of anchorage outside the oral cavity is
termed extraoral anchorage.
Headgears are commonly
employed to eliminate the reciprocal side effects seen with
many forms of intraoral anchorage.
Extraoral anchorage is
often used in the correction of maxillomandibular
relationships.8
Intramaxillary Anchorage
When anchorage is entirely contained within a single
dental arch, intramaxillary anchorage is utilized.10
Common
examples include transpalatal and lingual arches and Nance
buttons.
This anchorage may be simple, stationary, or
reciprocal in nature.8
8
Intermaxillary Anchorage
Intermaxillary anchorage is utilized when the
anchorage units of one dental arch are used to bring about
tooth movement in the opposing dental arch.8
Class II
elastics pit the anterior movement of the mandibular dental
arch against the posterior movement of the maxillary arch.
Tweed’s mechanics utilize intermaxillary anchorage in the
correction of Class II malocclusions.
While anchorage affects tooth movement in the
transverse and vertical dimensions, the primary focus of
the clinician is usually anteroposterior tooth movement.
Marcotte11 described anteroposterior anchorage as either A,
B, or C types.
In his description, type A refers to no
movement of the posterior teeth as anterior teeth are
retracted.
Type B is a “reciprocal anchorage” situation in
which the anterior and posterior units move equal amounts.
Type C anchorage is utilized when the posterior teeth are
protracted, with less posterior movement of the anterior
teeth.
These anchorage types have also been referred to as
maximum, moderate, and minimum, respectively.12
Anchorage is a factor that must be considered in every
orthodontic case.
While maximum anchorage is often the
goal of treatment, it is rarely obtained.
9
Indeed, Nanda13
has defined maximum anchorage as up to 25% movement of the
posterior teeth.
Traditional Anchorage Strategies
Many attempts have been made to limit the undesirable
movements of certain teeth while moving others.
As
mentioned, teeth differ in the amount of root surface
attached to bone.
The more root surface present in an
anchorage unit, compared to the tooth or teeth being moved,
the less anchorage will be lost.
This principle can be
utilized to establish one of the simplest forms of
anchorage, when the posterior teeth are ligated together
and used to retract an anterior tooth (or teeth).
The
expectation is that the posterior anchorage will overwhelm
that of the anterior teeth, resulting in greater retraction
of the anterior teeth than protraction of the posteriors.
While this is usually true, significant posterior
protraction does occur.
Dincer and Iscan14 measured
posterior anchorage loss versus canine retraction.
Extraction spaces were closed with reverse closing loops.
Their results showed 2.5 mm of anchorage loss when
maxillary canines were retracted 4.0 mm, and 1.3 mm of
anchorage loss when mandibular canines were retracted 2.7
mm.
Thiruvenkatachari and colleagues15 evaluated anchorage
10
loss of molars when canines were retracted into first
premolar extraction sites.
MSIs were placed unilaterally
in the maxillary and mandibular arches of 8 patients, and
in the maxilla only of 2 patients.
Space closure was
accomplished by connecting either the MSI or the molars to
the canines with closed-coil springs.
from 4 to 6 months.
Retraction lasted
Mean anchorage losses were 1.6 mm in
the maxilla and 1.7 mm in the mandible on the side where
molars were used for anchorage.
Where MSIs were used for
retraction, anchorage loss of the molars averaged 0 mm.
Tweed’s16 intraoral anchorage preparation involved
tipping the posterior teeth distally in order to resist the
undesired movements involved with the use of intermaxillary
elastics. Like tent stakes in the ground, a distally
inclined tooth might be expected to resist anterior and
superior movement more than a vertically oriented tooth.
Depending on the degree of posterior anchorage required,
different levels of posterior tooth tipping, and therefore
anchorage preparation, were established.
Extraoral anchorage, in the form of headgear, has been
used since the early days of orthodontics.
Gunnell
described the use of occipital anchorage in 1841, and
claimed to have used it since 1822.17
When worn, headgear
can add to the anchorage potential of the posterior teeth,
11
and can even move the maxillary teeth distally.
Case18
suggested that the only way to effect an upward and
backward movement of the maxillary posterior teeth was with
the use of headgear.
Cervical and high-pull headgears are
successful sources of extraoral anchorage.19,20
Anterior
headgear also provides for excellent control of anchorage
and control over the force vector applied.21 Anterior
headgear has been used for “en masse” retraction of
maxillary anterior teeth, without having to establish
posterior anchorage.22
In modern times, numerous appliances such as the
Pendulum, Distal Jet, and Jones-Jig have been used to
distalize maxillary molars.
However, even these appliances
are subject to the negative effects of Newton’s third law,
and unwanted proclination of anterior teeth is commonly
observed.23
Anchorage loss, measured at the incisors or
premolars, has been shown to vary from 0.2 to 2.2 mm.
Some
appliances, such as the Cetlin plate, use headgear wear to
minimize anterior tooth movement.
However, Ferro and
coworkers24 showed that even with cervical headgear use,
anterior anchorage loss occurs.
Their sample of 110
patients showed an average of 2.3 mm anterior anchorage
loss with 2.2 mm of maxillary molar distalization.
Although headgears (and removable appliances) offer
12
the clinician considerable control over the direction and
level of force applied, they require patient compliance,
which is almost entirely out of the orthodontist’s control.
Although compliance has been shown to be related to
duration of treatment, frequency and complexity of the
task,25 and pain experienced,26,27 it remains largely
unpredictable.
It is often said by seasoned orthodontists
that patient compliance has decreased over the years.
While it is unknown if this is true, it is clear that
compliance is less than perfect.
In a recent study,
patients were instructed to wear headgear for 14 hours per
day.
Despite knowing that their headgear use was being
monitored, patients only wore them for an average of 6.7
hours per day.
Furthermore, quality time (measured as
uninterrupted use) was only 1.8 hours per day.28
Headgears have other drawbacks as well.
They are
unesthetic and are becoming less socially accepted.
Headgears should not be worn while playing sports or
engaging in rough activities, as disengagement of the inner
bow can result in injuries to the face and eyes.
13
Implants
Even before Brånemark described osseointegration in
1981, attempts were made to directly attach dental devices
to the underlying bone.
In 1909, Greenfield29 patented a
predecessor to the hollow basket implant.
After removing a
cylindrical section of bone with a trephine bur, a hollow
cylindrical basket made of iridio-platinum was placed into
the bone.
The desired outcome was for bone to grow into
the basket, securing it in place.
However, the mesh
framework for the basket was not strong enough to withstand
occlusal forces, and premature loading was believed to have
contributed to its failure.30
With the development of new alloys in the 1940’s, it
became well established that vitallium was the most inert
alloy for use in surgery.31
Strock began using vitallium
screws for replacement of incisors.30
Gainsforth and
Higley32 placed vitallium implants in dogs in an effort to
achieve absolute orthodontic anchorage.
Thirteen 3.4 mm X
13 mm implants were placed in the mandibular rami of 6
mongrel dogs.
The maxillary first molars received crowns
with buccal tube attachments.
Maxillary canines were
banded and a wire ran from the canine through a tube on the
molar.
Distal to the molar tube, the wire was secured to
the mandibular implants via elastics.
14
One implant remained
unloaded.
Force levels on the loaded implants ranged from
140g to 200g.
The unloaded implant failed within 21 days.
The remaining implants all failed within 16-35 days.
It
was presumed that each of the screws failed due to the
communication with the oral cavity and the resultant
contact with the fluids and microorganisms of that region.
While the authors do not describe frank infection, it was
insinuated as the cause for failure.
It is possible that
intermittent loading contributed to their failure as well.
Despite this failed attempt, investigators continued to
develop this area of research.
In the early 1960s, Brånemark attempted to retrieve
optical chambers from bone, but found that they were
inseparably incorporated within the bone tissue, which
actually grew into thin spaces in the titanium33.
The work
by Brånemark and others34,35 demonstrated the mechanism by
which a metal fixture could be integrated in bone without
rejection by the body.
This phenomenon became known as
osseointegration, and was introduced to restorative
dentistry in 1965.
In 1969, Linkow utilized a blade implant for
orthodontic anchorage in which Class II mechanics were
employed.36,37
Blade implants have a wedge-shaped body that
sits in the alveolar bone.
The wedge tapers from top to
15
bottom and is approximately 1 mm wide at its greatest
dimension.
Because the length of blade implants can
approach 2 cm, they can only be used in edentulous areas.
On the body of the implant sits a narrow neck whose
uppermost part is broadened to bear the prosthesis.38
Linkow’s trial was significant in that it provides the
first example of successful intraosseous anchorage use in
orthodontics.
Blade implants have been used successfully
in other trials as well.39
Endosseous root form implants (approx. 4 mm X 9-15 mm)
became the most common type of implant for prosthetic
replacement of teeth, and have been used for orthodontic
anchorage as well.
Numerous reports have shown the
effectiveness of endosseous (restorative) implants for
orthodontic anchorage.40-44
These studies have shown that
restorative implants are capable of withstanding typical
orthodontic loads.
Restorative implants do have limitations, however.
The implant’s large size limits its use to partially
edentulous patients who need replacement of at least one
tooth.
Moreover, the implant must be positioned in its
final, ideal location before orthodontics begins.45
This
position can be difficult to determine, and requires an
inter-disciplinary approach.
Restorative implants also
16
require healing times of up to 6 months before they can be
loaded.
Because orthodontic treatment is itself a lengthy
process, any addition to the overall treatment time is
significant.
However, if a patient presents to the
orthodontist with a restorative implant already in place,
it may subsequently be used for anchorage during
treatment.46
Immediate provisional implants were developed as
temporary aids for prosthetic rehabilitation.
These
implants are approximately 1.5–2.0 mm X 10–18 mm and are
designed to be placed between regular dental implants to
support partial or complete dentures during the time the
restorative implants osseointegrate.
describe their use.47,48
Several papers
These implants are removed when the
final restorations are placed on the osseointegrated
restorative implants.
Because of their ease of use and
removal, immediate provisional implants encouraged
orthodontic applications.
Palatal Implants
Block49 noted that the use of restorative implants for
orthodontics is not practical for patients with complete
dentitions.
This represents a large portion, if not the
majority, of patients in a typical orthodontic practice.
17
Due to this limitation, palatal implants were developed as
a means of obtaining absolute implant anchorage outside the
dental arch.
The Straumann Orthosystem® (Institut
Straumann AG, Waldenburg, Switzerland) is an example of a
palatal implant.
It has a length of either 3 or 4 mm and a
threaded diameter of 3.75 mm.
Its design is based on a
traditional restorative implant; it consists of a selftapping body, a smooth cylindrical collar, and an octagonal
head used to connect attachments(Figure 2.1).50
Figure 2.1: The Straumann Orthosystem® (Institut Straumann
AG, Waldenburg, Switzerland)51
The surgical procedure involves removal of palatal
mucosa with a mucosal trephine, followed by pilot hole
creation with a series of burs and drills.
The implant is then inserted, covered, and allowed to
heal for 12 weeks,51 although healing times may equal those
of traditional restorative implants.52
18
After healing, a
second incision is made to uncover, and subsequently load
the implant.
Custom attachments (Figure 2.2) are usually
indicated, which require additional laboratory time and
cost.
Figure 2.2: The Straumann Orthosystem® (Institut
Straumann AG, Waldenburg, Switzerland) with
transpalatal arch connection51
Another limitation of the palatal implant is the
inability to place them in varied locations.
