Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
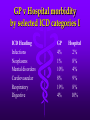
GP 4001 Lecture Series 2007-2008 1. Introduction What I plan to cover today • Learning outcomes for the course • Evaluation and assessment of this course • How general practice differs from hospital medicine • Nature and scope of general practice Learning Outcomes for this course - I • Develop a rapport with patients such that patients are at ease in discussing their health problem(s) (comm) • Gather appropriate information on the patient’s health problem(s) including information on the patient’s own perspective on the problem(s). (udp, comm) • Generate a reasonable range of diagnostic possibilities for undifferentiated medical problems presented by patients (udp) • Investigate these diagnostic possibilities using appropriately focused history taking and selective physical examination (udp, comm) Learning Outcomes for this course - II • Construct a general model for the safe and effective management of patients with multiple and long term health problems (cdm) • Adapt this model to the long term health problems commonly encountered by doctors (cdm) • Construct an appropriate and feasible management plan to deal with the physical, psychological and social aspects of patient’s problem(s) (udp, cdm) • Negotiate this plan with the patient. (comm) Learning Outcomes – three principal domains • Dealing with undifferentiated problems presented by patients (udp) • Management of chronic ill health (cdm) • Communication (comm) Assessment and Evaluation • Assessment • End of year exam – MEQ format • GP attachment assessment by GP tutor • Diagnostic thinking • Patient management • Attitudes to patients and staff • Responsiveness to teaching and enthusiasm for learning • Evaluation • Will be asked to complete an on-line evaluation by MarkClass • In class evaluation exercises throughout the year How general practice differs from hospital medicine I - the nature of illness seen • General Practice • non-illness & disorganised illness • acute self-limiting • chronic stable • all age groups • mixed physical, psychological and social • Hospital • nearly all clear cut disease • acute life threatening • acute-on-chronic • categorised by age • physical and psychologial divided virtually no social GP v Hospital morbidity by selected ICD categories I ICD Heading GP Hospital Infections Neoplasms Mental disorders Cardiovascular Respiratory Digestive 4% 1% 10% 8% 19% 4% 2% 8% 4% 9% 8% 10% GP v Hospital morbidity by selected ICD categories II ICD Heading GP Hospital Genito-urinary Childbirth & pregnancy Skin conditions Musculo-skeletal Symptoms & ill-defined conditions Accidents 5% 10% 6% 7% 8% 8% 19% 2% 3% 6% 5% 10% Spectrum of morbidity in General Practice 15% Minor Intermediate Major 53% 32% Bio-psycho-social diagnosis (a.k.a. ‘tri-axial diagnosis’) • Diagnosis in • physical • psychological • and social terms • Note - not either/ or but degrees of each • A manifestation of ‘holistic’ medicine non-reductionist • Philosophically breaking down Cartesian dualism - the ‘mind-body split’ Common problems seen in general practice - Physical • Respiratory tract - colds, flu, asthma, bronchitis • Gastro-intestinal tract - D&V, gastroenteritis, peptic ulcer, irritable bowel • Cardiovascular - IHD, hypertension • Musculoskeletal - backache, OA, soft tissue • Endocrine - diabetes, thyroid disease • Genito-urinary - cystitis, STDs Common problems seen in general practice - Psychological • Adjustment reactions e.g. grief reaction • Anxiety • Depression • Mixed anxiety-depression • Drug and alcohol problems • Chronic stable schizophrenia • Post-traumatic stress disorder Common problems seen in general practice -Social • Relationship difficulties • Job dissatisfaction • Effects of poor housing • Effects of unemployment/ social deprivation • Lack of education How general practice differs from hospital medicine II - Organisation • General Practice • small units, noninstitutional • non-hierarchical teams • low tech • easily accessible • Hospital • large institutional units • highly hierarchical teams • high tech • filtered access Levels of care location of care Regional Hospital General hospital General practitioner Self care People looked after 1,000,000 20,000 2,000 5 The illness ice-berg MAJOR ILLNESS MINOR ILLNESS SELF-CARE PRE-SYMPTOMATIC DISEASE HEALTH The ‘gate-keeper function’ • Controls access to more expensive secondary care resources • Necessary (essential) for costcontainment • Appropriate specialist selected for patients who need one • Avoidance of hazards of specialist care for patients who don’t need it • Maintenance of skills of specialists The ‘amoeba’ that is general practice (after Metcalfe, David) SOCIETY PRIMARY CARE HOSPITAL •ageing Capital intensive Low capital •increasing chronic morbidity Labour intentsive Lean manpower •declining family ties •changing attitudes to NonHierarchical professionals hierarchical •polico-economic change Stiff interface •ecological change Fluid interface Recommended Textbooks • Pocket Essentials of General Practice by Colin Bradley Saunders/ Elsevier ISBN 13-978-0-7020-2648-5 • A Textbook of Family Medicine by Ian R. McWhinney Pub Oxford Medical ISBN 0-19-515518-X • General Practice by John Murtagh McGraw-Hill Education ISBN: 0074711776