Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
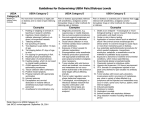
Depressive Symptoms in Primary Care: Recognition and Assessment Sudha Prathikanti, MD UCSF Department of Psychiatry Primary Care Statistics • Depressive symptoms the most common outpatient medical problem • Depression 10-25% vs HTN 6% • On average, medical resident should encounter at least 1 patient with depressive symptoms each clinic day • Not all depressive symptoms lead to MDD, but all require some management Costs of Untreated MDD • Untreated depressed patients use 2-3 times more medical services (e.g MD visits) • Untreated depressed patients spend more time in bed than those with chronic medical probs like IDDM, arthritis, COPD, GI disease • Risk of suicide (6% to 15% lifetime risk) 25% of suicide completers visit PMD before dying 50% of suicide completers visit PMD month before dying 1 wk 1 Recognition of Depressive Sx • Maintain high index of suspicion • Evaluate somatic complaints By type By number • Look for irritability/behavior change • Use screening questionnaires Beck (21 questions) mod. depress >16 Carroll (20 questions) mod. depress >19 Assessing Severity of Depressive Symptoms • Increased severity correlates with increased risk of threshold psychiatric disorder • Triage of symptom severity PAT : pt needs assurance & talk PAM : pt needs more assessment & management PIT : pt needs immediate treatment (usually psychiatry consult) Assessing Severity 1) Level of Overall Distress Ask patient to quantify on scale of 1-10 Use screening questionnaire PAT : lower distress PAM : moderate distress PIT : higher distress Assessing Severity 2) Identifiable Stressor (not always present) Acute Major (death, divorce) Minor (fender-bender, job deadline) Chronic Major (ongoing illness, marital conflict) Minor (noisy neighbor, long commute) PAT: distress commensurate with stressor, shows adaptation over time PAM: disproportionate distress, difficulty adapting PIT : disproportionate distress, unsafe adapting Assessing Severity 3) Functional Impairment Social withdrawal Impaired job performance Impaired parenting Relational difficulties Self-care problems PAT: less social, longer time to complete tasks PAM: impaired parenting/job performance PIT: self-care/self-preservation becomes issue Assessing Severity 4) Duration of Symptoms Days Weeks (2) Months (2-3) Years (2) PAT: mostly days PAM: mostly 2 weeks to 2-3 months PIT: mostly days, but any of above Assessing Severity 5) Always ask about Suicidal Ideation (esp if psychosis or substance abuse present) Active vs. passive Persistent vs. fleeting Intractable vs. distractable Specific vs. vague Means vs. no means Impulse to enact vs. no impulse Actual attempt vs. no attempt PAT: no suicidal ideation PAM: may be present, but usually passive/fleeting PIT: present, and active/persistent/intractable/specific