Site
specificity often requires the use of more complicated
attachments.
Finally, removal of palatal implants may be
accomplished with a hand ratchet, but may also require
trephination of the implant and surrounding bone, leaving
an extensive defect.51
Despite these limitations, the
success of palatal implants is well established.
19
Palatal Onplant
The surgical invasiveness of the palatal implant led
to the development of the palatal onplant.
The onplant is
a disk-shaped fixture (10 mm wide X 2 mm thick) with a
textured, hydroxyapatite-coated surface designed to
osseointegrate on the surface of the palatal bones (Figure
2.3).
Unlike restorative or palatal implants, the onplant
does not require bone perforation for placement.
After an
incision, it is placed subperiosteally onto the palate and
allowed to heal.
After healing, the onplant is uncovered
via an incision, and the abutment is attached.
Onplants
require two surgical procedures and 3 to 5 months of
healing time before they can be loaded.53,54
Figure 2.3: The palatal onplant55
Use of onplants is a relatively new area of research,
with the first successful use being reported in 1995.55
In
this report, an onplant was successfully loaded, in a
mongrel dog, with 11 oz. (approx. 300g) of continuous force
over a 5 month period.
Recently, an onplant was used for
orthopedic maxillary protraction with 400g of force applied
20
per side.54
Onplants have not gained widespread acceptance,
and there are few reports in the literature supporting
their use.
Surgical Miniplates
Surgical miniplates, such as the Skeletal Anchorage
System, are derivatives of surgical plates and bone screws
used for rigid fixation.
An extension of the surgical
plate was added to perforate the oral mucosa and serve as
an attachment for the orthodontic appliances (Figure 2.4).
The length of the extension arm ranges from 10.5-16.5 mm
and the system is secured with 2.0 X 5.0 mm screws.
Figure 2.4:
Example of miniplates56
It has been reported that the function of the anchor
plates is similar to that of an onplant, while the screws
function as implants.
As such, the Skeletal Anchorage
System reportedly gains anchorage from the osseointegration
effects of both the anchor plates and screws.57
Surgical
miniplates may be used in situations where restorative
21
implants are not feasible, such as in patients with
complete dentitions or insufficient bone to support a
restorative implant.
In 1992, the Skeletal Anchorage
System was used to correct a severe anterior crossbite in a
patient without molars that could be used for anchorage,
and with thin alveolar bone that could not retain
restorative implants.58
Miniplates were also recently used
to protract the maxilla in an 11 yr. old patient.59
In this
case, titanium miniplates were placed on the lateral nasal
wall of the maxilla and used as anchorage for face mask
protraction.
No tooth support was used.
A force of 350g
per side was applied for a period of 12 months, resulting
in an 8 mm anterior displacement of the maxilla.
Miniplates require a flap for placement, healing times of
approximately 3 months, and a second incision at time of
removal.60
Miniscrew Implants
Nomenclature
There is no consensus regarding the terminology used
to describe small implants used for orthodontic purposes.
MSIs are also referred to as microimplants, microscrew
implants, mini-implants, minidental implants, and screwtype implants.
“Micro,” short for “microscopic,” refers to
22
something requiring magnification to be seen.
This
description does not apply to any orthodontic implants.
“Mini,” short for “miniature,” refers to something small
compared with other objects of its type.
Because implants
used for orthodontics are small, screw shaped devices, they
will be referred to as miniscrew implants, or MSIs,
throughout this paper.
It has been suggested that the
orthodontic specialty adopt this term in order to
facilitate better communication among practitioners.61
Design
In recent years, many different MSI designs have been
developed.
Each design represents a different variant of a
screw’s basic features: length, diameter, thread width,
thread pitch, and head/end configuration.
It is important
to note that there is a difference between self-drilling
(drill-free) and self-tapping screws.
Self-tapping screws
have sharp threads that cut into a material upon insertion,
allowing them to advance when turned.
tapping.
All screws are self-
Self-drilling screws have a drill-shaped point
and a specially formed cutting flute that allow insertion
without prior drilling.
Drill-free screws have been shown
to exhibit more bone-to-metal contact and less mobility
than MSIs placed with a pre-drilled pilot hole.62
23
The
diameter of the threaded portion of the MSI varies among,
and within different manufacturers (Table 2.1).
For
example, the AbsoAnchor (Figure 2.5; Dentos Inc., Daegu,
Korea) is available in diameters ranging from 1.2 to 2.0
mm, the Spider Screw® (Figure 2.6; HDC Company, Sarcedo,
Italy) is either 1.5 mm or 2.0 mm in diameter,63 and the
IMTEC Ortho Implant (Figure 2.7; IMTEC Corporation,
Figure 2.5: Dentos
AbsoAnchor
Implants6
Figure 2.6: The
Spider Screw®63
Figure 2.7: IMTEC Ortho
Implant64
Ardmore, Oklahoma) comes in a single diameter of 1.8 mm.64
The advantage of a thinner screw is that it can be placed
in more locations, such as between the roots of teeth.
drawback, however, is the greater potential for screw
fracture.65
24
The
Table 2.1: Properties of several* commercially available
MSIs.
Name/Manufacturer
Length
(mm)
6, 8,
10
Diameter
(mm)
1.8 mm
Dentos AbsoAnchor
5, 6,
7, 8,
10, 12
HDC Company
Spider Screw
7, 9,
11
1.2,
1.3,
1.4,
1.5,
1.6,
1.7,
1.8, 2.0
1.5, 2.0
Dentaurum TOMAS
pin
8, 10
Mondeal LOMAS
Quattro
7, 9,
11
IMTEC Ortho
Implant
Head
SelfDesign
Drilling?
Circular
Yes
ball with
.028” tube
5 designs
Yes
available,
including
slot and
tube
designs
Bracket
design
with .021
X .025”
and .025”
slots
1.2
Bracket
design
with .022
X .028”
cross slot
1.5, 2.0
.022 X
.028” or
.018 X
.025” tube
and slot
1.5, 2.0
Bracket
design
with .022
X .028”
cross slot
No
No
Yes
Yes
5.4,
5.7,
5.8,
6.7,
7.4,
7.8,
8.7
* There are currently dozens of commercially available
MSIs. For conciseness, this table includes several of the
more widely used implants rather than an exhaustive list of
all those available.
Aarhus Anchorage
System
25
Surgical Procedure
It is generally accepted that surgical preparation for
MSI placement involves cleansing of the area followed by
local anesthetic infiltration.
Recently, some
practitioners have reported placing MSIs with only topical
anesthetic.66
Surgical placement procedures differ more than
surgical preparation. These range from mucoperiosteal flaps
and pilot drill access,67 to insertion of self-drilling
screws with hand drivers.61
Miniscrew Implant Studies
MSI use is becoming more widespread, and numerous case
reports have documented their use.1-3,68-71
There are,
however, few controlled studies that validate the manner in
which MSIs are being used.
For example, consensus is
lacking on the ideal MSI length, allowable force levels,
and loading times.
Before use of these MSIs can become
widespread, their potential applications and limitations
should be established by well-designed, scientific studies.
The remainder of this review will focus on studies
pertaining to orthodontic MSIs, emphasizing risk factors,
loading times, force levels, MSI lengths, and placement
26
torque.
The concepts of cortical anchorage and primary vs.
secondary stability will also be addressed.
Risk Factors
Many researchers cite various potential risk factors
for MSI failure.
Cope states that the minimum diameter to
avoid failure should be 1.5 mm.61
Melsen states that the
prognosis is poor in cases where: 1) the cortex is thinner
than 0.5 mm; 2) the mucosa is thick, leading to a greater
distance between the point of force application and the
center of resistance; 3) the MSI is inserted in an area
undergoing considerable bone remodeling, such as from
resorption of a deciduous tooth, or a recent extraction,
and; 4) the patient has systemic disease leading to bone
remodeling.65
While these suggestions appear logical, the
authors give them as opinions based on clinical experience
as opposed to specific research results.
Actually, only a
few studies have specifically evaluated the risk factors
for MSI failure.
One such study, by Miyawaki and
colleagues,72 evaluated the stability of three different MSI
systems, as well as a miniplate system, to determine the
factors that negatively affected the success of the MSIs
and miniplates.
They found that the 1-year success rate of
1.0 X 6 mm MSIs was significantly less than those measuring
27
1.5 X 11 mm or 2.3 mm X 14 mm; the success of the 1.0 x 6
mm MSIs was also less than that of miniplates secured with
2 screws measuring 2.0 X 5 mm.
The authors concluded that
the success rate of MSIs with 1.0 mm diameter was
significantly less than that of the other screws.
Their
rationale in selecting diameter over length as the
contributing factor was that all (10/10) of the 1.0 X 6.0
mm MSIs failed, while only 1 of 17 miniplates (secured with
2.0 X 5 mm screws) failed.
Because the miniplates were
secured with 5 mm long screws, length was not considered to
be a contributing factor to failure.
It seems logical,
however, that the differences in design between MSIs and
miniplates could also have been contributing factors to the
success of the miniplates.
Miyawaki’s group also found that flap surgery
contributed to patient discomfort, but did not increase the
risk of failure.
Inflammation of peri-implant tissue after
implantation was found to be a risk factor for mobility of
MSIs. However, no significant association was found between
the success rate and the following variables: MSI length,
kind of placement surgery, immediate loading, location of
implantation, age, gender, crowding of teeth,
anteroposterior jaw base relationship, controlled
periodontitis, or temporomandibular disorder symptoms.72
28
Cheng et al., who placed 140 MSIs (2 mm X 5-15 mm) in
44 patients, found that those placed in areas of inadequate
keratinized gingiva were more likely to fail.73
Other
authors have recommended placing MSIs in keratinized
gingiva, rather than mobile masticatory mucosa, in order to
avoid soft tissue inflammation and coverage of the MSI
head.74
Loading Time
Since the early days of implant dentistry, consensus
on loading protocols has been lacking.
Only recently have
researchers begun to make site and situation-specific
loading time recommendations.
Research has focused mainly
on restorative implants, and is only now beginning to
examine MSI loading and stability.
A brief history of
restorative implant loading will be presented along with
recent research involving MSIs.
It was previously mentioned that Strock began using
vitallium screws for replacement of incisors in 1939.
At
that time, he stated that immediate loading was feasible if
enough bone were present to allow for initial stability.
Modern researchers have also made the case for immediate
loading of implants.75
When placing restorative dental implants, the goal is
29
to achieve the maximum level of osseointegration possible.
Therefore, it has traditionally been thought that implants
should undergo up to a 6 month healing period before
loading.33
In 1984, Roberts et al. placed 4 pairs of 3.2 mm
X 8 mm implants into rabbit femurs and immediately loaded
them to each other, via springs, with 100g of force.
Within one week, spontaneous “torsional” bone fractures
were observed.
Ten other pairs of similar implants were
placed and allowed to heal for 6 weeks before being loaded
with the same amount of force.
Of the delayed-loading
implants, only 1 of 20 failed.
Roberts et al. concluded
that 6 weeks was the earliest time an implant could be
loaded after placement in a rabbit.
Since sigma (the
turnover time for one cycle of bone) is approximately 3
times longer in humans than rabbits, it was concluded that
the same duration equaled 18 weeks in humans.76
As restorative implant usage became more widespread,
researchers began to explore shorter healing periods.
