Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
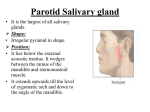
Sialography Spring 2009 DRAFT Salivary Glands Parotid Gland Sublingual gland Submandibular gland Parotid Gland Largest of the glands Consists of flattened superficial portion and wedge shaped deep portion Parotid duct – Conduct saliva from gland to the mouth Submandibular Gland Irregularly shaped Extends posteriorly from first molar to almost angle of mandible Sublingual Gland Smallest pair Located at floor of mouth beneath sublingual fold In contact with the mandible laterally Extends posteriorly from the side of frenulum to submandibular duct Main sublingual duct opens beside the orifice of the submandibular duct Sialography Term applied to radiographic exam of salivary glands – Only one gland done at a time – CT and MRI have largely replaced this exam for Salivary stone or lesion is suspected – Used when a definitive diagnosis is necessary for a problem with one of the salivary ducts Indications Tumors Inflammatory lesions Determine extent of salivary fistulae Localize diverticulae strictures and calculi Salivary duct obstruction Clinical Symptoms Clinical Symptoms Sialogram Tray and Catheter Procedure 1. Obtain preliminary radiographs • • Any condition that is visibe w/o contrast Optimum technique obtained 2. 2-3 min before procedure give patient lemon 3. Contrast media injected into main duct 4. After procedure suck on lemon to clear contrast 5. 10 min after procedure take radiograph Procedure Differences 1. Most manually inject contrast – Using cannula or catheter 2. Others use hydrostatic pressure – Contrast solution barrel plunger removed – Attached to drip stand – 28” above pt’s mouth 3. Some inject under fluoro and obtain spot radiographs Radiation Safety Have shields for PT’s, DR and yourself Question LMP and the possibility of being pregnant Use cardinal rules – Time – Distance – Shielding ALARA – Use pulse if possible – Save the last image on screen when possible Tangential Supine Rotate pt head toward side being examined so that parotid gland is perp to plane of IR Rest head on occipitus Center IR to parotid area Mandibular ramus parallel with longitudinal axis of the IR Fill mouth with air and puff cheeks CR perp to plane of IR along lateral surface of the ramus Rotate pt’s head away from side being examined Rest pt’s head on chin – Forehead and nose if parotid duct does not need to be seenRotate pt head toward side being examined so that parotid gland is perp to plane of IR Center IR to parotid area Mandibular ramus parallel with longitudinal axis of the IR Fill mouth with air and puff cheeks CR perp to plane of IR along lateral surface of the ramus Tangential Prone Tangential Radiograph Soft tissue dentisy Most of parotid gland lateral to and clear of ramus Mastoid overlapping only the upper portion of parotid gland Affected side close to the IR Extend mandible to clear c-spine Center IR 1” superior to angle Head 15 degrees from MSP toward IR CR 1” superior to angle Oblique often used as well Lateral Parotid Lateral Parotid Radiograph Mandibular Rami free from overlap of c-spine Parotid gland SI over the ramus Axiolateral oblique of mandible can be used Lateral Submandibular Center IR to inferior margin of angle PT head in true lateral CR at inferior margin of angle Lateral Submandibular Radiograph and Lateral oblique Rami free from overlap of C-spine SI mandibular rami if no angualtion is used Axiolateral oblique of mandible for better demonstration Axiolateral Oblique for Submandibular Review A A E B C REVIEW A B E C F D