Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
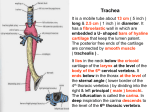
Dr. Mujahid Khan The trachea is a mobile cartilaginous and membranous tube It begins in the neck as a continuation of the larynx at the lower border of the cricoid cartilage at the level of the sixth cervical vertebra It descends in the midline of the neck In the thorax the trachea ends below at the carina by dividing into right and left principal (main) bronchi During expiration the bifurcation rises by about one vertebral level During deep inspiration may be lowered as far as the sixth thoracic vertebra In adults the trachea is about 4½ in. (11.25 cm) long and 1 in. (2.5 cm) in diameter The fibroelastic tube is kept patent by the presence of U-shaped rings of hyaline cartilage embedded in its wall The posterior free ends of the cartilage are connected by smooth muscle, the trachealis muscle Anteriorly: The sternum, the thymus, the left brachiocephalic vein, the origins of the brachiocephalic and left common carotid arteries, and the arch of the aorta Posteriorly: The esophagus and the left recurrent laryngeal nerve Right side: The azygos vein, the right vagus nerve, and the pleura Left side: The arch of the aorta, the left common carotid and left subclavian arteries, the left vagus and left phrenic nerves, and the pleura The upper two thirds are supplied by the inferior thyroid arteries The lower third is supplied by the bronchial arteries The lymph drains into the pretracheal and paratracheal lymph nodes and the deep cervical nodes The sensory nerve supply is from the vagi and the recurrent laryngeal nerves Sympathetic nerves supply the trachealis muscle The trachea bifurcates behind the arch of the aorta into the right and left principal (primary, or main) bronchi The bronchi divide into several million terminal bronchioles that terminate in one or more respiratory bronchioles Each respiratory bronchiole divides into 2 to 11 alveolar ducts that enter the alveolar sacs The alveoli arise from the walls of the sacs as diverticula Is wider, shorter, and more vertical than the left Is about 1 in. (2.5 cm) long Before entering the hilum of the right lung, it gives off the superior lobar bronchus On entering the hilum, it divides into a middle and an inferior lobar bronchus Is narrower, longer, and more horizontal than the right and is about 2 in. (5 cm) long It passes to the left below the arch of the aorta and in front of the esophagus On entering the hilum of the left lung, the principal bronchus divides into a superior and an inferior lobar bronchus Two lungs are soft, spongy and elastic In the child, they are pink, but with age, they become dark and mottled because of the inhalation of dust particles These particles are trapped in the phagocytes of the lung The lungs are situated so that one lies on each side of the mediastinum Two lungs are separated from each other by the heart and great vessels and other structures in the mediastinum Each lung is conical, covered with visceral pleura and suspended free in its own pleural cavity Attached to the mediastinum only by its root A blunt apex projects upward into the neck for about 1 in. (2.5 cm) above the clavicle A concave base that sits on the diaphragm A convex costal surface, which corresponds to the concave chest wall A concave mediastinal surface, which is molded to the pericardium and other mediastinal structures Hilum is a depression in which the bronchi, vessels, and nerves that form the root enter and leave the lung The anterior border is thin and overlaps the heart It is here on the left lung that the cardiac notch is found The posterior border is thick and lies beside the vertebral column The right lung is slightly larger than the left Divided by the oblique and horizontal fissures into three lobes: upper, middle, and lower The oblique fissure runs from the inferior border upward and backward across the medial and costal surfaces until it cuts the posterior border about 2.5 in. (6.25 cm) below the apex The left lung is divided by a similar oblique fissure into two lobes: upper and lower There is no horizontal fissure in the left lung The bronchopulmonary segments are the anatomic, functional, and surgical units of the lungs Each lobar (secondary) bronchus gives off branches called segmental (tertiary) bronchi Each segmental bronchus passes to a structurally and functionally independent unit of a lung lobe called a bronchopulmonary segment, surrounded by connective tissue The segmental bronchus is accompanied by a branch of the pulmonary artery Each segment has its own lymphatic vessels and autonomic nerve supply On entering a bronchopulmonary segment, each segmental bronchus divides repeatedly As the bronchi become smaller, the U-shaped bars of cartilage found in the trachea are gradually replaced by irregular plates of cartilage The smallest bronchi divide and give rise to bronchioles, which are less than 1 mm in diameter Bronchioles possess no cartilage in their walls and are lined with columnar ciliated epithelium The submucosa possesses a complete layer of circularly arranged smooth muscle fibers The bronchioles then divide and give rise to terminal bronchioles which show delicate outpouchings from their walls Gaseous exchange between blood and air takes place in the walls of these outpouchings, which explains the name respiratory bronchiole The diameter of a respiratory bronchiole is about 0.5 mm The respiratory bronchioles end by branching into alveolar ducts, which lead into tubular passages with numerous thin-walled outpouchings called alveolar sacs The alveolar sacs consist of several alveoli opening into a single chamber Each alveolus is surrounded by a rich network of blood capillaries Gaseous exchange takes place between the air in the alveolar lumen through the alveolar wall into the blood within the surrounding capillaries It is a subdivision of a lung lobe It is pyramid shaped, with its apex toward the lung root It is surrounded by connective tissue It has a segmental bronchus, a segmental artery, lymph vessels, and autonomic nerves The segmental vein lies in the connective tissue between adjacent bronchopulmonary segments Because it is a structural unit, a diseased segment can be removed surgically Superior lobe: Apical, posterior, anterior Middle lobe: Lateral, medial Inferior lobe: Superior (apical), medial basal, anterior basal, lateral basal, posterior basal Superior lobe: Apical, posterior, anterior, superior lingular, inferior lingular Inferior lobe: Superior (apical), medial basal, anterior basal, lateral basal, posterior basal The bronchi and the connective tissue of the lung receive their blood supply from the bronchial arteries, which are branches of the descending aorta The bronchial veins communicate with the pulmonary veins and drain into the azygos and hemiazygos veins The alveoli receive deoxygenated blood from the terminal branches of the pulmonary arteries The oxygenated blood leaving the alveolar capillaries drains into the tributaries of the pulmonary veins Two pulmonary veins leave each lung root to empty into the left atrium of the heart The lymph vessels originate in superficial and deep plexuses They are not present in the alveolar walls The superficial (subpleural) plexus lies beneath the visceral pleura and drains over the surface of the lung toward the hilum, where the lymph vessels enter the bronchopulmonary nodes The deep plexus travels to the hilum of the lung and enters the bronchopulmonary nodes All the lymph from the lung leaves the hilum and drains into the tracheobronchial nodes and then into the bronchomediastinal lymph trunks At the root of each lung is a pulmonary plexus composed of efferent and afferent autonomic nerve fibers The plexus is formed from branches of the sympathetic trunk and receives parasympathetic fibers from the vagus nerve The sympathetic efferent fibers produce bronchodilatation and vasoconstriction The parasympathetic efferent fibers produce bronchoconstriction, vasodilatation, and increased glandular secretion