In
1991, Lum et al. found that immediately loaded implants in
monkeys had similar stability and bone contact when
compared to delayed loaded implants.77
More recently
(1997), Tarnow and coworkers placed 69 implants in humans,
and immediately loaded them with a single-unit prosthesis.
Only 2 of the 69 implants failed.
30
These results suggest
that immediate loading of restorative implants may be
possible as long as the implants are splinted together to
minimize micromotion and encourage osseointegration.78
Similar to restorative implants, numerous healing
times have been suggested for orthodontic MSIs.
In the
early days of MSIs, a healing period up to 36 weeks in
length was recommended.79
Ohmae conducted a study on the
efficacy of MSIs for orthodontic intrusion in the beagle
dog.
After a six week healing period, the MSIs were loaded
with a 150g force.
At the end of the 18 week loading
period, 4.5 mm of intrusion was achieved, with all 36 of
the MSIs remaining stable.
Interestingly, the author
stated that the 6 week healing time may have been “too
short to allow enough osseointegration.”80
Immediate loading of MSIs is becoming more common,
with several reports in the literature to support the
practice.1,4,81,82
In 2006, Doi reported a study in which 48
6 mm MSIs were placed in the jaws of 4 beagle dogs.
Two
MSIs were immediately connected to each other by nickel
titanium coil springs that pulled either 300 or 600g of
force.
Two of the 48 MSIs were placed near erupting teeth
and failed shortly after placement.
This required their
removal, and the exclusion of the other MSI they were
paired with.
After 5 weeks, only 1 out of the remaining 44
31
MSIs demonstrated greater than 1 mm of mobility.
The
author concluded that MSIs can be loaded immediately with
typical orthodontic (300g), and even orthopedic force
levels (600g).7
This immediate loading is made possible by
the mechanical interdigitation of the implant screws with
the alveolar bone.
Owens83 recently placed 56 1.8 X 6 mm MSIs into the
jaws of 7 beagle dogs.
Of the 56 MSIs, 21 were immediately
loaded with either 25 or 50g of force.
Three of the
immediately loaded MSIs failed within 21 days of placement.
Retrospective radiographic analysis revealed that the 3
failed MSIs were placed into incompletely healed extraction
sites, which likely contributed to their failure.
Comparison of the delayed vs. immediately loaded maxillary
MSIs showed no differences in failure rate, indicating that
the timing of implant loading was not a determinant of
success.
It was concluded that the concern for a healing
period with restorative implants may not be applicable to
MSIs subjected to lighter forces.
Force Application
The forces applied to restorative implants in past
studies have ranged from 30g84 up to 1500g.85
In 1983, MSIs
loaded with 60, 120, and 180g of force showed no
32
significant movement at any force level over a 28 day
period.40
In 2004, Carrillo86 placed 96 MSIs into the buccal
and lingual cortical plates of 8 mature beagle dogs.
The
MSIs were immediately loaded with 25, 50, or 100g of force,
and were used to intrude the mandibular premolars.
One of
the 96 MSIs failed after 50 days of loading with 100g
force.
None of the remaining MSIs failed over the duration
of the 98-day study.
It was therefore concluded that
miniscrew implants have excellent stability and produce
significant amounts of tooth movement after immediate
loading with up to 100g of force.
Asikainen et al.87 placed 20 MSIs into the foreheads of
sheep and, after a 3 month healing period, loaded them with
250 to 350g of horizontally-directed force.
The MSIs
withstood the force until they were removed 3 months later.
MSIs have also successfully withstood forces of 1000g when
allowed to heal for 20 weeks.42
The maximum force level an immediately loaded MSI can
actually withstand has yet to be determined.
In 2004,
Pickard88 performed a study designed to evaluate the effects
of MSI orientation on stability and resistance to failure.
The study also sought to identify the maximum amount of
force that can be applied to MSIs in the human mandible.
In the study, MSIs were placed at either 90° or 45° angles
33
to the mandibular cortical plate of human cadaver bone, and
were tested to the point of failure in pull-out (tensile)
and shear tests.
In the shear tests, the MSIs aligned at
45° were tested from two directions: angled in a direction
towards (head pointing toward the direction of shear force)
and opposing (head pointed away like a tent stake) the axis
of shear force.
The pullout test implants aligned at 90°
had the highest force at failure, which was measured at 342
± 80.9 N (1 N = 102 g).
In the shear tests, the MSIs that
were angled in the same direction as the line of force
experienced significantly higher shear forces than those
MSIs angled away from the force (253 ± 74.05 N vs. 87 ± 27.2
N).
While the study does not directly describe maximum
force levels that MSIs can withstand under clinical loading
situations, the forces required to remove the implants were
considerably higher than typical orthodontic force levels.
Placement Torque
Two recent studies have examined the relationship
between implant placement torque and survival of
implants.89,90
In the first study, 23 patients received two
restorative implants each.
Each implant was placed with a
minimum insertion torque of 20 Ncm.
34
One of the implants
was restored and occlusally loaded within 24 hours of
placement.
Of the 23 implants that were immediately
loaded, 10 failed within 2 years.
In the delayed-loading
group, only 1 implant failed during the 2 year follow-up
period.
In the immediately loaded group, the relative risk
for implant failure was associated with insertion torque.
The authors concluded that an insertion torque above 32 Ncm
is necessary for osseointegration, and that immediate
loading should only be proposed if this minimum level of
insertion torque has been applied.89
As previously discussed, orthodontic MSIs are
designed, placed, and loaded in a different manner than
restorative implants.
Therefore, a study relating
placement torque of MSIs would be more helpful for the
orthodontic practitioner.
Such a study was performed by
Motoyoshi et al.,90 who sought to determine an adequate
level of placement torque for MSIs placed in the buccal
alveolar bone.
Forty-one orthodontic patients received a
total of 124 1.6 mm X 8 mm MSIs.
The peak value of implant
placement torque when tightening the implant into bone was
measured using a torque screwdriver.
ranged from 2 to 18 Ncm.
The placement torque
Of the 124 MSIs placed, 18
failed, for a success rate of 85.5%.
In the mandible, the
placement torque was significantly higher in the failure
35
group than in the success group, which was an unexpected
finding.
The success rate for MSIs with a placement torque
between 5 and 10 Ncm was significantly higher than that for
MSIs with a placement torque less than 5 Ncm or more than
10 Ncm.
According to the authors’ calculated risk ratio
for failure, the recommended placement torque should be
within the range of 5 to 10 N cm.
The authors conclude
that a “large implant placement torque” should not always
be used.
Other authors have shown that very high placement
torque can generate high levels of stress at the boneimplant interface, resulting in degeneration of the bone.91
Implant Length
Traditional restorative implants range from 3-4.75 mm
in diameter and 7-20 mm in length.
Failure rates of
restorative implants have been reported to be higher as the
length decreased.92
However, when forces are directed
tangentially rather than axially, the shorter length of the
MSI does not appear to result in failure.72
Numerous
studies have reported successful use of 6 mm long
MSIs.7,83,86,93,94
Deguchi et al. reported retention of 93 out
of 96 1 mm x 5 mm MSIs when loaded with 200-300g of force
for 3 months.95
To date, no studies evaluating the stability of
36
immediately-loaded 3 mm length MSIs have been reported in
the literature; nor are there reports of 6mm length MSIs
immediately-loaded with 900g of force.
Primary vs. Secondary Stability
The goal of implant orthodontics is to obtain maximum
stability of the implant, thereby allowing for absolute
anchorage.
The stability of restorative implants has been
shown to change in the initial weeks after their
placement.96
Stability can be divided into two phases:
primary and secondary stability (Figure 2.8).
Primary
stability is due to the mechanical interdigitation of the
implant with the bone.
Secondary stability is enhanced as
the bone heals around the implant surface.
Factors such as
timing of load, implant placement torque, and implant size
may also affect the primary and secondary stability of
implants.
Osseointegration is defined as bone-to-implant
contact at the light microscopic level.
According to
Cochran’s group, as soon as an implant is placed, certain
areas of its surface are in contact with bone and are
therefore, osseointegrated.97
This is referred to as
primary bone contact (primary stability).
As healing
occurs, this bone is remodeled, and areas of new bony
contact appear around the implant surface.
37
This remodeled
bony contact, termed secondary bone contact (secondary
stability), predominates at later healing times (Figure
2.8).
Stability Pattern of Endosseous
Dental Implants
Stability
(percent)
100
Primary
Stability
Secondary
Stability
Total Stability
75
50
25
0
0
1
2
3
4
5
6
7
8
Time (weeks)
Figure 2.8: Stability pattern of endosseous dental
implants. Adapted from Raghavendra, Wood, and Taylor.96
Primary stability is related to implant size and
placement torque.
Implants with greater dimension will
have a larger surface area in contact with bone, and
theoretically, more primary stability.
also related to secondary stability.
Implant length is
As the bone around an
implant heals, the cancellous bone turns over and is
replaced by denser bone that is more like the cortical
plate.
Secondary stability increases as more of the
implant becomes surrounded by denser bone.
38
As previously explained, very high placement torque
can result in degeneration of the bone surface.
While very
tight placement may temporarily increase primary stability,
secondary stability will be decreased as the bone
degenerates.
Modern implant studies have sought to achieve shorter
healing periods prior to implant restoration.
More rapid
secondary bone stability (i.e. healing) has been attempted
by modifying the implant surface.
For example the Institut
Straumann’s SLA implant has a sandblasted, large-grit,
acid-etched titanium surface.98
Orthodontic MSIs, on the
other hand, are actually designed to prevent maximum
osseointegration.
titanium alloy.
The usual design is a smooth-surfaced
The Mondeal LOMAS Quattro (Mondeal North
America, San Diego, CA) is manufactured with a polishing
technique that is designed to prevent osseointegration and
allow for easy removal.
Cortical Anchorage
As previously stated, the present study is based on
the notion that MSIs gain the majority of their retention
from their location in the cortical plate, and that the MSI
need not be significantly longer than the cortical plate
thickness.
Cortical bone is, by nature, much more dense
39
than cancellous bone.
Therefore, the threads of the MSI
are in more intimate contact with the cortical bone,
enhancing primary stability.
A recent study found a weak
but significant positive correlation (r = 0.39) between
cortical bone thickness and MSI pull-out strength in the
beagle dog.99
In that study, the maxillary and mandibular
anterior regions had the thinnest labial cortical bone,
averaging 1.3 mm.
This region also had the lowest mean
pull-out strength at 134.5 ± 24 N.
The posterior mandible
had the greatest mean thickness at 2.4 mm, and also had the
highest mean pull-out strength at 388.3 ± 23.1 N.
In other
words, the thicker the cortical bone, the greater the force
required to pull out the MSI.
Miyawaki et al. found a high mandibular plane angle
(MPA) to be a risk factor for failure of MSIs.72
It was
suggested that sufficient mechanical interdigitation
between the MSI and the cortical bone is an important
factor that affects the stability of the MSI.
The
relationship between a high MPA and cortical bone thickness
was not, however, explained by the authors.
The work of
Tsunori and colleagues helps to explain this relationship.
They showed that subjects with high MPAs have thinner
cortical bone in the posterior, mandibular buccal region
than those with low angles (1.5-2.7 mm avg. vs. 2.3-3.7 mm
40
avg.).100
It can be deduced that the reason a high MPA is a
risk factor for MSI failure is because of the thinner
cortical bone associated with this characteristic.
These
studies, and the report by Huja et al.,99 support the
concept that increased cortical bone thickness is related
to greater MSI stability and success.
Similarly, Melsen
states that the prognosis for primary stability of an MSI
is reported to be poor in cases where the cortex is thinner
than 0.5 mm and the density of the trabecular bone is low.65
It appears that the primary stability that the
cortical plate provides for MSIs is one factor related to
their success.
This study, which proposes to place 3 mm
long MSIs into the cortical plates of beagle dogs, will
provide further information on this notion.
Doi’s7
Building on
findings, we will investigate whether immediately-
loaded 1.3 X 3 mm MSIs can withstand orthopedic forces and
remain stable over a 6 week period.
41
References
1. Costa A, Raffainl M, Melsen B. Miniscrews as orthodontic
anchorage: a preliminary report. Int J Adult Orthodon
Orthognath Surg 1998;13:201-209.
2. Giancotti A, Greco M, Mampieri G, Arcuri C. Treatment of
ectopic maxillary canines using a palatal implant for
anchorage. J Clin Orthod 2005;39:607-611.
3. Lee JS, Park HS, Kyung HM. Micro-implant anchorage for
lingual treatment of a skeletal Class II malocclusion. J
Clin Orthod 2001;35:643-647; quiz 620.
4. Park HS, Bae SM, Kyung HM, Sung JH. Micro-implant
anchorage for treatment of skeletal Class I bialveolar
protrusion. J Clin Orthod 2001;35:417-422.
5. Park HS, Kyung HM, Sung JH. A simple method of molar
uprighting with micro-implant anchorage. J Clin Orthod
2002;36:592-596.
6. Kyung HM, Park HS, Bae SM, Sung JH, Kim IB. Development
of orthodontic micro-implants for intraoral anchorage. J
Clin Orthod 2003;37:321-328; quiz 314.
7. Doi PAK. A comparison of stability of immediately loaded
mini-implants with two different force levels in the beagle
dog. Center for Advanced Dental Education. St. Louis, MO:
Saint Louis University; 2006.
8. Graber TM. Orthodontics - Principles and practice.
Philadelphia, PA: W.B. Saunders; 1961.
9. Salzmann JA. Principles of orthodontics. Philadelphia,
PA: J.B. Lippincott Company; 1943.
10. Dewey M. Practical orthodontics. St. Louis, MO: The
C.V. Mosby Company; 1942.
42
11. Marcotte J. Biomechanics in orthodontics. Philadelphia,
PA: B.C. Decker Incorporated; 1990.
12. Giannelly A, Goldman H. Biologic basis of orthodontics.
Philadelphia, PA: Lea and Febinger; 1971.
13. Nanda RS. Biomechanics in clinical orthodontics.
Philadelphia, PA: W.B. Saunders Company; 1997.
14. Dincer M, Iscan HN. The effects of different sectional
arches in canine retraction. Eur J Orthod 1994;16:317-323.
15. Thiruvenkatachari B, Pavithranand A, Rajasigamani K,
Kyung HM. Comparison and measurement of the amount of
anchorage loss of the molars with and without the use of
implant anchorage during canine retraction. Am J Orthod
Dentofacial Orthop 2006;129:551-554.
16. Tweed CH. Clinical orthodontics. St. Louis, MO: C.V.
Mosby Company; 1966.
17. Weinberger BW. Orthodontics: An historical review of
its origin and evolution. St. Louis, MO: C.V. Mosby Co.;
1926.
18. Case CS. A practical treatise on the technics and
principles of dental orthopedia and prosthetic correction
of cleft palate. Chicago, IL: C.S. Case Company; 1921.
19. Pavlick CT, Jr. Cervical headgear usage and the
bioprogressive orthodontic philosophy. Semin Orthod
1998;4:219-230.
20. van Steenbergen E, Burstone CJ, Prahl-Andersen B,
Aartman IH. The role of a high pull headgear in
counteracting side effects from intrusion of the maxillary
anterior segment. Angle Orthod 2004;74:480-486.
21. Miethke RR. Indication and effectiveness of the J-hook
headgear. Prakt Kieferorthop 1990;4:267-284.
43
22. Guray E, Orhan M. "En masse" retraction of maxillary
anterior teeth with anterior headgear. Am J Orthod
Dentofacial Orthop 1997;112:473-479.
23. Chiu PP, McNamara JA, Jr., Franchi L. A comparison of
two intraoral molar distalization appliances: distal jet
versus pendulum. Am J Orthod Dentofacial Orthop
2005;128:353-365.
24. Ferro F, Monsurro A, Perillo L. Sagittal and vertical
changes after treatment of Class II division 1 malocclusion
according to the Cetlin method. Am J Orthod Dentofacial
Orthop 2000;118:150-158.
25. Sinha PK, Nanda RS. Improving patient compliance in
orthodontic practice. Semin Orthod 2000;6:237-241.
26. Sergl HG, Klages U, Zentner A. Pain and discomfort
during orthodontic treatment: causative factors and effects
on compliance. Am J Orthod Dentofacial Orthop 1998;114:684691.
27. Egolf RJ, BeGole EA, Upshaw HS. Factors associated with
orthodontic patient compliance with intraoral elastic and
headgear wear. Am J Orthod Dentofacial Orthop 1990;97:336348.
28. Brandao M, Pinho HS, Urias D. Clinical and quantitative
assessment of headgear compliance: a pilot study. Am J
Orthod Dentofacial Orthop 2006;129:239-244.
29. Greenfield EJ. Mounting for artificial teeth. U.S.A.
Patent No. 943,113; 1909: p. 1-3.
30. Strock AE. Experimental work on a method for the
replacement of missing teeth by direct implantation of a
metal support into the alveolus. Am J Orthod 1939;25:467472.
44
31. Venable CS, Stuck WG. Clinical uses of vitallium.
Philadelphia, PA: Lippincott Co.; 1943.
32. Gainsforth BL, Higley LB. A study of orthodontic
anchorage possibilities in basal bone. Am J Orthod Oral
Surg 1945;31:406-416.
33. Brånemark PI. Osseointegration and its experimental
background. J Prosthet Dent 1983;50:399-410.
34. Brånemark PI, Adell R, Breine U, Hansson BO, Lindstrom
J, Ohlsson A. Intra-osseous anchorage of dental prostheses.
I. Experimental studies. Scand J Plast Reconstr Surg
1969;3:81-100.
35. Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year
study of osseointegrated implants in the treatment of the
edentulous jaw. Int J Oral Surg 1981;10:387-416.
36. Ring ME. Pause for a moment in dental history: a
thousand years of dental implants: a definitive history part 1. Compendium 1995;16:1060-1069.
37. Ring ME. Pause for a moment in dental history: a
thousand years of dental implants: a definitive history part 2. Compendium 1995;16:1132-1142.
38. Linkow LI. Theories and techniques of oral
implantology. St. Louis, MO: The C.V. Mosby Co.; 1970.
39. Haanaes HR, Stenvik A, Beyer-Olsen ES, Tryti T, Faehn
O. The efficacy of two-stage titanium implants as
orthodontic anchorage in the preprosthodontic correction of
third molars in adults--a report of three cases. Eur J
Orthod 1991;13:287-292.
40. Gray JB, Steen ME, King GJ, Clark AE. Studies on the
efficacy of implants as orthodontic anchorage. Am J Orthod
1983;83:311-317.
45
41. Odman J, Lekholm U, Jemt T, Branemark PI, Thilander B.
Osseointegrated titanium implants--a new approach in
orthodontic treatment. Eur J Orthod 1988;10:98-105.
42. Turley PK, Kean C, Schur J, Stefanac J, Gray J, Hennes
J et al. Orthodontic force application to titanium
endosseous implants. Angle Orthod 1988;58:151-162.
43. Rasmussen R. A new dimension--implant-assisted
orthodontics. Dent Implantol Update 1991;2:24-26.
44. Thilander B, Odman J, Grondahl K, Friberg B.
Osseointegrated implants in adolescents. An alternative to
replacing teeth? Eur J Orthod 1994;16:84-95.
45. Spear FM, Mathews DM, Kokich VG. Interdisciplinary
management of single-tooth implants. Semin Orthod
1997;3:45-72.
46. Prosterman B, Prosterman L, Fisher R, Gornitsky M. The
use of implants for orthodontic correction of an open bite.
Am J Orthod Dentofacial Orthop 1995;107:245-250.
47. Lee JH, Frias V, Lee KW. Use of an immediate
provisional implant to support a full-arch interim
restoration: a clinical report. J Prosthodont 2005;14:127130.
48. Krennmair G, Furhauser R, Weinlander M, Piehslinger E.
Maxillary interim overdentures retained by splinted or
unsplinted provisional implants. Int J Prosthodont
2005;18:195-200.
49. Block MS. Discussion on: {Mandibular lengthening by
distraction osteogenesis using osseointegrated implants and
an intraoral device.}. J Oral Maxillofac Surg 1996;54:600.
50. Cousley R. Critical aspects in the use of orthodontic
palatal implants. Am J Orthod Dentofacial Orthop
2005;127:723-729.
46
51. Crismani AG, Bernhart T, Bantleon HP, Cope JB. Palatal
implants: the Straumann Orthosystem. Semin Orthod
2005;11:16-23.
52. Huang LH, Shotwell JL, Wang HL. Dental implants for
orthodontic anchorage. Am J Orthod Dentofacial Orthop
2005;127:713-722.
53. Janssens F, Swennen G, Dujardin T, Glineur R, Malevez
C. Use of an onplant as orthodontic anchorage. Am J Orthod
Dentofacial Orthop 2002;122:566-570.
54. Hong H, Ngan P, Han G, Qi LG, Wei SH. Use of onplants
as stable anchorage for facemask treatment: a case report.
Angle Orthod 2005;75:453-460.
55. Block MS, Hoffman DR. A new device for absolute
anchorage for orthodontics. Am J Orthod Dentofacial Orthop
1995;107:251-258.
56. Sugawara J, Nishimura M. Minibone plates: the skeletal
anchorage system. Semin Orthod 2005;11:47-56.
57. Sugawara J, Daimaruya T, Umemori M, Nagasaka H,
Takahashi I, Kawamura H et al. Distal movement of
mandibular molars in adult patients with the skeletal
anchorage system. Am J Orthod Dentofacial Orthop
2004;125:130-138.
58. White LW, Sugawara J. JCO interviews Dr. Junji Sugawara
on the skeletal anchorage system. J Clin Orthod
1999;33:689-696.
59. Kircelli BH, Pektas ZO, Uckan S. Orthopedic protraction
with skeletal anchorage in a patient with maxillary
hypoplasia and hypodontia. Angle Orthod 2006;76:156-163.
47
60. Daimaruya T, Takahashi I, Nagasaka H, Umemori M,
Sugawara J, Mitani H. Effects of maxillary molar intrusion
on the nasal floor and tooth root using the skeletal
anchorage system in dogs. Angle Orthod 2003;73:158-166.
61. Cope JB. Temporary anchorage devices in orthodontics: a
paradigm shift. Semin Orthod 2005;11:3-9.
62. Kim JW, Ahn SJ, Chang YI. Histomorphometric and
mechanical analyses of the drill-free screw as orthodontic
anchorage. Am J Orthod Dentofacial Orthop 2005;128:190-194.
63. Maino BG, Maino G, Mura P. Spider Screw: skeletal
anchorage system. Prog Orthod 2005;6:70-81.
64. Herman R, Cope JB. Miniscrew implants: IMTEC mini ortho
implants. Semin Orthod 2005;11:32-39.
65. Melsen B. Mini-implants: Where are we? J Clin Orthod
2005;39:539-547; quiz 531-532.
66. Mah J, Bergstrand F. Temporary anchorage devices: a
status report. J Clin Orthod 2005;39:132-136; discussion
136; quiz 153.
67. Kanomi R. Mini-implant for orthodontic anchorage. J
Clin Orthod 1997;31:763-767.
68. Bae SM, Park HS, Kyung HM, Kwon OW, Sung JH. Clinical
application of micro-implant anchorage. J Clin Orthod
2002;36:298-302.
69. Paik CH, Woo YJ, Boyd RL. Treatment of an adult patient
with vertical maxillary excess using miniscrew fixation. J
Clin Orthod 2003;37:423-428.
70. Park YC, Chu JH, Choi YJ, Choi NC. Extraction space
closure with vacuum-formed splints and miniscrew anchorage.
J Clin Orthod 2005;39:76-79.
48
71. Yun SW, Lim WH, Chun YS. Molar control using indirect
miniscrew anchorage. J Clin Orthod 2005;39:661-664.
72. Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T,
Takano-Yamamoto T. Factors associated with the stability of
titanium screws placed in the posterior region for
orthodontic anchorage. Am J Orthod Dentofacial Orthop
2003;124:373-378.
73. Cheng SJ, Tseng IY, Lee JJ, Kok SH. A prospective study
of the risk factors associated with failure of miniimplants used for orthodontic anchorage. Int J Oral
Maxillofac Implants 2004;19:100-106.
74. Costa A, Pasta G, Bergamaschi G. Tissue depths for
temporary anchorage devices. Semin Orthod 2005;11:10-15.
75. Cooper L, De Kok IJ, Reside GJ, Pungpapong P, RojasVizcaya F. Immediate fixed restoration of the edentulous
maxilla after implant placement. J Oral Maxillofac Surg
2005;63:97-110.
76. Roberts WE, Smith RK, Zilberman Y, Mozsary PG, Smith
RS. Osseous adaptation to continuous loading of rigid
endosseous implants. Am J Orthod 1984;86:95-111.
77. Lum LB, Beirne OR, Curtis DA. Histologic evaluation of
hydroxylapatite-coated versus uncoated titanium blade
implants in delayed and immediately loaded applications.
Int J Oral Maxillofac Implants 1991;6:456-462.
78. Tarnow DP, Emtiaz S, Classi A. Immediate loading of
threaded implants at stage 1 surgery in edentulous arches:
ten consecutive case reports with 1- to 5-year data. Int J
Oral Maxillofac Implants 1997;12:319-324.
79. Roberts WE, Marshall KJ, Mozsary PG. Rigid endosseous
implant utilized as anchorage to protract molars and close
an atrophic extraction site. Angle Orthod 1990;60:135-152.
49
80. Ohmae M, Saito S, Morohashi T, Seki K, Qu H, Kanomi R
et al. A clinical and histological evaluation of titanium
mini-implants as anchors for orthodontic intrusion in the
beagle dog. Am J Orthod Dentofacial Orthop 2001;119:489497.
81. Freudenthaler JW, Haas R, Bantleon HP. Bicortical
titanium screws for critical orthodontic anchorage in the
mandible: a preliminary report on clinical applications.
Clin Oral Implants Res 2001;12:358-363.
82. Takano-Yamamoto T, Miyawaki S, Koyama I. Can implant
orthodontics change the conventional orthodontic treatment?
Dental Diamond 2002;27:26-47.
83. Owens SE. Experimental evaluation of tooth movement in
the beagle dog utilizing the mini-implant for orthodontic
anchorage. Dallas, TX: Baylor College of Dentistry; 2004.
84. Mendez-Villamil CA, Oliver SV. [Periodontometric
evaluation of induced mobility by orthodontic forces in
vitreous carbon implants in baboons]. Rev Odontol P R
1981;18:4-9.
85. Turley PK, Roth P. Orthodontic force application to
vitallium subperiosteal implants. J Dent Res 1983;62A:282.
86. Carillo R. Intrusion and root resorption of
multiradicular teeth using mini-screw implants as
anchorage. Dallas, TX: Baylor College of Dentistry; 2004.
87. Asikainen P, Klemetti E, Vuillemin T, Sutter F, Rainio
V, Kotilainen R. Titanium implants and lateral forces. An
experimental study with sheep. Clin Oral Implants Res
1997;8:465-468.
88. Pickard MB. Effect of mini-screw orthodontic anchorage
implant orientation on implant stability and resistance to
failure at the bone-implant interface. Master's Thesis.
Baylor College of Dentistry. Dallas, TX. 2004.
50
89. Ottoni JM, Oliveira ZF, Mansini R, Cabral AM.
Correlation between placement torque and survival of
single-tooth implants. Int J Oral Maxillofac Implants
2005;20:769-776.
90. Motoyoshi M, Hirabayashi M, Uemura M, Shimizu N.
Recommended placement torque when tightening an orthodontic
mini-implant. Clin Oral Implants Res 2006;17:109-114.
91. Meredith N. Assessment of implant stability as a
prognostic determinant. Int J Prosthodont 1998;11:491-501.
92. Naert I, Quirynen M, van Steenberghe D, Darius P. A
six-year prosthodontic study of 509 consecutively inserted
implants for the treatment of partial edentulism. J
Prosthet Dent 1992;67:236-245.
93. Park HS, Lee SK, Kwon OW. Group distal movement of
teeth using microscrew implant anchorage. Angle Orthod
2005;75:602-609.
94. Park HS, Kwon TG, Kwon OW. Treatment of open bite with
microscrew implant anchorage. Am J Orthod Dentofacial
Orthop 2004;126:627-636.
95. Deguchi T, Takano-Yamamoto T, Kanomi R, Hartsfield JK,
Jr., Roberts WE, Garetto LP. The use of small titanium
screws for orthodontic anchorage. J Dent Res 2003;82:377381.
96. Raghavendra S, Wood MC, Taylor TD. Early wound healing
around endosseous implants: a review of the literature. Int
J Oral Maxillofac Implants 2005;20:425-431.
97. Cochran DL, Schenk RK, Lussi A, Higginbottom FL, Buser
D. Bone response to unloaded and loaded titanium implants
with a sandblasted and acid-etched surface: a histometric
study in the canine mandible. J Biomed Mater Res 1998;40:111.
51
98. Cochran DL, Morton D, Weber HP. Consensus statements
and recommended clinical procedures regarding loading
protocols for endosseous dental implants. Int J Oral
Maxillofac Implants 2004;19 Suppl:109-113.
99. Huja SS, Litsky AS, Beck FM, Johnson KA, Larsen PE.
Pull-out strength of monocortical screws placed in the
maxillae and mandibles of dogs. Am J Orthod Dentofacial
Orthop 2005;127:307-313.
100. Tsunori M, Mashita M, Kasai K. Relationship between
facial types and tooth and bone characteristics of the
mandible obtained by CT scanning. Angle Orthod 1998;68:557562.
52
Chapter III: Journal Article
Abstract
Introduction: Because the minimum size and maximum
load of miniscrew implants (MSI) have not been established,
this study compared the stability of 3 mm and 6 mm long
MSIs.
Methods: Using a split-mouth experimental design, 3
mm and 6 mm long MSIs were placed into the jaws of mature
beagle dogs and immediately loaded with either 600 or 900g
of force.
Continuous forces were applied for six weeks by
reciprocally loading pairs of MSIs with NiTi coil springs.
The mandible received 3 mm MSIs, with 600g and 900g forces
being randomly assigned to the right and left sides.
In
the maxilla, 3 mm and 6 mm long MSIs were randomly assigned
to the two sides, and loaded with 600g of force.
An
unloaded, control MSI was placed in each quadrant.
success was defined as lack of MSI pull-out.
Overall
Net success
rates excluded MSIs that sheared off or MSIs that failed in
one dog that was frequently chewed his run bars and food
bowl.
Intraoral measurements of inter-implant distance and
MSI mobility, measured with the Periotest, were recorded at
weeks 0 and 6.
Results: The overall success rates of the 3
mm and 6 mm experimental MSIs were 66.7% and 100%,
respectively.
The net success rate was 95.2% for the 3 mm
53
experimental MSIs.
The overall success rates of 3 and 6 mm
control MSIs were 66.7% and 100%, respectively.
success rate of 3 mm controls was 81.8%.
The net
The overall
success rates of the 3 mm mandibular MSIs loaded with 600
and 900g of force were both 60%. The net success rates were
100% for those loaded with 900g, and 85.7% for those loaded
with 600g.
The overall success rate of the 3 mm
experimental MSIs placed in the maxilla was 80%, compared
to a 60% overall success rate in the mandible; the net
success rates were 100% and 85.7% in the maxilla and
mandible, respectively.
Except the overall differences in
success rates between 3 mm and 6 mm MSIs, there were no
significant differences associated with force or location.
Both 3 mm and 6 mm loaded MSI pairs showed significant
decreases in inter-implant distance, averaging 2.2 mm and
1.8 mm, respectively.
There was no significant correlation
between initial MSI mobility and success or failure of
MSIs.
Conclusions: Success rates of immediately-loaded
3 mm MSIs were significantly lower than those of
immediately-loaded 6 mm MSIs.
Both 3 mm and 6 mm loaded
MSI pairs experienced significant linear displacement.
There was no significant difference in success rates of 3
mm MSIs placed in the maxilla and mandible.
54
Introduction
Since the early days of orthodontics, anchorage control
has been one of the most challenging aspects of treatment.
While “absolute” anchorage is often pursued, it is seldom
achieved.
Auxiliary sources of anchorage, such as
headgears, palatal buttons, and transpalatal and lingual
arches, are typically employed to help preserve anchorage.
Although these devices preserve anchorage, they do not
allow for complete control over dental movements.
Furthermore, many of these methods rely on patient
compliance, which often cannot be expected.1
Lack of
compliance can lead to further loss of anchorage control,
prolonged and compromised treatments, and frustrations for
both the patient and practitioner.
Several types of implants are now being used to
establish absolute anchorage, avoid unwanted tooth
movement, and minimize the need for patient compliance.
Restorative implants, which are approximately 4 mm in
diameter and 7 to 18 mm long, have been used for
orthodontic anchorage and prosthetic replacements for
teeth.2-6
However, the surgery required, arch space needed,
healing times, and location requirements often limit the
use of restorative implants as an adjunct to orthodontic
treatment.7
Palatal implants (3.3-3.75 mm X 4-6 mm) also
55
require invasive surgery for their placement and removal,8
and mechanical attachment to palatal implants is more
complicated than their restorative counterparts.
Onplants
(10 mm wide X 2 mm thick), which were developed as a
potential source of absolute anchorage without the
requirement for bone penetration,9,10
also require surgical
procedures and extended healing times.
Their effectiveness
and efficiency have yet to be established.
Recently,
miniscrew implants (MSIs) have gained the attention of
orthodontists.
Their small size (1.2-2 mm X 5-12 mm)
allows them to be placed almost anywhere, with only minimal
surgery required for their placement.
MSIs are also much
less expensive than restorative implants.
Studies attempting to validate the use of MSIs have
produced conflicting results.
Human studies have
demonstrated variable success rates with MSIs, ranging from
49% to 100%.11,12
Animal studies, which allow for greater
control than human studies, perhaps provide the best means
of evaluating factors associated with MSI success.
Owens13
and Carillo14 reported 86% (18/21) and 99% (95/96) success
rates (defined as lack of gross mobility) after immediately
loading 6 mm MSIs in beagle dogs.
Doi15 recently
demonstrated a 94% success rate (lack of pull-out) for 6 mm
MSIs that were immediately loaded with 600g of force
56
(N=48).
Asikainen et al.,16 who placed 4.5 mm MSIs loaded
with 250-350g of force into the foreheads of sheep, showed
100% success after 3 months (N=20).
Ohmae et al.17 placed 4
mm long MSIs into the jaws of beagle dogs and observed 100%
success after loading them with 150g of force for 12-18
weeks (N=36).
Consensus is currently lacking with regard to ideal MSI
dimensions, allowable force levels, placement protocols,
and loading times, among other things.
The ideal MSI would
be easily placed and removed, affordable, biocompatible,
comfortable for the patient, would allow the use of simple
mechanics, and would remain stationary during treatment,
even when loaded with relatively high forces.
Importantly,
it would also be as small as possible, to minimize the risk
of contacting vital structures during placement.
The shortest MSI documented in the literature is 4 mm
long.17
However, Doi15 reported that many of the 6 mm MSIs
in his study that remained stable had only 3.5 mm of
threads placed into the bone.
It appears that the MSIs
gained sufficient stability from their location in the
cortical plate, without passing deep into the medullary
bone.
The cortex might be expected to be the primary
source of stability, especially primary stability.
MSIs
shorter than 3.5–4 mm MSIs might be expected to subject the
57
patient to less risk and discomfort during placement, but
may also be less stable than longer implants.
The purpose of this study was to experimentally compare
the difference in stability between 3 mm and 6 mm long MSIs
immediately-loaded with 600g of force, as well as the
difference in stability between 3 mm long MSIs immediatelyloaded with either 600g or 900g of force over a 6 week
period.
Materials and Methods
Animals
The sample included five healthy male, 10-15 month old
beagle dogs (approximate weight 9kg).
A soft diet
(Sensible Choice, Royal Canin, St Peters, MO and Purina
Ground, Purina Farms, Gray Summit, MO) was implemented
three weeks prior to MSI placement.
The dogs were housed
individually in the Comparative Medicine Department of
Saint Louis University Medical School.
All procedures were
approved by the Saint Louis University Animal Care
Committee (Authorization #1551).
Preparation
The dogs were injected with buprenorphine HCL
(Carpuject®, Hospira, Inc, Lake Forest, IL) 0.01 mg/kg SC
58
and carprofen (Rimadyl®, Pfizer Animal Health, Exton, PA)
4mg/kg subcutaneous for analgesia.
Acepromazine maleate
(VEDCO, Inc., St. Joseph, MO) 0.04 mg/kg was given
subcutaneously as a pre-anesthetic agent, along with
ampicillin (Fort Dodge Animal Health, Fort Dodge, IA) 10
mg/kg as a prophylactic measure.
Induction was performed
using propofol (Baxter Healthcare Corp., Irvine, CA) 3-4
mg/kg IV and isoflurane (IsoSol™, VEDCO, Inc., St. Joseph,
MO) 1-2%.
An IV drip of 0.9% sodium chloride (Baxter
Healthcare Corp, Deerfield, IL) was given at a rate of
20mg/kg/hr to maintain hydration.
Prior to MSI placement,
pre-operative periapical radiographs were taken in order to
determine if adequate space was present for MSI placement.
The sites were then swabbed with 0.12% chlorhexidine
gluconate (Acclean®, Henry Schein, Inc., Melville, NY) and
infiltrated with 0.25% bupivicaine HCl (Abbott
Laboratories, North Chicago, IL).
Six mandibular MSIs were
placed through the alveolar mucosa, approximately 5 mm
apical to the root furcations of the third and fourth
premolars and first molar.
To prevent the mucosa from
wrapping around the MSI during insertion, a tissue punch
(Imtec Corporation, Ardmore, OK) was used in the mandible.
Six maxillary MSIs were placed between the roots of the
second and third premolars and first molar, approximately 3
59
mm palatal to the gingival margins of the teeth.
All MSIs
were placed with a hand driver without pre-drilling.
Immediately after the MSIs were placed, periapical
radiographs were taken to verify that the roots had not
been contacted.
Miniscrew Implants
The MSIs used for this study were the AbsoAnchor®
system (Dentos, Inc., Daegu, Korea).
Two different lengths
of MSIs were used for the study: 3 mm and 6 mm (Figure
3.1).
The 6 mm MSIs are commercially available.
The 3 mm
MSIs were manufactured for this project by Dentos, Inc.
All MSIs measured 1.3 mm in diameter.
The tips of the MSIs
had a notched design that allows for self-drilling.
As a
modification for this study, the coronal surface of each
MSI was dimpled with a diamond bur, to serve as a
registration point for measurement.
Twelve MSIs were placed in each of the five dogs,
including eight experimental (loaded) and four control
implants (Figures 3.2 & 3.3).
The 3 mm MSIs in the right
and left sides of the mandible were randomly loaded with
either 600 or 900g of force.
3 mm or 6 mm MSIs, loaded
with 600g of force, were randomly assigned to the right and
left sides of the maxilla.
Because previous animal studies
60
have reported excessive tissue overgrowth around MSIs
placed buccally in the maxilla,13-15 the maxillary MSIs were
placed palatally rather than buccally.
A pair of
experimental MSIs was placed in each quadrant approximately
20 mm apart with one control MSI, of the same length,
placed slightly anterior to the midpoint between the two
experimental MSIs.
Initial Measurements
Primary stability was initially confirmed by exerting
manual pressure with the hand driver and a cotton forcep.
After taking periapical radiographs, mobility of the MSIs
was measured using the Periotest device (Medizintechnik
Gulden, Lautertal, Germany).18,19
Linear measurements were made between pairs of
experimental MSIs in each quadrant using a digital caliper
(Chicago Brand Industrial Inc., Fremont, CA).
The inter-
implant distance and Periotest mobility measurements were
repeated three times and the median values were used for
the statistical analyses.
Loading of Miniscrew Implants
After the initial measurements were taken, the MSIs
were loaded by ligating two 9 mm nickel titanium coil
61
springs (#428-650, The Orthodontic Store, Gaithersburg, MD)
between each pair of experimental implants.
The distances
that the NiTi coil springs needed to be activated in order
to obtain 600g and 900g of force were pre-determined with a
force gauge to be 13.4 and 18.2 mm, respectively.
These
distances were verified intraorally using the digital
caliper.
The springs were ligated to the MSIs using 0.012”
stainless steel ligature wire.
The ends of the ligature
wires were encapsulated with flowable composite (Natural
Elegance™, Henry Schein Incorporated, Melville, NY) to
minimize soft tissue irritation and to ensure that the
appliances remained intact.
The control implants remained
unloaded.
Interim
The dogs were monitored daily for six weeks following
the initial placement.
Each day, an intraoral examination
was performed to verify that the appliances were intact and
to evaluate the soft tissue response.
The study areas were
irrigated daily with 0.12% chlorhexidine gluconate
(Acclean®, Henry Schein, Inc., Melville, NY) in order to
flush food particles from the MSIs and springs.
For 10 days after MSI placement, all dogs were given
subcutaneous injections of 10 mg/kg aqueous ampicillin
62
(Fort Dodge Animal Health, Fort Dodge, IA) to minimize
infection, and 4 mg/kg SC carprofen (Rimadyl®, Pfizer
Animal Health, Exton, PA) to control inflammation and pain.
These were given for 10 days after MSI placement.
One dog
experienced severe tissue inflammation and overgrowth
around the mandibular implants and springs, which required
an additional 21 days of carprofen administration.
If an MSI failed (i.e., was pulled out) during the
course of the 6 week study, it was replaced within 1 to 7
days.
MSIs that failed during the last week of the study
were not replaced.
Replacement MSIs served only to provide
an anchor for the force being placed on the original,
intact, experimental MSI; no assessments of the replaced
MSIs were performed.
Six weeks following initial MSI placement, the dogs
were sacrificed with a lethal dose (3-5 mL) of
pentobarbital (Euthanasia-5, Henry Schein, Inc., Port
Washington, NY).
Subsequently, the distances between each
pair of study MSIs were again measured three times with a
digital caliper.
The dogs were then used in a study by
Caraway20, which measured maximum pull-out force of the
MSIs.
63
Statistical Methods
MSI success was defined as lack of MSI pullout.
Descriptive statistics were used to examine the success
rates of the MSIs, according to MSI length, location (i.e.,
maxilla vs. mandible), and force level.
Success rates of
the 20 control MSIs were also evaluated according to MSI
length and location.
Chi-square tests were used to analyze the associations
between MSI success or failure with length (3 mm vs. 6 mm),
location (maxilla vs. mandible), and force level (600 vs.
900g).
When appropriate (i.e., any cell N<5), Fisher’s
exact test was used to determine the statistical
significance of the chi-square values.
The Phi
coefficient, a measure of the degree of association between
two binary variables, was also used to evaluate the
relationship between success and length.
Intra-class correlations (ICC) were used to determine
the reliability of the three successive measurements
obtained with the Periotest.
An ICC of 0.80 or greater
indicates good reliability.
The ICCs, described in terms
of a Cronbach’s alpha, were calculated between measures 1
and 2, measures 1 and 3, and measures 2 and 3.
The median
Periotest mobility value was obtained for each MSI.
64
The Wilcoxon signed-rank test for related samples was
used to evaluate changes in inter-implant distances
(displacement).
Because displacement was measured as the
distance (a single value) between each pair of experimental
MSIs, the median Periotest mobility values for both MSIs in
the pair were averaged and compared against the single
displacement value.
Pearson’s correlation coefficient was
used to analyze the relationship between initial MSI
mobility and displacement of experimental MSIs.
In order to determine the association between initial
MSI mobility and success, the median values of the three
mobility measurements were converted to an ordinal scale.
Periotest values, which range between -8 and +50, were rescaled to ordinal values as follows: -8 to +6, +7 to +21,
+22 to +36, and +37 to +50.
Spearman’s rho correlation
coefficient was used to analyze the correlation between MSI
success or failure and initial mobility.
All statistics were performed using SPSS version 14.0
(SPSS Incorporated, Chicago, IL).
Results
Success Rates by Implant Length
The overall success rates of the 3 mm and 6 mm
experimental MSIs were 66.7% and 100%, respectively (Table
65
3.1), with the differences being statistically significant
(Χ²=4.03, p=.045).
of the study.
Failed MSIs were inspected at the end
Of the failed 3 mm experimental MSIs, the
tips of five were found to have sheared during placement
Caraway20 demonstrated that only one of the
(Figure 3.4).
successful MSIs was found to have a sheared tip.
the sheared MSIs, the success rate was 80%.
Excluding
Sixty percent
(6/10) of the 3 mm experimental MSIs that failed were from
dog #3.
This dog was described by the supervising
veterinarian as being unusually active and was regularly
observed chewing on its food bowl and the run bars of its
cage.
Because this activity may have contributed to MSI
failures, success rates were also reported after excluding
this animal.
The net success rate of 3 mm experimental
MSIs, excluding those that sheared and those placed in dog
#3, was 95.2%.
After these exclusions, the difference in
success rates between 3 mm and 6 mm experimental MSIs was
not statistically significant (Χ²=0.35, p=.557).
The overall success rates of the 3 mm and 6 mm control
MSIs were 66.7% and 100%, respectively (Table 3.1).
Of the
five 3 mm control MSIs that failed, one was found to have a
sheared tip, and one belonged to dog#3, resulting in a net
success rate of 81.8%.
Neither the overall (Χ²=1.98,
p=.160) nor the net (Χ²=0.93, p=.334) differences in
66
success rates between 3 mm and 6 mm control MSIs were
statistically significant.
The Phi coefficient showed a low, significant
association (φ=0.32, p=.045) between experimental MSI
length and success.
The control MSIs demonstrated no
significant association between length and success (φ=0.33,
p=.160).
Success Rates by Location
The overall success rates of 3 mm experimental MSIs
were 80% in the maxilla and 60% in the mandible (Table
3.2).
After excluding those that sheared and those placed
in dog #3, success rates were 100% for those placed in the
maxilla and 85.7% for those placed in the mandible.
The
differences in success between 3 mm experimental MSIs in
the maxilla and mandible were not statistically significant
either before (Χ²=1.20, p=.273) or after (Χ²=0.65, p=.421)
the exclusions.
The overall success rates of 3 mm control
MSIs were 80% in the maxilla and 60% in the mandible (Table
3.2).
After exclusions, success rates of 3 mm control MSIs
were 100% for those placed in the maxilla and 71.4% for
those placed in the mandible.
The differences in success
between control MSIs in the maxilla and mandible were not
67
statistically significant either before (Χ²=0.60, p=.439)
or after (Χ²=1.07, p=.301) exclusions.
Success Rates by Force Levels
The overall success rates of 3 mm mandibular MSIs
loaded with 600 and 900g of force were both 60% (Table
3.3).
After exclusions, the success rates were 100% for
900g of force, and 85.7% for 600g of force.
The
differences in success rates between 3 mm mandibular MSIs
loaded with 600g and 900g of force were not statistically
significant either before (Χ²=0.00, p=1.000) or after
(Χ²=0.93 p=.335) exclusions.
Linear Displacement
All of the loaded implant pairs showed significant
decreases in inter-implant distances during the six week
experimental period.
The mean displacement of the eight 3
mm MSI pairs that remained intact throughout the
experimental period was 2.2 mm, with a range of 0.4-4.4 mm.
The five pairs of loaded 6 mm MSIs that remained intact
showed a mean decrease in inter-implant distance of 1.8 mm,
with a range of 1.0-3.4 mm.
The difference in linear
displacement between the 3 mm and 6 mm MSI pairs was not
statistically significant (p=.369).
68
The mean displacement of the 3 mm MSI pairs loaded
with 600g of force was 2.0 mm (N=6), compared to a mean
displacement of 3.1 mm for the 3 mm MSI pairs loaded with
900g of force (N=2).
This difference was statistically
significant (p=.012).
Success/Mobility Correlations
The intra class correlations showed good reliability
between successive mobility measurements with the
Periotest.
The average Cronbach’s alpha was 0.97.
There
was no significant correlation between initial Periotest
mobility and success or failure of experimental (r=0.10,
p=.506) or control (r=-0.27, p=.350) MSIs.
There was no
statistically significant correlation between initial
Periotest mobility and displacement of the experimental
MSIs (r=0.00, p=.993).
Discussion
During the six week course of the study, ten 3 mm
experimental and five 3 mm control MSIs failed.
Six of
these failed 3 mm MSIs were found to have sheared tips.
Since only one of the 30 MSIs that remained stable had a
sheared tip, it appears that shearing of the MSIs may have
contributed to their failures.
69
The tip of a self-drilling
screw is designed to draw the rest of the screw into the
bone.
Once damaged, the tip is unable to advance, causing
the threaded barrel to strip the bone when turned.
For
these reasons, success rates were calculated after
excluding those MSIs that were found to be sheared.
As
previously mentioned, success rates were also calculated
after excluding all of the MSIs placed in dog #3, which was
regularly observed chewing on the run bars and food bowl.
These exclusions complicate the interpretation of the study
results, for it is impossible to determine how much of an
effect these external factors may have had on MSI failures.
Until further studies are performed, overall rather than
net success rates should be used for comparative purposes.
This study was based on the notion that MSIs gain the
majority of their primary stability (mechanical retention)
from the cortical plate.
Due to the differences in success
rates of 3 mm and 6 mm MSIs, primary stability may be
increased by contact with the medullary bone.
This could
explain why none of the 6 mm experimental MSIs failed.
Because secondary stability requires the first four to five
weeks of healing (Figure 3.5), adequate primary stability
is critical for short-term MSI success.
It is important to note that the length of the MSI
does not necessarily equal the depth of its insertion.
70
As
previously indicated, Doi15 found that several of the 6 mm
MSIs in his study had only been placed 3.5 mm into the
bone.
Caraway20 showed that the 6 mm MSIs used in the
present study were inserted an average of 3.9 mm into the
bone; the 3 mm MSIs were inserted an average of 1.6 mm.
Caraway also reported the cortical plate thickness of the
dogs used for this study to be approximately 2.1 mm.
On
that basis, the average 6 mm MSI passed through the
cortical plate and into the medullary bone, while the
average 3 mm MSI did not completely pass through the
cortex.
It is possible that the 3 mm MSIs that failed were
inserted less than required to attain primary stability.
This could also help to explain the high rate of failure of
3 mm MSIs in dog #3.
Had flaps been laid to ensure that
the MSIs were placed completely into bone, the success rate
of the 3 mm MSIs may have been higher.
The majority (7/10) of the 3 mm experimental MSIs that
were unsuccessful failed within the first two weeks of the
study (Figure 3.6).
primary stability.
This clearly indicates failures of
This was likely due to the minimal
surface area of the 3 mm MSIs that contacted bone.
There was no significant difference in success rates
between 3 mm MSIs immediately-loaded with 600g and 900g of
force, which is consistent with previous animal studies
71
comparing lower forces.
Owens13 found no differences in
success rates of 6 mm MSIs loaded with either 25 or 50g of
force; Carrillo14 reported no significant differences in
success rates of 6 mm MSIs loaded with 25, 50, or 100g,
and;
Doi15 found no significant difference in success rates
of 6 mm MSIs loaded with 300 or 600g.
It appears that the
level of force applied (up to 900g in this study) is not
the critical factor in determining MSI success or failure.
This suggests that force levels have to be high enough to
crush the surrounding bone before stability is affected.
Such force levels are likely outside the range of those
used in typical orthodontic situations since the maximum
pull-out force of 6 mm long MSIs have been reported to
range from 134-388 N (1 N = 102g).21,22
While there was not a significant difference in
success rates between 3 mm MSIs immediately-loaded with
600g and 900g of force, their overall success rates (both
60%, Table 3.3) were lower than those of 6 mm MSIs reported
by other authors.
Doi15, for example, reported a 96%
success rate for 6 mm MSIs immediately-loaded with 600g of
force.
These findings mirror those of the present study,
in that all 6 mm MSIs loaded with 600g of force were
successfully retained.
Collectively, then, it seems likely
that the overall lower success rate of the 3 mm MSIs in
72
this study was due to the shorter length of the MSI rather
than the relatively high force levels applied.
The 3 mm control MSIs had an overall success rate
similar to that of the 3 mm experimental MSIs.
However,
the control MSIs that were unsuccessful failed both early
and late in the six week study (Figure 3.6).
Because they
were unloaded, force cannot be implicated in their failure.
Although it is unclear exactly why they failed at a rate
equal to their loaded counterparts, length or depth of
insertion appear to be contributing factors.
The MSIs experienced significant linear displacement
during the course of the study, depending on the amount of
force.
MSI displacement has been reported to occur in both
immediately15 and delayed23 loaded MSIs.
The 6 mm,
experimental MSIs in the present study were displaced
approximately 0.9 mm (1.8/2), which was higher than in
previous reports.
Doi15, for example, reported an average
of 0.4 mm of displacement per implant, for 6 mm MSIs that
were immediately-loaded with 600g of force over a five week
period.
Because the 6 mm MSIs in the present study were
also loaded with 600g of force, it is unknown why they
experienced more displacement.
However, the increased
displacement of the 3 mm MSIs was likely due to the shorter
length of the MSIs.
Because the 3 mm MSIs loaded with 900g
73
were displaced more than those loaded with 600g, the
increased force appears to be a contributing factor.
While
the average displacement of the 3 mm MSI pairs was 2.2 mm,
geometry dictates that the apex of the average, individual,
3 mm MSI was only displaced 0.3 mm.
Considerably more
movement occurred at the implant head than at the apex,
which was surrounded by bone.
Two possibilities exist regarding the displacement
observed in this study: first, displacement could be but
one step in the progression toward eventual MSI failure.
Had the study been longer than six weeks, perhaps more of
the MSIs would have failed.
predicted, however.
This cannot be accurately
Second, it is possible that the
displacement occurred early (i.e., during the first four
weeks) in the study, and were retained by the applied
forces until healing occurred (secondary stability).
Because success was defined as lack of MSI pullout,
the displaced MSIs were considered successful.
Some MSI
displacement may be permissible as long as the treatment
objectives are being met.21,23
A tangentially-applied load
may actually help bind the MSI in the bone, compensating
for some degree of mobility.
Furthermore, once bony
healing establishes secondary stability, mobility may
74
actually be reduced.
This observation has been reported in
the literature.24
There was no significant correlation between initial
Periotest mobility and success or failure of MSIs, or
eventual displacement of experimental MSIs.
Some
relationship between initial Periotest mobility and success
or failure was expected.
The validity of the Periotest,
when used with miniscrew implants, is therefore
questionable.
Further research regarding this question is
warranted.
The success rates of 3 mm experimental MSIs placed in
the mandible were 20% lower than those placed in the
maxilla.
While this difference was not statistically
significant, other authors have also demonstrated lower
success rates in the mandible.25-28
Mandibular bone is
denser than maxillary bone,29 and density may affect success
rates of MSIs.
All six of the failed MSIs that were found
to have sheared tips had been placed in the mandible.
It
appears that the increased torque required to place a selfdrilling MSI through dense bone may, in some cases, alter
MSI integrity and lead to material failure.
This
observation may support the practice of pre-drilling MSI
sites in the mandible.
75
This study was limited by the shearing of several of
the MSIs, as well as the behavior of dog #3.
A longer
study period could have provided more information regarding
the stability of 3 mm MSIs over an extended time.
The
major limitation of the present study, however, was a lack
of power.
The limited number of MSIs compared makes it
impossible to say that the force level applied or placement
location play no role in stability.
As such, an increased
sample size would likely have allowed for a more meaningful
interpretation of the results.
Conclusions
1. Overall, success rates of immediately-loaded 3 mm MSIs
were significantly lower than those of immediatelyloaded 6 mm MSIs.
After exclusions, however, the
difference was not statistically significant.
2. The difference in success rates between 3 mm
mandibular MSIs loaded with 600g or 900g of force was
not significant.
3. Both 3 mm and 6 mm MSIs immediately-loaded with 600 or
900g of force experienced significant amounts of
linear displacement during the course of the study.
76
4. There was no relationship between initial mobility and
success or failure of MSIs, or eventual displacement
of experimental MSIs.
5. Further research involving the effects of length on
MSI stability is indicated.
Acknowledgements
The authors wish to acknowledge Drs. George Vogler and
Heidi Israel for their assistance during this project, and
the support of Dentos, Inc.
This research was supported by
the Saint Louis University Orthodontic Education and
Research Foundation.
References
1. Sinha PK, Nanda RS. Improving patient compliance in
orthodontic practice. Semin Orthod 2000;6:237-241.
2. Gray JB, Steen ME, King GJ, Clark AE. Studies on the
efficacy of implants as orthodontic anchorage. Am J Orthod
1983;83:311-317.
3. Odman J, Lekholm U, Jemt T, Branemark PI, Thilander B.
Osseointegrated titanium implants--a new approach in
orthodontic treatment. Eur J Orthod 1988;10:98-105.
4. Rasmussen R. A new dimension--implant-assisted
orthodontics. Dent Implantol Update 1991;2:24-26.
77
5. Thilander B, Odman J, Grondahl K, Friberg B.
Osseointegrated implants in adolescents. An alternative to
replacing teeth? Eur J Orthod 1994;16:84-95.
6. Turley PK, Kean C, Schur J, Stefanac J, Gray J, Hennes J
et al. Orthodontic force application to titanium endosseous
implants. Angle Orthod 1988;58:151-162.
7. Spear FM, Mathews DM, Kokich VG. Interdisciplinary
management of single-tooth implants. Semin Orthod
1997;3:45-72.
8. Crismani AG, Bernhart T, Bantleon HP, Cope JB. Palatal
implants: the Straumann Orthosystem. Semin Orthod
2005;11:16-23.
9. Block MS, Hoffman DR. A new device for absolute
anchorage for orthodontics. Am J Orthod Dentofacial Orthop
1995;107:251-258.
10. Janssens F, Swennen G, Dujardin T, Glineur R, Malevez
C. Use of an onplant as orthodontic anchorage. Am J Orthod
Dentofacial Orthop 2002;122:566-570.
11. Herman RJ, Currier GF, Miyake A. Mini-implant anchorage
for maxillary canine retraction: a pilot study. Am J Orthod
Dentofacial Orthop 2006;130:228-235.
12. Thiruvenkatachari B, Pavithranand A, Rajasigamani K,
Kyung HM. Comparison and measurement of the amount of
anchorage loss of the molars with and without the use of
implant anchorage during canine retraction. Am J Orthod
Dentofacial Orthop 2006;129:551-554.
13. Owens SE. Experimental evaluation of tooth movement in
the beagle dog utilizing the mini-implant for orthodontic
anchorage. Master's Thesis. Baylor College of Dentistry.
Dallas, TX. 2004.
78
14. Carillo R. Intrusion and root resorption of
multiradicular teeth using mini-screw implants as
anchorage. Master's Thesis. Baylor College of Dentistry.
Dallas, TX. 2004.
15. Doi PAK. A comparison of stability of immediately
loaded mini-implants with two different force levels in the
beagle dog. Master's Thesis. Center for Advanced Dental
Education. Saint Louis University. St. Louis, MO. 2006.
16. Asikainen P, Klemetti E, Vuillemin T, Sutter F, Rainio
V, Kotilainen R. Titanium implants and lateral forces. An
experimental study with sheep. Clin Oral Implants Res
1997;8:465-468.
17. Ohmae M, Saito S, Morohashi T, Seki K, Qu H, Kanomi R
et al. A clinical and histological evaluation of titanium
mini-implants as anchors for orthodontic intrusion in the
beagle dog. Am J Orthod Dentofacial Orthop 2001;119:489497.
18. Kim JW, Ahn SJ, Chang YI. Histomorphometric and
mechanical analyses of the drill-free screw as orthodontic
anchorage. Am J Orthod Dentofacial Orthop 2005;128:190-194.
19. Akin-Nergiz N, Nergiz I, Schulz A, Arpak N, Niedermeier
W. Reactions of peri-implant tissues to continuous loading
of osseointegrated implants. Am J Orthod Dentofacial Orthop
1998;114:292-298.
20. Caraway DM. Shear force at failure of immediatelyloaded 3 mm and 6 mm miniscrew implants at six weeks postinsertion. Master's Thesis. Center for Advanced Dental
Education. Saint Louis University. St. Loouis, MO. 2007.
21. Pickard MB. Effect of mini-screw orthodontic anchorage
implant orientation on implant stability and resistance to
failure at the bone-implant interface. Master's Thesis.
Baylor College of Dentistry. Dallas, TX. 2004.
79
22. Huja SS, Litsky AS, Beck FM, Johnson KA, Larsen PE.
Pull-out strength of monocortical screws placed in the
maxillae and mandibles of dogs. Am J Orthod Dentofacial
Orthop 2005;127:307-313.
23. Liou EJ, Pai BC, Lin JC. Do miniscrews remain
stationary under orthodontic forces? Am J Orthod
Dentofacial Orthop 2004;126:42-47.
24. Roberts WE, Marshall KJ, Gongloff RK. Rigid endosseous
implants for orthodontic and orthopedic anchorage. Angle
Orthod 1989;59:247-256.
25. Park HS, Jeong SH, Kwon OW. Factors affecting the
clinical success of screw implants used as orthodontic
anchorage. Am J Orthod Dentofacial Orthop 2006;130:18-25.
26. Tseng YC, Hsieh CH, Chen CH, Shen YS, Huang IY, Chen
CM. The application of mini-implants for orthodontic
anchorage. Int J Oral Maxillofac Surg 2006;35:704-707.
27. Cheng SJ, Tseng IY, Lee JJ, Kok SH. A prospective study
of the risk factors associated with failure of miniimplants used for orthodontic anchorage. Int J Oral
Maxillofac Implants 2004;19:100-106.
28. Deguchi T, Takano-Yamamoto T, Kanomi R, Hartsfield JK,
Jr., Roberts WE, Garetto LP. The use of small titanium
screws for orthodontic anchorage. J Dent Res 2003;82:377381.
29. Park HS, Lee YJ, Jeong SH, Kwon TG. Bone density of the
alveolar and basal bone in the maxilla and the mandible. Am
J Orthod Dentofacial Orthop. In press 2006.
80
Figures
Fig 3.1.
3 mm and 6 mm MSIs
81
Dogs 1 & 3
xxxxxx
xxxx
x
600g
600g
900g
600g
Maxillary
Mandibular
3mm experimental implant
6mm experimental implant
Control implant (same length as adjacent experimental implants)
Dogs 2, 4 & 5
xxxxxx
xxxxxx
600g
900g
600g
600g
Maxillary
Mandibular
3mm experimental implant
6mm experimental implant
Control implant (same length as adjacent experimental implants)
Fig 3.2. MSI placement locations and
force levels applied
82
5 Dogs
N=60 Implants
(12 per dog)
3 mm N=45
(9 per dog)
Experimental
N=30 (6 per dog)
600g of force
N=20 (4 per dog)
6 mm N=15
(3 per dog)
Control N=15
(3 per dog)
900g of force
N=10 (2 per dog)
Experimental
N=10 (2 per dog)
600g of force
N=10 (2 per dog)
Control N=5
(1 per dog)
900g of force
N=0 (0 per dog)
83
Maxilla N=10
(2 per dog)
Mandible N=20
(4 per dog)
Maxilla N=10
(2 per dog)
Mandible N=0
(0 per dog)
0g force
N=15 (3 per dog)
Maxilla N=5
(1 per dog)
Mandible N=10
(2 per dog)
Fig 3.3. Experimental design outline.
0g force
N=5 (1 per dog)
Maxilla N=5
(1 per dog)
Mandible N=0
(0 per dog)
B
A
B
84
C
Fig 3.4. Scanning electron microscope images of MSIs:
sheared during placement; C, sheared 3 mm MSI.
A, virgin MSI; B, 6 mm MSI that
C
Stability (percent)
100
Primary
Stability
Secondary
Stability
Total
Stability
75
50
25
0
0
1
2
3
4
5
6
7
8
Time (weeks)
Fig 3.5. Stability Patterns of Endosseous Dental
Implants (Adapted from Raghavendra, Wood, and Taylor)
85
3
∆
*
2
∆
*
1
∆
0
*
∆
∆
* *
*
*
*
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
86
Number of failed implants
4
Day of failure
Control
Experimental
Fig 3.6. Failure times for 3 mm MSIs. ∆ indicates an MSI that was
found to be sheared. * indicates an MSI that was placed in dog #3.
Table 3.1. Success rates of MSIs by length
Length
Number
failed that
were
sheared
Success
rate
excluding
sheared
implants
Number
failed from
dog #3
Success
rate
excluding
sheared
implants
and dog #3
Number
placed
Number
failed
Overall
success rate
3 mm
30
10
66.7%
(20/30)
5
80%
(20/25)
6
95.2%
(20/21)
6 mm
10
0
100%
(10/10)
0
100%
(10/10)
0
100%
(8/8)
3 mm
15
5
66.7%
(10/15)
1
71.4%
(10/14)
2
81.8%
(9/11)
6 mm
5
0
100%
(5/5)
0
100%
(5/5)
0
100%
(4/4)
3 mm
45
15
66.7%
(30/45)
6
76.9%
(30/39)
8
90.6%
(29/32)
6 mm
15
0
100%
(15/15)
0
100%
(15/15)
0
100%
(12/12)
Experimental MSIs
Total
Tables
87
Control MSIs
Table 3.2 Success rates of 3 mm MSIs by location
Length
Number
Placed
Number
Failed
Overall
success rate
Number of
failed
implants
that were
sheared
10
2
80% (8/10)
0
80% (8/10)
2
100% (8/8)
5
1
80% (4/5)
0
80% (4/5)
1
100% (4/4)
15
3
80% (12/15)
0
80% (12/15)
3
100%
(12/12)
20
8
60% (12/20)
5
80% (12/15)
4
85.7%
(12/14)
10
4
60% (6/10)
1
66.7% (6/9)
1
71.4% (5/7)
30
12
60% (18/30)
6
75% (18/24)
5
81% (17/21)
Success rate
excluding
sheared
implants
Number of
failed
implants
from dog #3
Success rate
excluding
sheared
implants
and dog #3
Maxilla
Experimental MSIs
3 mm
Control MSIs
88
3 mm
Total
3 mm
Mandible
Experimental MSIs
3 mm
Control MSIs
3 mm
Total
3 mm
Table 3.3. Success rates of mandibular MSIs by force level applied
Length
Number
Placed
Number
Failed
Overall
success rate
Number of
failed
implants
that were
sheared
10
4
60% (6/10)
3
85.7% (6/7)
2
100% (6/6)
10
4
60% (6/10)
2
75% (6/8)
2
85.7% (6/7)
Success rate
excluding
sheared
implants
Number of
failed
implants
from dog #3
Success rate
excluding
sheared
implants
and dog #3
900g Load
89
3 mm
600g Load
3 mm